










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.9 Madrid oct. 2013
https://dx.doi.org/10.4321/S1130-01082013000900004
Safety and effectiveness of gastric balloons associated with hypocaloric diet for the treatment of obesity
Seguridad y efectividad de los balones gástricos asociados a una dieta hipocalórica en el tratamiento de la obesidad
M.a Luisa de-Castro1, M.a José Morales2, Miguel A. Martínez-Olmos3, Juan R. Pineda1, Lucía Cid1, Pamela Estévez1, Víctor del-Campo4 and J. Ignacio Rodríguez-Prada1
Departments of 1Gastroenterology, 2Endocrinology, and 4Epidemiology. Complexo Hospitalario Universitario de Vigo (CHUVI). Vigo, Pontevedra. Spain.
3Department of Endocrinology. Complexo Hospitalario Universitario de Santiago de Compostela (CHUS). A Coruña, Spain
ABSTRACT
Introduction: intragastric balloons provide early satiety and thereby induce short-term weight loss. The aim of this study was to evaluate safety and short and medium-term effectiveness of gastric balloons associated to hypocaloric diet in obesity.
Material and methods: from May 2004 to June 2011 91 obese patients, body mass index [BMI] 45.2 ± 7.2 kg/m2 were prospectively followed after endoscopic implantation of a gastric balloon associated to restricted diet. Successful therapy was defined as percent loss of total weight (%LTW) ≥ 5% at six months after balloon placement and 6 and 12 months after their withdrawal. All analyses followed intention-to treat principles considering significant p-values < 0.05.
Results: we placed 73 fluid-filled balloons (80.2%) and 18 air-filled ones (19.8%). Compared to baseline values, at 6-month 73.7% subjects succeeded, showing significant reductions in weight (13.3 ± 8.8 kg), BMI (5 ± 3.4 kg/m2) (p < 0.0001), with% LTW 11 ± 7%. Six and twelve months after retrieval 45.1% and 28.6% patients reached% LTW ≥ 5%. Short-term and medium-term effectiveness was negatively associated to obesity in first-grade relatives (p = 0.003 and p = 0.04). Higher weight loss 6 months after balloon placement independently predicted medium-term effectiveness (p = 0.0001). Mortality was absent but there were two spontaneous deflations of air-filled balloons and severe withdrawal difficulties in 8 patients, leading to surgery in one case. Retrieval complications associated to air-filled balloons (p = 0.0005).
Conclusions: in obesity, effectiveness of gastric balloons associated to hypocaloric diet decreases over time.
Complications occurred mainly in the retrieval endoscopic procedure and related to air-filled balloons.
Key words: Intragastric balloon. Bariatric treatment. Obesity. Morbid obesity. Endoscopy.
RESUMEN
Introducción: el balón gástrico produce saciedad precoz favoreciendo la pérdida de peso en un corto plazo de tiempo. El objetivo de este estudio fue evaluar la seguridad y la efectividad del tratamiento mediante balón gástrico y dieta hipocalórica en la obesidad.
Material y métodos: estudio de cohortes prospectivo en 91 pacientes obesos sometidos a balón gástrico durante 6 meses. Como criterio de efectividad se consideró el porcentaje de peso perdido (PPP) ≥ 5% 6 meses tras su colocación y 6 y 12 meses tras su retirada. Analizamos los resultados por intención de tratar, considerando significativos los valores de p < 0,05.
Resultados: empleamos 73 balones rellenos de líquido (80,2%) y 18 de aire (19,8%). Tras 6 meses un 73,7% de pacientes alcanzó el objetivo terapéutico mostrando descenso de peso (13,3 ± 8,8 kg) e IMC (5 ± 3,4 kg/m2) (p < 0,0001), con PPP 11 ± 7%. Transcurridos 6 y 12 meses de la retirada un 45,1% y 28,6% mantenían un PPP ≥ 5%. La efectividad a corto y medio plazo se asoció negativamente con obesidad en familiares (p = 0,003 y p = 0,04). La pérdida ponderal lograda tras 6 meses se asoció con efectividad a medio plazo (p = 0,0001). No existió mortalidad, observando 2 desinflados espontáneos y 8 retiradas complicadas, requiriendo cirugía 1 paciente. Los balones rellenos de aire presentaron más complicaciones (p = 0,0005).
