










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 no.7 Madrid jul. 2011
https://dx.doi.org/10.4321/S1130-01082011000700010
Mutations in HFE and TFR2 genes in a Spanish patient with hemochromatosis
Mutaciones en los genes HFE y TFR2 en un paciente español con hemocromatosis
Alejandro del-Castillo-Rueda1, Nuria Cuadrado-Grande2, Emilio Álvarez-Fernández3, Rafael Enríquez-de-Salamanca2, Luis Antonio Álvarez-Sala1 and María Josefa Morán-Jiménez2
1Unit of Ferropathology. Deparament of Internal Medicine. Hospital General Universitario Gregorio Marañón. Madrid, Spain.
2Centro de Investigación. Instituto de Investigación. Hospital 12 de Octubre. Madrid, Spain.
3Department of Pathology. Hospital General Universitario Gregorio Marañón. Madrid, Spain
Grant sponsors: "Fondo de Investigaciones Sanitarias" (FIS 07/0074), "Fundación Mutua Madrileña de Investigación Biomédica" (FMM 2007-73), and the Genomics Facility of the "Instituto de Investigación del Hospital 12 de Octubre", Spain.
ABSTRACT
Iron overload disease has a wide variety of genotypes. The genetic study of this disease confirms its hereditary nature and enables us to provide genetic counseling for first-degree relatives. We performed magnetic resonance imaging and liver biopsy in an asymptomatic patient with more than 1,000 µg/L of serum ferritin and studied the genes involved in this condition. The phenotype of iron overload is confirmed by a predominantly periportal pattern of iron deposits in the liver suggestive of genetic disease. In the case we present the molecular study revealed a double heterozygosity for the mutations c.187C>G (p.H63D) and c.840C>G (p.F280L) in the HFE and transferrin receptor 2 (TFR2) genes, respectively.
Key words: Hemochromatosis. HFE. Transferrin receptor 2.
RESUMEN
La enfermedad por sobrecarga de hierro está originada por diversas anomalías genéticas. El estudio genético de esta enfermedad confirma su carácter hereditario y nos permite ofrecer consejo genético a los familiares en primer grado. Hemos realizado resonancia magnética y biopsia de hígado en un paciente asintomático con más de 1.000 µg/l de ferritina en suero, y hemos analizado los genes implicados en el metabolismo del hierro. El fenotipo de sobrecarga de hierro se confirmó por la presencia de un patrón de depósito de hierro en el hígado con predominio periportal que sugiere la existencia de una enfermedad genética. En el caso que presentamos, el estudio genético reveló que el paciente es doble heterocigoto para las mutaciones c.187C>G (p.H63D) y c.840C>G (p.F280L) en los genes HFE y receptor 2 de transferrina (TFR2), respectivamente.
Palabras clave: Hemocromatosis. HFE. Receptor 2 de la transferrina.
Introduction
Clinicians have been aware of the clinical syndrome of hemochromatosis for more than 100 years; however, the most important advances in knowledge of this condition have occurred in the last two decades, especially with the discovery of the HFE gene (1). Hemochromatosis presents marked heterogeneity in genetic etiology, type of inheritance, environmental factors, and clinical and analytical manifestations (2-5).
Although the homozygous c.845G>A (p.C282Y) mutation in the HFE gene is responsible for the classic form of hereditary hemochromatosis, known as type 1 hemochromatosis, other genotypes, such as compound heterozygous c.845G>A (p.C282Y)/c.187C>G (p.H63D) in the HFE gene, are associated with iron overload (6). The heterozygous c.187C>G (p.H63D) mutation does not seem to be responsible for iron overload or hemochromatosis; therefore, it is necessary to analyze associated factors such as alcohol intake, hepatitis viruses, or mutations in genes involved in iron homeostasis (7,8). In rare cases, molecular abnormalities in the TFR2 and HFE genes in patients with iron overload are responsible for digenically inherited hemochromatosis (9,10).
