










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.10 Madrid oct./nov. 2012
https://dx.doi.org/10.4321/S1130-01082012001000003
Predictions and estimations of colorectal cancer mortality, prevalence and incidence in Aragon, Spain, for the period 1998-2022
Estimaciones y proyecciones de incidencia, prevalencia y mortalidad del cáncer colorrectal en Aragón, España, para el periodo de 1998 a 2022
Dyego Leandro Bezerra-de-Souza1, María Milagros Bernal2, Francisco José Gómez3 and Germán Jorge Gómez4
1Departamento de Saúde Coletiva. Universidade Federal do Rio Grande do Norte. Brasil.
2Department of Microbiology, Preventive Medicine and Public Health. Universidad de Zaragoza. Zaragoza, Spain.
3Familiar Medicine. Zaragoza, Spain.
4Hospital San Juan de Dios. Zaragoza, Spain
ABSTRACT
Objective: estimate colorectal cancer incidence and prevalence in Aragón, Spain, based on mortality and survival data from the period 1998-2007, and provide projections of incidence, prevalence and mortality until the year 2022.
Methods: general and colorectal cancer mortality rates were obtained from the National Statistics Institute and survival data was obtained from the EUROCARE study. Estimations were carried out through the program MIAMOD. The joinpoint program was used to quantify the annual change expected in the projections.
Results: in men, an increase in prevalence is expected, from 237.2 (Crude Rate - CR = 303.5) to 237.7 (CR = 412.7) per 100.000 inhabitants/year in 2022. Incidence rates would increase from 48.2 (CR = 61.6) in 2007 to 55.2 (CR = 83.1), and mortality would increase from 22.7 (CR = 29.4) to 26.0 (CR = 39.6) when comparing 2007 and 2022. In women, a reduction in prevalence is expected from 181.5 (CR = 268.3) to 167.9 (CR = 286.2) cases per 100,000 inhabitants/year. Incidence would change from 25.0 (CR = 38.0) in 2007 to 22.7 (CR = 39.2), and for mortality there is also an expected decrease, from 11.3 (CR =18.0) to 10.3 (CR = 18.5).
Conclusion: the projections indicate that colorectal cancer in Spain follows an increasing trend in incidence, mortality and prevalence in men, in opposition to corresponding decreasing trends in women. These projections must be considered in order to plan more effective prevention and treatment measures.
Key words: Colorectal cancer. Projections. Incidence. Mortality. Prevalence.
RESUMEN
Objetivo: estimar la incidencia y la prevalencia del cáncer colorrectal en Aragón, España, basándose en datos de mortalidad y supervivencia del periodo de 1998 a 2007, y proporcionar proyecciones de incidencia, prevalencia y mortalidad hasta el año 2022.
Métodos: la mortalidad por todas las causas y para el cáncer colorrectal se obtuvo del Instituto Nacional de Estadística y los datos de supervivencia del estudio EUROCARE. Las estimaciones han sido realizadas utilizándose el programa MIAMOD. El programa Joinpoint ha sido utilizado para cuantificar el cambio anual que se espera en las proyecciones.
Resultados: en los hombres, se prevé un aumento de la prevalencia con valor de tasa ajustada de 237,2 (tasa cruda - TC = 303,5) a 273,7 (TC = 412.7) casos por 100.000 habitantes/año en el año 2022. La tasa de incidencia aumentaría de 48,2 (TC = 61,6) a 55,2 (TC = 83,1) casos y la mortalidad de 22,7 (TC = 29,4) a 26,0 (TC = 39,6) al comparar los años de 2007 y 2022. En mujeres se espera una reducción de la prevalencia de 181,5 (TC = 268,3) a 167,9 (TC = 286,2) casos por 100.000 habitantes/año. La tasa de incidencia disminuiría de 25,0 (TC = 38,0) a 22,7 (TC = 39,2) y la mortalidad de 11,3 (TC = 18,0) a 10,3 (TC = 18,5).