Conclusiones: la efectividad del tratamiento combinando balón gástrico y dieta hipocalórica en la obesidad disminuye a lo largo del tiempo.
Las complicaciones ocurrieron mayoritariamente durante la retirada endoscópica y con el empleo de balones rellenos de aire.
Palabras clave: Obesidad. Obesidad mórbida. Balón intragástrico. Endoscopia.
Introduction
Obesity is a chronic disease with considerable morbidity and mortality and its prevalence is rising rapidly in both developed and developing countries all over the world (1,2). Numerous diseases are caused or worsened by obesity, shortening life expectancy and decreasing quality of life as well(3,4).
A caloric-restricted diet associated to physical activity and behavioral modifications are considered as the mainstay of therapy in obesity (1,5). The aim of treatment is to achieve and maintain a significant weight loss, as 5-10% reduction of initial body weight is enough to produce health benefits in obesity related morbidities (1,6). Nevertheless for obese patients who fail to achieve an adequate weight loss pharmacotherapy is very limited, as many drugs had to be withdrawn as causing severe adverse effects (7). On the other hand bariatric surgery is generally restricted to the most severe degrees of obesity, as it posses mortality and morbidity (8).
In summary, there is a wide intermediate group of patients who do not respond to medical therapy and who are not candidates to bariatric surgery or even refuse it.
Intragastric balloons are endoscopical devices filled with liquid or air that are placed into the stomach for a limited period of time. As these devices produce a feeling of early satiety, they are considered to be a temporary and reversible restrictive therapeutic method of facilitating the implementation of adequate dietary and behavioral habits (9,10).
Although gastric balloons had been used for over thirty years in obese patients, they have not yet proved to be a convincing means of primary weight loss. This is due to that several articles have comprehensively analyzed different types of balloon some of them obsolete (11) and lack of standardized data on its effectiveness especially in the medium and long term.
Our aim was to assess the safety and effectiveness of this endoscopical devices associated to hypocaloric diet in the treatment of obesity.
Material and methods
Prospective single centre cohort study performed in 91 obese subjects referred for placement of gastric balloon. Inclusion criteria were morbid obesity (body mass index BMI > 40 kg/m2) in preparation for a bariatric operation to reduce surgical risk or if they were not candidates for this surgery, type II obesity (BMI 35-40 kg/m2) with obesity-related diseases that ruled out bariatric surgery or who had failed many attempts at weight loss and both obesity type patients in preparation for an elective surgery.
Exclusion criteria were hormonal or genetic obesity, presence of an organic disease of the upper gastrointestinal tract, large hiatal hernias > 3 cm, previous gastric surgery and patients on anti-inflammatory or anticoagulant therapies.
Bioenterics intragastric balloons (BIB® Allergan USA) filled with liquid were placed in 73 patients and Heliosphere Bag® air filled balloons in 18 subjects.
Enrolled patients underwent blood tests and a clinical evaluation including family diseases, eating habits, weight measures and dietary and nutritional education. Specifically written informed consent was signed by all participants and the study was approved by the local clinical research committee.
After performing a diagnostic upper endoscopy, the balloons were passed and located under the inferior esophageal sphincter using conscious sedation controlled by the endoscopist with midazolam and fentanyl. Then the injection catheter was connected to a 60 cc syringe and the BIB® balloons were slowly inflated with 500-700 ml of saline solution stained with 10 ml of methylene-blue dye, and the Heliosphere Bag® balloons with 900-960 cc of air. The proper filling and release of balloons was checked by endoscopy, recording insertion and retrieval complications. During the first 24 hours after placement, intravenous saline (30-35 ml/kg/day), pantoprazole (40 mg/day) and metoclopramide (30 mg/day) were administered. The initial diet was liquid with a gradual return to solid food and all participants were discharged home on a 1,000 kcal diet, oral multivitamin supplements and proton pump inhibitors (PPIs).
Follow-up included a 1, 3 and 6-month check-up with routine blood tests and weight controls. At these intervals, patients were asked for digestive complaints such as vomiting, epigastric pain and gastroesophageal reflux symptoms.