Type 3 hemochromatosis is caused by mutations in the transferrin receptor 2 (TFR2) gene. The first cases were described in two Sicilian families with a homozygous c.750C>G (p.Y250X) mutation in this gene (11). TFR2 is homologous to TFR1, it is mainly expressed in liver, and the affinity of the TFR2 protein for transferrin is 30-fold higher than that of TFR1 (11). Patients with heterozygous mutations in the TFR2 gene do not have iron overload, unlike patients with heterozygous mutations in the HFE gene. The clinical manifestations of type 3 hemochromatosis are comparable to those of type 1, although there have been reports of more severe cases with earlier onset (12).
We report the case of a patient with mutations in HFE and TFR2 genes and a clinical phenotype of iron overload. This report confirms the genotypic and phenotypic heterogeneity of hemochromatosis.
Case report
A 50-year-old man with 2-year history of serum ferritin higher than 1,000 µg/L (normal range, 26-370) was referred to our department. He had increased ferritin (1,277 µg/L) and the γGT (116 U/L; normal range, 10-60) and ultrasonography of the liver led us to suspect fatty liver disease. Complementary analytical and serological testing revealed no abnormalities. The patient was asymptomatic. He had no toxic habits, and his personal/family history and physical examination were unremarkable.
We analyzed iron metabolism markers (serum levels of iron, ferritin, soluble transferrin receptor, and transferrin saturation) and hepatic iron and tissue architecture by liver biopsy. Magnetic resonance imaging (MRI) was performed and the allelic variations c.845G>A (p.C282Y) and c.187C>G (p.H63D) were identified in the HFE gene. Five-micrometer tissue sections were stained with hematoxylin and eosin and Perls Prussian blue to detect the presence of iron.
Genomic DNA was extracted from peripheral blood and polymerase chain reaction (PCR) was performed using specific oligonucleotides to amplify the entire coding regions, splice junctions and 5 ' and 3 ' untranslated regions (UTR) of the HFE, hemojuvelin (HJV), hepcidin (HAMP), TFR2 and ferroportin (SLC40A1) genes. PCR products were sequenced bidirectionally using the ABI Prism 3130x1 DNA sequencer and compared with the reference sequence (GenBank Accession numbers: NG_008720.1, NG_011568.1, NG_011563.1, NM_003227.3, and NG_009027.1, respectively, for the aforementioned genes).
Written informed consent was obtained according to local guidelines for the genetic study, liver biopsy, and iron challenge. The study protocol was in accordance with the ethical guidelines of the Declaration of Helsinki (2008).
The patient's iron parameters were as follows: serum ferritin, 1,070 µg/L (normal range, 26-370 µg/L); serum iron, 160 µg/dL (normal range, 59-158 µg/dL); transferrin saturation, 48% (normal range, 20-45%); and soluble transferrin receptor, 0.90 mg/L (normal range, 0.83-1.76 mg/L). Hepatic MRI showed diffuse intensity abnormalities in the parenchyma associated with an increase in iron; hepatic iron content was estimated to be 160 µmol/g (normal values < 36 µmol/g). Ultrasound-guided percutaneous liver biopsy was performed. Histopathologic evaluation showed normal lobular architecture, narrow portal spaces without inflammation or fibrosis, and no ductal or vascular lesions. The lobe was composed of hepatocytes with regular morphology and low-intensity hepatocellular hemosiderin deposits with the typical hemochromatosis pattern, namely, iron deposits located almost exclusively in the parenchymal cells in periportal areas with a granular pattern and a pericanicular distribution (Fig. 1).
The patient underwent phlebotomy, and, after 20 phlebotomies fortnightly, more than 5 g of iron were removed and these γGT and ferritin concentrations returned to normal values. The patient currently undergoes maintenance phlebotomy twice per year.
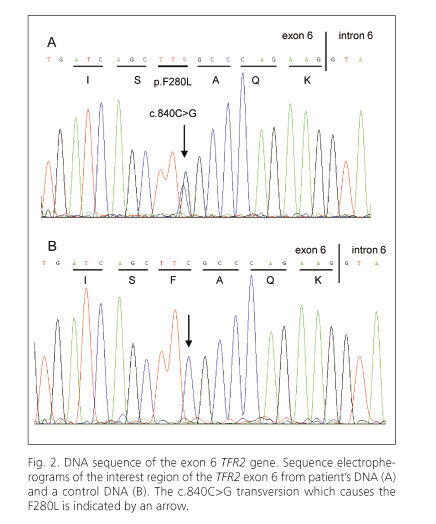
The molecular study of the genes involved in iron metabolism showed the following heterozygous allelic variants: c.187C>G (p.H63D) in the HFE gene and c.840C>G (p.F280L) in the TFR2 gene (Fig. 2).
