










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.1 Madrid ene. 2013
https://dx.doi.org/10.4321/S1130-01082013000100016
LETTERS TO THE EDITOR
Ischemic colitis associated with hormonal contraceptive treatment delivered via vaginal ring
Colitis isquémica asociada con el tratamiento hormonal anticonceptivo administrado mediante un anillo intravaginal
Key words: Ischemic colitis. Contraceptive vaginal ring.
Palabras clave: Colitis isquémica. Anillo vaginal anticonceptivo.
Dear Editor,
We present the case of a young woman diagnosed with ischemic colitis associated with contraceptive hormonal therapy delivered via a vaginal ring. We have not found a similar case in the published literature.
Case report
A 28-year-old woman without any significant personal medical history who was treated with anticonceptive hormonal therapy (etonogestrel and ethinylestradiol) delivered by vaginal ring due to menstrual anomalies in the two previous years.
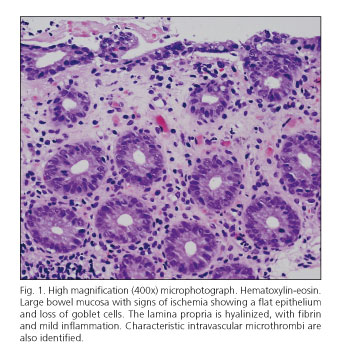
During that time, she developed chronic constipation and underwent a colonoscopy. A friable, edematous mucosa with superficial ulcerations covered with fibrin, was found in the descending colon. The histopathological study of the biopsies showed atrophy and regenerative changes in the epithelium with presence of capillary microthombi (Fig. 1). The neutrophilic infiltrate was minimal but submucosal edema was important. The changes were compatible with ischemia even though its origin was still undetermined.
After colonoscopy the vaginal ring was removed and a repeat colonoscopy was performed after 4 months in which the lesion had resolved. Constipation then responded to conventional treatment. In order to exclude other possible causes of ischemic colitis an analytical and immunological assessment, electrocardiogram, echocardiogram and a computed tomography angiography were also performed and found to be normal. Coagulation tests showed antigenic S protein deficiency. Factor V Leyden and G20210A mutation in the thrombin gene were absent. The genetic study showed the same anomaly in the patient's father.
Discussion
Ischemic colitis is more frequent in women with advanced age with concomitant cardiovascular diseases (1). In young women, due to its low prevalence, this disease is not well characterized (2). In them, the most common cause is the use of oral hormonal therapy due to their prothrombotic effect (2-4). Other causes of ischemic colitis in young women are pulmonary embolism, vasoactive drugs, hypovolemia, vasculitis and some antibiotics (2). Some studies have suggested that a genetic predisposition to thrombosis may play an important role in the pathogenesis of ischemic colitis in young women (5). It has also been described during pregnancy, probably related to the high circulating levels of estrogens (6). In almost half of the cases, the cause is not found (2).
The most common symptoms that should alert to the possible development of ischemic colitis are abdominal pain, hematochezia and bloody diarrhea (2,7). In general, the patients are diagnosed by colonoscopy, which shows a segmental involvement of the left colon (2,8). This location of the lesions is due to the lack of collaterals in that area of the colon. Other segments of the colon can also be affected (3). Clinical diagnosis is difficult and a biopsy is normally required (9). This can be done safely usually unless the mucosa has a black or dusky color in which case the risk of perforation is high. The endoscopic and histological findings of ischemic colitis are similar to those described in our case and, even though they are nonspecific, they have a vital role in early diagnosis (7). As in our case, the superficial layers of the mucosa were more severally affected than the deeper portions partly due to a mechanism that reduces oxygen delivery in the upper part of the mucosa in case of hypoperfusion. As in our case, most cases resolve spontaneously or with a conservative treatment (1). Patients with long ischemic time however can develop important complications and recovery occurs with severe fibrosis and strictures.
In conclusion, this is the first case of ischemic colitis due to hormonal contraceptive treatment delivered via vaginal ring favored by a mild preexisting congenital hypercoagulability state.
Pablo Solís-Muñoz1, M. Teresa Muñoz-Yagüe2, Yolanda Rodríguez-Gil3, Francisco Colina3 y José Antonio Solís-Herruzo4
1Institute of Liver Studies. Kings College Hospital. London, United Kingdom.
2Gastroenterology Department. Hospital Universitario 12 de Octubre. Universidad Complutense. Madrid, Spain.
3Pathology Department. Hospital Universitario 12 de Octubre. Universidad Complutense. Madrid, Spain.
4Research Institute. Hospital 12 de Octubre. Universidad Complutense. Departamento de Medicina. School of Medicine. Madrid, Spain
References
1. Theodoropoulou A, Koutroubakis IE. Ischemic colitis: clinical practice in diagnosis and treatment. World J Gastroenterol 2008;14:7302-8. [ Links ]
2. Preventza OA, Lazarides K, Sawyer MD. Ischemic colitis in young adults: a single-institution experience. J Gastrointest Surg 2001;5:388-92. [ Links ]
3. Deana DG, Dean PJ. Reversible ischemic colitis in young women. Association with oral contraceptive use. Am J Surg Pathol 1995;19:454-62. [ Links ]
4. Chevrel B. Acute damage to the digestive tract related to contraceptives. Contracept Fertil Sex (Paris) 1981;9:317-22. [ Links ]
5. Theodoropoulou A, Sfiridaki A, Oustamanolakis P, Vardas E, Livadiotaki A, Bounpaki A, et al. Genetic risk factors in young patients with ischemic colitis. Clin Gastroenterol Hepatol 2008;6:907-11. [ Links ]
6. Frossard JL, Spahr L, Queneau PE, Armenian B, Bründler MA, Hadenque A. Ischemic colitis during pregnancy and contraceptive medication. Digestion 2001;64:125-7. [ Links ]
7. Zou X, Cao J, Yao Y, Liu W, Chen L. Endoscopic findings and clinicopathologic characteristics of ischemic colitis: a report of 85 cases. Dig Dis Sci 2009;54:2009-15. [ Links ]
8. Lozano-Maya M, Ponferrada-Díaz A, González-Asanza C, Nogales-Rincón O, Senent-Sánchez C, Pérez-de-Ayala V, et al. Usefulness of colonoscopy in ischemic colitis. Rev Esp Enferm Dig 2010;102:478-83. [ Links ]
9. Villanacci V, Manenti S, Antonelli E, Chiudinelli M, Giuliano V, Vassotti G. Non-IBD colitides: clinically useful histopathological clues. Rev Esp Enferm Dig 2011;103:366-72. [ Links ]