Conclusión: las proyecciones indican que el cáncer colorrectal en España sigue una tendencia de aumento en la incidencia, mortalidad y prevalencia en hombres y reducción en mujeres. Se necesitan planificar medidas de prevención y tratamiento más efectivas.
Palabras clave: Cáncer colorrectal. Proyecciones. Incidencia. Mortalidad. Prevalencia.
Introduction
Colorectal cancer is the third most common cancer in men and the second most common in women. In 2008, approximately 1.2 million new cases were diagnosed and 609,000 deaths were recorded worldwide. In Spain, colorectal cancer is currently the third most common type of cancer in men, with age adjusted rates in accordance with the standard world population of approximately 39.7 and 18 cases per 100.000 inhabitants/year for incidence and mortality, respectively. In women, this type of cancer occupies the second position, with incidence and mortality rates of, respectively, 23 and 9.5 cases per 100.000 inhabitants/year (1). Incidence in Spain is comparable to that found in high risk zones of Occidental Europe, North America, Australia and Japan (2).
In 2008, it was estimated that approximately 28,551 new cases and 14,303 deaths by colorectal cancer were recorded in Spain and the prediction for 2015 is actually an increase in these values: 32,197 new cases and 16,104 deaths (1).
The information gathered on mortality and cancer incidence are the main resource, not only for clinical and epidemiological research on the determining factors for cancer, but also to quantify the magnitude of the disease and planify/evaluate health services. Knowledge on incidence, mortality and prevalence trends can be utilized to predict the number of incident cases and deaths in the future, and predict the necessities of treatment facilities (3).
Mortality indicators for cancer in Spain are produced at a national level, while other data, such as incidence and survival, are collected and analyzed by Population-Based Cancer Registries (PBCR), which cover only part of the country (4, 5). Data from the PBCR of Zaragoza, published in Cancer Incidence in Five Continents latest edition, for the 1996-2000 period, reveal that 1,230 cases were registered in men, with an adjusted rate of 29.4 (CR = 59.7) cases per 100,000 inhabitants/year. For women, 955 new cases were registered, with an adjusted rate of 18.5 (CR = 44.2) cases per 100.000 inhabitants/year (6). Nevertheless, incidence data take a while to be published because of data processing. In these situations, when it is not possible to obtain current and updated information on incidence and survival at a national or regional level, cancer estimations and predictions are important tools to quantify the assistance needs and, consequently, plan prevention and control measures (7).
The objective of this article was to estimate the incidence and prevalence of colorectal cancer in the Autonomous Community of Aragon, Spain, based on mortality and survival data from the period 1998-2207, and provide predictions of incidence, prevalence and mortality until the year 2022.
Methods
Colorectal cancer mortality data was considered (International Classification of Diseases, 10th revision - ICD-10: C18-C21), as well as populational data of such as sex, age and year for the period 1998-2007. Data were obtained from the Spanish National Statistics Institute (NSI) (8). The NSI determines estimations and predictions for the Spanish population, and these data were utilized for the period 2008-2022. Relative survival data were collected from the EUROCARE study, which includes data from six Spanish PBCR (9).
Estimations and predictions for incidence, prevalence and survival were calculated by the statistics program Mortality-Incidence Analysis Model (MIAMOD), applying "backwards" calculations from mortality and survival data. This method is based on mathematical relationships between mortality and prevalence, as well as the probabilities of incidence and survival, and can be utilized for other chronic illnesses. Incidence is calculated by a Poisson regression, which provides estimations with maximum likeliness to mortality. The model calculates the crude and adjusted rates (per 100,000 inhabitants/year), utilizing the European population as a reference. Incidence is predicted after the last year of observed data, based on changes in age-period-cohort of the observed period. The program uses a Weibull parametric model and relative survival data. Selection of the best model was made in function of likelihood. The model was validated by cross-checking the retrospective estimations obtained with the ones observed by mortality. The backwards calculation model of the MIAMOD program recalculates the mortality data required to start the program, in such a way that a correlation can be made between observed and estimated data to evaluate validity and reliability of estimations.