Discussion
Hemochromatosis is a clinically and genetically heterogeneous disease caused by an inappropriate increase in intestinal absorption of iron. Although most patients are homozygous for the C282Y mutation in the HFE gene, genetic and environmental factors can modify the hemochromatosis phenotype. Patients with double heterozygous c.845G>A/c.187C>G (p.C282Y/p.H63D) mutations in the HFE gene showed a common phenotype of hemochromatosis, and a wide variety of clinical manifestations have been reported in patients with monogenically and digenically inherited mutations in other genes such as SLC40A1, TFR2, HJV, and HAMP (9,13).
Type 3 hemochromatosis is an unusual recessive disease caused by mutations in the TFR2 gene. This alteration has been described in a small group of Italo-French families, as well as in Japanese, Portuguese, and Scottish families, and it causes clinical hemochromatosis that is indistinguishable from type 1 hemochromatosis. However, diagnosis of type 3 hemochromatosis is made at a significantly younger age than type 1 hemochromatosis (12,14). Type 3 hemochromatosis is an intermediate syndrome between the typical adult type 1 hemochromatosis and two juvenile forms, type 2a and type 2b, which are caused by mutations in the HJV and HAMP genes; therefore, mutations in the TFR2 gene should be borne in mind in younger patients with adult-onset hemochromatosis (10,14,15).
The low level of circulating hepcidin, the hormone that controls intestinal iron absorption, is a common feature of type 1, 2, and 3 hemochromatosis (16). HFE, TFR2, and HJV are considered modulators of synthesis/activity of hepcidin, which in turn regulates the release of iron into blood from duodenal cells and macrophages, thus maintaining appropriate iron levels to satisfy the body's needs (17,18). The combination of mutations in the HFE and TFR2 genes and mutations in HAMP and HJV genes lead to more severe forms of hemochromatosis (due to a dysregulation in intestinal iron absorption), an increase of iron influx into the blood, and iron storage in tissues (10).
There are reports of type 3 hemochromatosis in patients with a heterozygous mutation in the TFR2 gene, and with or without mutations in the HFE gene. Mendes et al. (19) reported a case with heterozygous mutations, namely, c.187C>G in the HFE gene and c.840C>G in the TFR2 gene, and alcoholic habits, which are responsible for iron overload disease. This double heterozygosity was also observed in our patient, without toxic habits, who presented an iron overload phenotype confirmed by MRI and liver biopsy. The patient's condition was mild and responded to phlebotomy. Although we did not find relevant mutations in other genes studied in the patient (HJV, HAMP and SLC40A1), other environmental factors and modifiers genes might be involved in the hemochromatotic patients iron storage.
Early identification of patients with iron overload is very important for prognosis. Therefore, liver biopsy, measurements of the hepatic iron index, and a genetic study are necessary to clarify the diagnosis, classification, and treatment of patients with hemochromatosis.