At 6 months, gastric balloons were removed on an outpatient basis under general anesthesia and tracheal intubation. We used the extraction kit provided by the manufacturer for each type of balloon, which consists of an empty catheter to puncture and deflate the devices and a hook forceps to grasp and remove them. After balloon removal patients were followed for up to 12 months by their endocrinologist recording body weight measures at 3, 6 and 12 months.
The results are analyzed with SPSS statistical program SPSS 15.0 (SPSS Inc, Chicago IL) and presented as mean and standard deviation for numerical variables and as absolute number (percentage) for categorical ones, being analyzed using the appropriate method for each comparison and considering as significant p values < 0.05. All analysis were carried out on an intention-to-treat basis considering as an accepted criterion of effectiveness of this treatment if percentage loss of total weight (% LTW) was > 5% at 6 months after placement (short-term effectiveness) and 6 and 12 months after withdrawal (medium-term effectiveness).
Results
From May 2004 to June 2011 ninety-one obese subjects underwent gastric balloon placement: 23 males/68 females (74.7%), mean age 43,3 ± 11,5 years, range (18-69), mean weight 121,3 ± 22,8 kg, range (78-198), mean BMI 45,2 ± 7,2 kg/m2 range (33,8-66,3).

Eighty-three balloons (91.2%) were placed in our Endoscopy Unit under conscious sedation controlled by the endoscopist using midazolam at mean dose 7.7 ± 1.6 mg range (1-13). In twenty patients fentanyl (range 50-150 mcg) was intravenously administered as well, and 78 (94%) received benzodiazepine antagonist as flumacenyl at the end of procedure. Endoscopic and post-positioning mortality were absent and obese patients had neither cardiac nor breathing complications during the endoscopical procedures.
Seventy-three patients (80.2%) showed no lesions in the upper gastrointestinal tract at initial endoscopy and 83 had indemnity at retrieval endoscopy (91.2%), finding a low percentage of esophagitis (1.1-3.3%), duodenitis (8.8-0%), gastric erosions (5.5-2.2%) or gastric polyps (3.3-1.1%) in both procedures.
Balloon positioning was mainly uneventful. Twenty three BIB® balloons (30.1%) were filled with 500 ml and 50 (68.5%) at their full capacity of 700 ml. During placement, there were two technical events: One defective valve in a BIB® balloon, which was replaced by a new one in the same act, and hard resistance to pharyngeal passage in eight cases, requiring a new appointment under general anesthesia to placement. However, there were no differences in placement complications between balloons filled with liquid or with air.
The balloons stayed into the stomach for 6.2 ± 1.9 months range (0-8). Eighty-one patients (89%) had withdrawal under general anesthesia and tracheal intubation, two Heliosphere Bag® balloons were spontaneously deflated and eliminated in stools and 8 balloons were removed at the Endoscopy Unit under conscious sedation with midazolam and fentanyl. Removal was uneventful in 75 patients (82.4%), but six subjects had a large amount of solid food in their stomachs that temporary precluded the withdrawal despite of mandatory 24 hours liquid diet prior to balloon extraction requiring a new appointment. In 8 cases the retrieval was considered as extremely difficult by the endoscopist as the deflated balloons did not go across the cardia or the upper esophageal sphincter requiring a prolonged procedure time, various endoscopic tools such as forceps and snares or even the use of rigid esophagoscope (4 cases) or laparoscopic surgery (1 case) to finally remove the balloon. Comparing the two devices, there was a higher complication rate related to air-filled balloon (p = 0.0005) especially in the retrieval endoscopic procedure (Fig. 1).

The in-hospital stay for balloon placement was 2.9 ± 1.4 days range (0-8) and digestive symptoms were generally present such as vomiting (50.5%), epigastric pain (37.4%), nausea (19.8%) and heartburn (8.8%).
Removal of the balloon prior to the scheduled data was performed in 12 cases (13.2%) in 78.6 ± 66.3 days range (7-168), because of psychological intolerance or continued vomiting. It was more frequent in females (p = 0.03) and in patients that complained about digestive symptoms beyond the first month (p = 0.001). We did not find any differences between both gastric balloons regarding tolerance.
Two patients suffered from gastrointestinal bleeding while the balloon was located in their stomach. The endoscopy showed a tear on the cardia in one case and acute gastric erosions in the other patient; both of them resolved without requiring early removal of the devices.