Data estimated by MIAMOD have been used to carry out a trend study using the regression program Joinpoint. The objective was to determine if the estimated trends were statistically significant, using adjusted rates (AR). Joinpoint analysis starts with a minimum number of joinpoints and tests whether more joinpoints are statistically significant and must be added to the model. This enables the user to test that an apparent change in trend is statistically significant (10).
Results
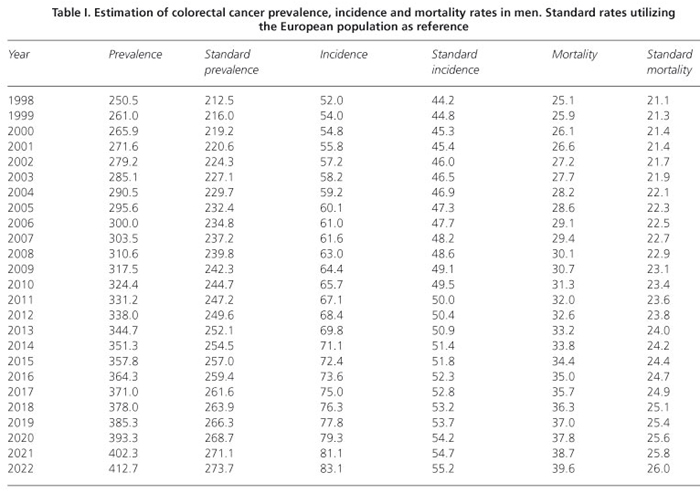
Predictions until the year 2022, based on the period 1998-2007, reveal different results according to gender for the incidence, prevalence and mortality rates of colorectal cancer. In men, there is an expected increase in prevalence, with an adjusted rate of 237.2 (crude rate, CR = 303.5) to 273.7 (CR = 412.7) cases per 100.000 inhabitants/year in the year 2022. Incidence rates would increase from 48.2 (CR = 61.6) to 55.2 (CR = 83.1) cases and mortality increases from 22.7 (CR = 29.4) to 26.0 (CR = 39.6) when comparing the years 2007 and 2022 (Table I).
In women, a reduction is expected in prevalence rates, from 181.5 (CR = 268.3) to 167.9 (286.2) cases per 100.000 inhabitants/year. Incidence rates would decrease from 25.0 (CR = 38.0) to 22.7 (CR = 39.2), and mortality from 11.3 (CR = 18.0) to 10.3 (CR = 18.5) cases per 100.000 inhabitants/year between the years 2007 and 2022 (Table II).

Joinpoint analysis demonstrated that the expected changes are statistically significant both in men and women (Figs. 1 and 2). In men, APC for prevalence and incidence were respectively 1.04 (CI: 95%; 1.0/1.1) and 0.92 (CI: 95%; 0.9/0.9). For mortality an increase was also observed with an APC of 0.90 (CI: 95%; 0.9/0.9). In women, a decrease was observed in prevalence, incidence and mortality: respective APCs are -0.42 (CI: 95%; -0.5/-0.4), -0.64 (CI: 95%; -0.6/-0.6) and -0.70 (CI: 95%; -0.7/-0.7).


Discussion
Different incidence trends for colorectal cancer incidence can be observed worldwide. Data from the publication Cancer Incidence in Five Continents reveal that there is an increasing trend for men in European countries, except in France where at first there was an increase but then a decrease in rates, with the same occurring in USA and Japan. In Canada and India the rates are stable. There are also increasing trends for women in most of Europe. In Canada, Denmark and Japan there was an increase and then a decrease in rates for women, and in India the rates are stable. Incidence follows increasing trends in South America and Asia in both men and women (2). Although there are technological advances in the treatment of colorectal cancer, mortality continues to increase in developing countries which also present defective health services, such as Brasil, Mexico and Romania (11).
Data of this investigation, carried out in the region of Aragon, has revealed an increasing trend in mortality by colorectal cancer in men, which is repeated in the predicted rates of incidence and prevalence. For women, a decrease was observed in prevalence, incidence and mortality rates. A study on trends and predictions of mortality for colorectal cancer with country-wide Spain data corroborates the findings presented herein. For the period 1995-2004, a 1.8% increase was identified for men and a reduction for women starting from 1995, after an increase recorded in the period 1985-1994. The prediction results, carried out until 2019, demonstrated a slight increase in mortality for men and reduction with a tendency to stabilization for women (12).