References
1. Feder JN, Gnirke A, Thomas W, Tsuchihashi Z, Ruddy DA, Basava A, et al. A novel MHC class I-like gene is mutated in patients with hereditary haemochromatosis. Nat Genet 1996;13:399-408. [ Links ]
2. Bacon BR, Britton RS. Clinical penetrance of hereditary hemochromatosis. N Engl J Med 2008;358:291-2. [ Links ]
3. Barton JC, Lafreniere SA, Leiendecker-Foster C, Li H, Acton RT, Press RD, et al. HFE, SLC40A1, HAMP, HJV, TFR2, and FTL mutations detected by denaturing high-performance liquid chromatography after iron phenotyping and HFE C282Y and H63D genotyping in 785 HEIRS Study participants. Am J Hematol 2009;84:710-4. [ Links ]
4. Jorquera F, Dominguez A, Diaz-Golpe V, Espinel J, Muñoz F, Herrera A, et al. C282Y and H63D mutations of the haemochromatosis gene in patients with iron overload. Rev Esp Enferm Dig 2001;93:293-302. [ Links ]
5. Solis-Herruzo JA, Solis Muñoz P. Non-HFE hemochromatosis. Rev Esp Enferm Dig 2005;97:266-86. [ Links ]
6. Pietrangelo A. Inherited metabolic disease of the liver. Curr Opin Gastroenterol 2009;25:209-14. [ Links ]
7. Rochette J, Le Gac G, Lassoued K, Ferec C, Robson KJ. Factors influencing disease phenotype and penetrance in HFE haemochromatosis. Hum Genet 2010;128:233-48. [ Links ]
8. Ropero Gradilla P, Villegas Martinez A, Fernández Arquero M, García-Agúndez JA, González Fernández FA, Benítez Rodríguez, et al. C282Y and H63D mutations of HFE gene in patients with advanced alcoholic liver disease. Rev Esp Enferm Dig 2001;93:156-63. [ Links ]
9. Merryweather-Clarke AT, Cadet E, Bomford A, Capron D, Viprakasit V, Miller A, et al. Digenic inheritance of mutations in HAMP and HFE results in different types of haemochromatosis. Hum Mol Genet 2003;12:2241-7. [ Links ]
10. Pietrangelo A, Caleffi A, Henrion J, Ferrara F, Corradini E, Kulaksiz H, et al. Juvenile hemochromatosis associated with pathogenic mutations of adult hemochromatosis genes. Gastroenterology 2005;128: 470-9. [ Links ]
11. Camaschella C, Roetto A, Cali A, De Gobbi M, Garozzo G, Carella M, et al. The gene TFR2 is mutated in a new type of haemochromatosis mapping to 7q22. Nat Genet 2000;25:14-5. [ Links ]
12. Aguilar-Martinez P. Non-HFE-related hereditary iron overload. Presse Med 2007;36:1279-91. [ Links ]
13. Brissot P, Troadec MB, Bardou-Jacquet E, Le Lan C, Jouanolle AM, Deugnier Y, et al. Current approach to hemochromatosis. Blood Rev 2008;22:195-210. [ Links ]
14. Biasiotto G, Camaschella C, Forni GL, Polotti A, Zecchina G, Arosio P. New TFR2 mutations in young Italian patients with hemochromatosis. Haematologica 2008;93:309-10. [ Links ]
15. Gerolami V, Le Gac G, Mercier L, Nezri M, Berge-Lefranc JL, Ferec C. Early-onset haemochromatosis caused by a novel combination of TFR2 mutations (p.R396X/c.1538-2 A>G) in a woman of Italian descent. Haematologica 2008;93:e45-6. [ Links ]
16. Pelucchi S, Mariani R, Trombini P, Coletti S, Pozzi M, Paolini V, et al. Expression of hepcidin and other iron-related genes in type 3 hemochromatosis due to a novel mutation in transferrin receptor-2. Haematologica 2009;94:276-9. [ Links ]
17. De Domenico I, Ward DM, Kaplan J. Hepcidin regulation: ironing out the details. J Clin Invest 2007;117:1755-8. [ Links ]
18. Hentze MW, Muckenthaler MU, Galy B, Camaschella C. Two to tango: regulation of Mammalian iron metabolism. Cell 2010;142:24-38. [ Links ]
19. Mendes AI, Ferro A, Martins R, Picanço I, Gomes S, Cerqueira R, et al. Non-classical hereditary hemochromatosis in Portugal: novel mutations identified in iron metabolism-related genes. Ann Hematol 2009;88:229-34. [ Links ]
![]() Correspondence:
Correspondence:
María Josefa Morán-Jiménez.
Centro de Investigación.
Hospital Universitario 12 de Octubre.
Avenida de Córdoba, s/n.
28041 Madrid, Spain.
e-mail: moranjimenez@h12o.es
Received: 21-12-10.
Accepted: 13-01-11.