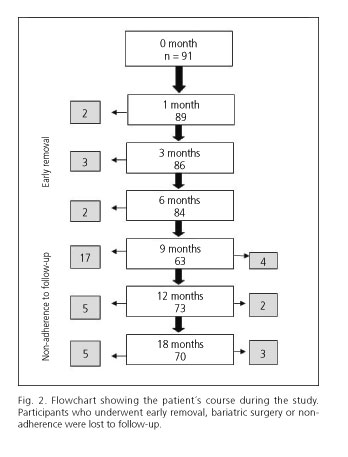
Hypocaloric diet plus balloon caused a considerable body weight reduction throughout the study. Six-month after balloon placement 84 patients were evaluated (92.3%) (Fig. 2), mean weight reduction was 13.3 ± 8.8 kg, BMI reduction was 5 ± 3.4 kg/m2,% LTW was 11 ± 7 and% EWL 27,3 ± 19,9. There were significant differences in BMI and weight values regarding basal values (p = 0.0001). Weight losses increased continuously throughout the 6-month period of balloon implantation, but the main decrease occurred at three months (88% LTW). Air-filled balloons showed similar weight reduction as fluid-filled ones.
In an intention to treat basis, at 6 month 73.7% patients showed weight loss ≥ 5% from initial weight and 50.5% patients reached weigh loss ≥ 10%. There were not differences in effectiveness regarding age, sex, degree of obesity, fluid-filled balloon volume, or smoking habit. Nevertheless, obesity in first degree relatives, binge eating disorder and sweet food eating were related to worse result with this therapy. In multivariate analyses obesity in first-degree relatives was the only factor significantly related to less effectiveness (p = 0.003). On the other hand, 26.4% patients enrolled in the study reduced less than 5% of their initial body weight despite of restricted diet plus gastric balloon for six months.
After balloon retrieval patients followed no structured weight maintenance program, attending visits to their endocrinologist at 3, 6 and 12 months, and 14.8% patients were lost because of being operated on or due to non-adherence to follow-up schedule (Fig. 2).
Patients showed a progressive regain of weight over time. Mean lost weight at 6 month were 6.3 ± 10,6 kg and reduction in BMI 2.4 ± 4.1 kg/m2, both lesser than their basal values (p = 0.0001) % LTW was 5.4 ± 9.2% and % EWL 13.7 ± 24.7%. At 12 month weight loss was 2.4 ± 4.1 kg and BMI decrease 1.1 ± 4.4 kg/m2 (p = 0.03),% LTW 2.2 ± 10% and% EWL 5.4 ± 25.7%.
In an intention to treat analysis% LTW ≥ 5% was reached by 45.1% and 28.6% at 6 and 12 months after balloon retrieval, and% LTW ≥ 10% for 24.2% and 17.6% at the same intervals.
Obesity in first-degree relatives was independently associated to worse medium-term effectiveness, whereas higher weight loss at 6 month was associated to a better medium-term effectiveness.
Discussion
The first experience in the treatment of obesity by placing gastric balloons was published in 1982, but these devices have undergone significant technological changes since then (12). The first prototypes were built with weak materials, had low volumes and were filled with air, being abandoned by a prohibitive number of complications and limited effectiveness (13,14). Nowadays, the most widely used gastric balloons are filled with air and fulfill international recommendations on safety (15), having low mortality (0.06%) and severe morbidity (< 1%) rates in two systematic reviews and one meta-analysis conducted in more than 5.0000 obese patients (16-18).
As regards to endoscopic procedures of placement and withdrawal of these devices, we found a great variability in the literature, performing both by general anesthesia, with conscious sedation controlled by the endoscopist or performing one procedure, usually the retrieval, under anesthesia. We choose the latter option as consider withdrawal to be a more complex procedure than placement, although the gain in safety that occurs by incorporating an anesthesiologist should be contrasted with the greatest economic cost that it represents. Regarding the implantation procedure, in this study there were neither adverse cardiovascular nor respiratory events justifying the administration of antiarrhythmic, inotrope or vasopressor drugs or performing resuscitation, although obese patients required high doses of benzodiazepines to obtain adequate sedation as these drugs are administered in body weight basis. The frequent administration of benzodiazepines antagonists was performed to reduce postsedation monitoring time and not to reverse a decreased level of consciousness at the end of the endoscopic procedure. Nevertheless, upper gastrointestinal (GI) endoscopy under sedation in obese patients is considered to be a procedure with an increased risk of cardiovascular and respiratory complications compared to normal-weight subjects (19), so we think that the combinations of sedative and analgesic drugs should be administrated as appropriate for the endoscopic procedure and the condition of the patient by qualified and trained practitioners (20).