There are three main causes that might be related to decrease in colorectal mortality rates in a defined population: Changes in risk factors, screening programs, and improvements in treatment. In a study carried out in the USA, in the period 1975-2000, a reduction of 26% was observed in mortality by colorectal cancer. The predictive models have suggested that 53% of the increase was due to screening, 35% due to changes in risk factors, and the remaining 12% due to advances in treatment (13).
Screening programs are more common, mainly in developed countries, and are responsible for the changes in incidence and mortality trends identified recently. In the short-term, after the implementation of screening programs, there is an increase in incidence due to detection of prevalent cases. In the long-term, the inverse occurs: incidence reduces due to the diagnosis of precancerous polyps and consequent removal (11).
At an international level, selection of a determined screening modality for colorectal cancer varies in accordance with cost and availability of diagnostic resources. Colonoscopy is still a gold standard, although this modality requires a qualified examiner, implies in elevated costs, and is the most inconvenient test in the patient's viewpoint. For these reasons, colonoscopy as a screening method at a population level is the least indicated test in countries with limited resources. In these cases, the Fecal Occult Blood Test (FOBT) appears as a feasible alternative due to its low cost and simplicity of execution, although less sensitive than structural tests in the detection of precancerous polyps. The majority of countries that have screening programs in place utilize FOBT as a diagnostic method, such as the Czech Republic, Japan, Israel, France, Denmark. Other countries, such as Poland, Germany and USA have screening tests that use colonoscopy.
In Spain, screening programs started to be rolled out in the year 2000 and are limited to the region of Catalonia, where FOBT is utilized in the majority of population and colonoscopy in a smaller scale (11,14,15). Due to the elevated incidence rates, the Cancer Strategy in the National Health System has the objective, since 2009, of implementing populational screening programs for colorectal cancer based on FOBT (16). Nevertheless, the rather recent character of this program, which started in 2009, does not allow for the evaluation of the achieved results in our study, as the analysis is based on data of the year 2007. Therefore, for the population of Aragon there is no relationship between the trends encountered and the implementation of screening programs. Differences in trends according to gender in the population of Aragon, in consequence, could be related to changes in risk factors.
Diet, obesity, reduced physical activity and the consumption of alcohol and tobacco (17-21) can be mentioned as risk factors associated with colorectal cancer. Ex-smokers, even if they quit more than 10 years ago, presented a higher risk when compared to non-smokers and the amount of tobacco smoked was more important than the number of years smoking (21).
The new control law on the consumption of tobacco in Spain started on January 1, 2011. Prohibition of the consumption of tobacco in bars and restaurants was the most polemic measure. The main effected intended by this law is to reduce prevalence of tobacco consumption and, consequently, decrease the incidence of the illnesses associated with tobacco consumption, such as colorectal cancer. This law has been effective in the reduction of tobacco consumption prevalence in both genders in several countries (22). The predictions presented in this study are based on past trends and were carried out in the short term, which makes it difficult to reflect the results of this new law.
Regarding the consumption of alcohol in the Spanish population, data reveal that there was an increase until the late 1970s and then a reduction until the late 1990s (23,24).
Actually, according to the Ministry of Health and Consumer Affairs, the consumption of alcohol is high among Spanish society and remains stable. Approximately 64.6% of Spanish population consumes alcohol habitually and 14.9% daily (25). Legislation on the consumption of alcohol in Spain is still not yet in accordance with the measures recommended by scientific societies, regarding restrictions on hours and sales licenses, undisclosed publicity and other. The only advance was the age restriction (23).
The increase in colorectal cancer incidence rates in Asia and Oriental Europe reflect changes in diet and lifestyle due to "occidentalization", such as the consumption of tobacco and obesity. In the Czech Republic, for example, approximately 60% of men are smokers and obesity prevalence in adults is over 35% (26,27).
