










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 no.6 Madrid jun. 2010
CARTAS AL DIRECTOR
Dieulafoy's lesion in a duodenal diverticulum successfully treated with N-butyl-2-cyanoacrylate
Lesión de Dieulafoy en un divertículo duodenal tratado con éxito con N-butil-2-cianoacrilato
Palabras clave: Lesión de Dieulafoy. N-butil-2-cianoacrilato. Duodeno.
Key words: Dieulafoy's lesion. N-butyl-2-cyanocrylate. Duodenum.
Dear Editor,
Duodenal diverticula (DD) are usually asymptomatic and are an uncommon source of gastrointestinal bleeding.
Dieulafoy's lesion is an often unrecognized cause of catastrophic upper gastrointestinal hemorrhage, typically seen in an otherwise asymptomatic patient. The lesion is most often found in the proximal stomach and has rarely been reported to occur in the duodenum, and even rarely within a duodenal diverticulum.
Case report
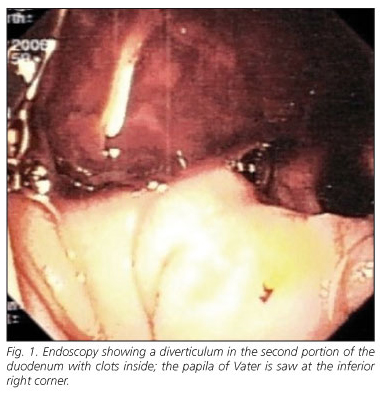
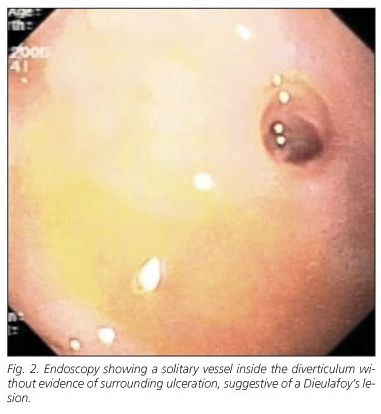
We report the case of a 75-year-old man that was admitted to our emergency department with a 2-day history of hematochezia. Past medical history was significant for alcoholic liver cirrhosis. At admission, blood pressure was 86/45 mmHg, pulse rate 98 beats/minute, hemoglobin 7,3 g/dL, platelets 112,000/mm3 and INR 1.46. Emergency upper endoscopy revealed esophageal varices grade I (with no signs of recent bleeding) and fresh blood in the stomach and duodenum. It was not possible to identify the source of the hemorrhage. The following day, repeated endoscopy showed a diverticulum in the second portion of the duodenum with clots and a solitary vessel inside it without evidence of surrounding ulceration, suggestive of a Dieulafoy's lesion (Figs. 1 and 2). It was treated with 4 ml of a 1:10,000 epinephrine solution and 1 ml of fibrin glue. Two days later, the patient presented hematochezia, fresh blood on the nasogastric tube, hypotension and a decrease in hemoglobin from 10.7 g/dL to 8.8 g/dL. Endoscopy revealed persistence of the vessel, which was treated with 0.8 cc of N-butyl-2-cyanoacrylate/lipiodol moisture (0.5/0.3 cc). A plain abdominal film showed a opacity localized at the injection point (Fig. 3). No further bleeding occurred. A third endoscopy, performed 7 days after the procedure, showed no lesions. The patient has not rebled after 2 years of follow-up.

Discussion
Bleeding from a duodenal diverticulum is an uncommon event (1); although endoscopy has changed dramatically the diagnosis and treatment of this condition, experience is still limited due to its rarity.
Dieulafoy's lesion is an important cause of bleeding in which massive hemorrhage occurs from an unusually large, tortuous submucosal artery. In most cases, this lesion is found in the proximal stomach within 6 cm of the gastroesophageal junction, being rare similar lesions in the duodenum. A multiplicity of endoscopic methods have been used to achieve definitive hemostasis, namely injection, thermal or mechanical methods (2,3). Chung et al. reported that mechanical therapy, such as hemoclipping or band ligation, was superior to injection therapy for bleeding Dieulafoy's lesions (4).
N-butyl-2-cyanoacrylate is an effective option for treating variceal bleeding, but also a good alternative for bleeding ulcers (5), although cases of intraabdominal embolization have been reported (6). It was successfully used to treat gastric Dieulafoy's lesions (3,7), but no duodenal ones.
Only a few cases of Dieulafoy's lesions within a DD have been published (1,8); treatment of this condition may bring additional difficulties due to the narrow stoma of the diverticulum and the thin wall, which can limit the use of mechanical methods and enhance the rate of complications. A case of perforation was reported following hemoclipping (9).
We believe that N-butyl-2-cyanoacrylate is a safe and effective alternative therapy, especially in high risk patients; a low injection volume may minimize the risk of intraabdominal embolization.
A. Sadio, P. Peixoto, A. Castanheira, E. Cancela, P. Ministro, A. Silva and A. Caldas
Department of Gastroenterology. São Teotónio Hospital. Viseu, Portugal
References
1. Chen YY, Yen HH, Soon MS. Impact of endoscopy in the management of duodenal diverticular bleeding: experience of a single medical center and a review of recent literature. Gastrointest Endosc 2007; 66: 831-5. [ Links ]
2. Romãozinho JM, Pontes JM, Lérias C, et al. Dieulafoy's lesion: management and long term outcome. Endoscopy 2004; 36: 653-6. [ Links ]
3. Cheng CL, Lui NJ, Lee CS, et al. Endoscopic management of Dieulafoy lesions in acute nonvariceal upper gastrointestinal bleeding. Dig Dis Sci 2004; 49: 1139-44. [ Links ]
4. Chung IK, Kim EJ, Lee MS, et al. Bleeding Dieulafoy's lesions and the choice of endoscopic method: comparing the hemostatic efficacy of mechanical and injection methods. Gastrointest Endoscopy 2000; 52: 721-4. [ Links ]
5. Kok KYY, Kum CK, Goh PMY. Endoscopic hemostasis of upper gastrointestinal bleeding with Histoacryl: last resort before surgery. Endoscopy 1996; 28: 256-8. [ Links ]
6. Lee GH, Kim JH, Lee KJ, et al. Life-threatening intrabdominal arterial embolization after histoacryl injection for bleeding gastric ulcer. Endoscopy 2000; 32: 422-4. [ Links ]
7. Loperfido S. Endoscopic hemostasis of gastric bleeding from Dieulafoy's ulcer with Histoacryl. Endoscopy 1989; 21: 199-200. [ Links ]
8. Lee BI, Kim BW, Choi H, et al. Hemoclip placement through a forward-viewing endoscope for a Dieulafoy-like lesion in a duodenal diverticulum. Gastrointest Endosc 2003; 58: 813-4. [ Links ]
9. Ko KH, Lee SY, Hong SP, et al. Duodenal perforation after endoscopic hemoclip application for bleeding from Dieulafoy's lesion in a duodenal diverticulum. Gastrointest Endosc 2005; 62: 781-2. [ Links ]