Obesity prevalence in Spain is high and together with Italy, Poland and Czech Republic, lead the European statistics and continue with increasing trends. The scientific literature discusses that changes in the Mediterranean diet caused by urbanization and globalization of certain lifestyles are the main responsible for obesity in Spain (27). According to data from the National Health Survey, for the period 1993-2005, an increase has been identified in morbid obesity prevalence, from 1.8 to 6.1 cases per 1000 inhabitants/ year. Prevalence has been higher in women, after age adjustments, and an annual increase of 12% in men and 4% in women was observed (28).
Primary prevention of colorectal cancer must be a priority in public health strategies. Primary prevention measures, especially legislative and educational measures, are more effective for the control of an illness, and are cheaper than assistance measures (29). The association between colorectal cancer incidence and factors associated with lifestyle, such as diet, obesity, reduced physical activity, consumption of tobacco and alcohol has been well documented and must be considered to decide the strategy to follow for an effective prevention.
Colorectal cancer predictions for prevalence, incidence and mortality reveal important data for the organization of health services. Although the trends observed were decreasing for incidence and mortality in women, the increment and high rates for men must be treated in a preferential manner in the combat plan against cancer in Aragon. It must be highlighted that the predictions presented herein are based on past trends, on past risk factor exposition, and may not continue in the future (30).
The detection of precancerous lesions or early-state cancer, via screening programs, along with advances in surgical techniques and adoption of treatment protocols must be utilized to reduce mortality and incidence of colorectal cancer. In the future, genetic tests will be utilized with higher frequency to identify high risk patients and, consequently, develop more effective prevention strategies, such as the prioritization of these patients on screening programs (31).
References
1. GLOBOCAN 2008, cancer incidence and mortality worldwide: IARC CancerBase no. 10 (internet). (Internet). Lyon, France: International Agency for Research on Cancer. Available at: http://globocan.iarc.fr [ Links ]
2. Ferlay J, Parkin DM, Curado MP, Bray F, Edwards B, Shin HR, et al. Cancer incidence in five continents, volumes I to IX: IARC CancerBase no. 9 (internet). Lyon, France: International Agency for Research on Cancer; 2010. [ Links ]
3. Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG. Cancer registration: Principles and methods. IARC Scientific Publications No. 95 ed. Lyon, France: IARC Scientific Publications No. 95; 1991. [ Links ]
4. Navarro C, Martos C, Ardanaz E, Galceran J, Izarzugaza I, Peris-Bonet R, et al. Population-based cancer registries in spain and their role in cancer control. Ann Oncol. 2010;21(Supl. 3):iii3-13. [ Links ]
5. de Souza DL, Perez MM, Curado MP. Gender differences in the incidence of laryngeal and hypopharyngeal cancers in Spain. Cancer Epidemiol 2011;35:328-33. [ Links ]
6. Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al., editors. Cancer incidence in five continents. Lyon, France: IARC Scientific Publications; 2008. [ Links ]
7. Bray F, Moller B. Predicting the future burden of cancer. Nat Rev Cancer 2006;6:63-74. [ Links ]
8. Instituto nacional de estadística (INE) (Internet). Available at: http://www.ine.es/ [ Links ]
9. EUROCARE (Internet). Available at: http://www.eurocare.it/ [ Links ]
10. Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000; 19:335-51. [ Links ]
11. Center MM, Jemal A, Smith RA, Ward E. Worldwide variations in colorectal cancer. CA Cancer J Clin 2009;59:366-78. [ Links ]
12. Ribes J, Navarro M, Cleries R, Esteban L, Pareja L, Binefa G, et al. Colorectal cancer mortality in Spain: Trends and projections for 1985-2019. Eur J Gastroenterol Hepatol 2009;21:92-100. [ Links ]
13. Edwards BK, Ward E, Kohler BA, Eheman C, Zauber AG, Anderson RN, et al. Annual report to the nation on the status of cancer, 1975-2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010;116:544-73. [ Links ]
14. Navarro M, Binefa G, Blanco I, Guardiola J, Rodriguez-Moranta F, Peris M, et al. Colorectal cancer screening: Strategies to select populations with moderate risk for disease. Rev Esp Enferm Dig 2009; 101:855-60. [ Links ]
15. Navarro M, Peris M, Binefa G, Nogueira JM, Miquel JM, Espinas JA, et al. Colonoscopic findings from a pilot screening study for colorectal cancer in Catalonia. Rev Esp Enferm Dig 2008;100:343-8. [ Links ]
16. Ministerio de Sanidad y Política Social. Estrategia en cáncer del sistema nacional de salud. Actualización aprobada por el consejo interterritorial del Sistema Nacional de Salud, el 29 de octubre de 2009, 2010. [ Links ]
17. Corpet DE. Red meat and colon cancer: Should we become vegetarians, or can we make meat safer? Meat Sci 2011;89:310-6. [ Links ]
18. Magalhaes B, Peleteiro B, Lunet N. Dietary patterns and colorectal cancer: Systematic review and meta-analysis. Eur J Cancer Prev 2012; 21:15-23. [ Links ]
19. Schlienger JL, Luca F, Vinzio S, Pradignac A. Obesity and cancer. Rev Med Interne 2009;30:776-82. [ Links ]
20. Boffetta P, Hashibe M. Alcohol and cancer. Lancet Oncol 2006;7:149-56. [ Links ]
21. Slattery ML, Potter JD, Friedman GD, Ma KN, Edwards S. Tobacco use and colon cancer. Int J Cancer 1997;70:259-64. [ Links ]
22. Shafey O, Eriksen M, Ross H, Mackay J. El atlas del tabaco. Atlanta, USA: American Cancer Society; 2009. [ Links ]
23. Bejar L, Gili M, Lopez J, Ramirez G, Cabanillas J, Cruz C. Trends in colorectal cancer in Spain from 1951-2007 and alcohol and cigarette consumption. Gastroenterol Hepatol 2010;33:71-9. [ Links ]
24. Núñez Pérez A, Soto Carballada C, Castro Pastor A. Consumo de drogas en España: Reflexiones sobre sus tendencias epidemiológicas y sociales. Psiquiatria Pública 1998;10:355-60. [ Links ]
25. Encuesta nacional de salud - España 2006 (Internet). Available from: http://www.msc.es/estadEstudios/estadisticas/encuestaNacional/home.htm [ Links ]
26. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev 2010;19:1893-907. [ Links ]
27. Berghofer A, Pischon T, Reinhold T, Apovian CM, Sharma AM, Willich SN. Obesity prevalence from a European perspective: A systematic review. BMC Public Health 2008;8:200. [ Links ]
28. Basterra-Gortari FJ, Beunza JJ, Bes-Rastrollo M, Toledo E, Garcia-Lopez M, Martinez-Gonzalez MA. Increasing trend in the prevalence of morbid obesity in Spain: From 1.8 to 6.1 per thousand in 14 years. Rev Esp Cardiol 2011;64:424-6. [ Links ]
29. Day TA, Chi A, Neville B, Hebert JR. Prevention of head and neck cancer. Curr Oncol Rep 2005;7:145-53. [ Links ]
30. de Souza DL, Bernal Perez MM, Curado MP. Predicted incidence of oral cavity, oropharyngeal, laryngeal, and hypopharyngeal cancer in Spain and implications for cancer control. Cancer Epidemiol 2011; 35:510-4. [ Links ]
31. O'Lorcain P, Deady S, Comber H. Mortality predictions for colon and anorectal cancer for Ireland, 2003-17. Colorectal Dis 2006;8:393-401. [ Links ]
![]() Correspondence:
Correspondence:
Dyego Leandro Bezerra de Souza.
Department de Microbiología,
Medicina Preventiva y Salud Pública.
Universidad de Zaragoza.
C/ Domingo Miral, s/n.
50009 Zaragoza
e-mail: dysouz@yahoo.com.br
Received: 31-01-2012
Accepted: 11-09-2012