Moreover an increased prevalence of upper GI pathology has been reported in obese subjects (21), but we did not find any lesion that could alter the balloon protocol. This fact questions the profitability of the routine upper GI endoscopy performed before the placement of these devices versus the recognized value of the endoscopy prior to bariatric surgery, which alter the planned operative procedure in 5-42% cases (22). In this series the GI tract showed no lesions in 80.2% at initial endoscopy and in 93.4% at withdrawal, but other authors have reported the onset or worsening of peptic esophageal lesions between 5% and 22% at the retrieval endoscopy (23,24). One explanation for this difference may lie as all the patients took full-dose PPI while the balloons stayed in their stomach. On the other hand the lowest percentage of gastric polyps at retrieval can be explained as the biopsies took at the prior endoscopy removed these lesions.
New gastric balloons have recently become available. Adjustable balloons with long-term durability permit long implantation time (25), and gastric devices filled with air could result in better gastrointestinal tolerance (26).
Twelve obese (13.2%) had the balloon removed before the scheduled data due to digestive intolerance. Early removal was significantly associated with female gender and persistence of gastrointestinal symptoms beyond the first month of follow-up. However this study showed no differences in post-procedure hospital stay, presence of GI symptoms at follow-up or early removal between liquid and air-filled balloons. Gastric balloons placement is often managed in an outpatient basis, however we decided to place them in a short hospital stay because of the high frequency of digestive complaints and oral intolerance in the first 24 hours.
There were no major complications or differences between both balloons in the placement endoscopic procedure, but complications occurred in 16 withdrawals (17.6%). Heliosphere® balloon associated to spontaneous deflation and serious difficulties at the endoscopic removal because the deflated device maintains a big volume, causing high resistance to removal across the cardia and the upper esophageal sphincter. This forced us to perform complementary radiological studies to exclude intestinal migration of the balloons and to employ various endoscopic tools as forceps and snares to achieve their removal, requiring laparoscopic gastric surgery in one patient, so we consider there are significant differences regarding safety between both gastric balloons.
The lower safety profile of air-filled Heliosphere® balloon have been previously reported by several authors as these devices have greater rigidity that hinders the placement under conscious sedation, the lack of an early warning system to detect spontaneous deflation as methylene blue leads to exposing patients to several disturbing diagnostic procedures and they present greater difficulties to endoscopic removal (27-29).
The complications in the balloon withdrawal have been associated with a prolonged gastric implantation time (30). The manufacturers recommend removal of both gastric balloons six month after implantation, as gastric acid can weaken the material hampering the grasping and retrieval of these devices. The mean duration of balloon implantation in our series was 6.2 (2) months and it was not associated with a difficult removal of the balloons.
The lack of effectiveness of the balloons used before the 90s as its usual employment adjunct to a restricted diet raised important questions about the real efficacy of these devices to promote weight reduction. In 2006 Genco definitely established the efficacy of gastric balloons versus restricted diet in obesity (31), but recently a systematic review had questioned it again (11), although this study represents a very limited evidence for decision making as it evaluated obsolete gastric balloons.
With regard to effectiveness of gastric balloons, at 6 months the mean weight loss achieved was 13.4 (8.8) kg, the decrease of BMI and waist circumference were 5 (3.4) kg/m2 and 8.1 (6.4) cm and the ratios% LTW and% excess weight loss (EWL) situated on 11 (7) and 27.3 (19.9) respectively, showing a gradual increase along the implantation time of these devices. Our short-term results were similar to those previously reported confirming the effectiveness of this therapy in a weight loss range of 13-18 kg (18,32-34). Sixty-seven subjects (73.7%) reached a weight loss ≥ 5% and 46 patients (50.5%) had weight loss ≥ 10% of weight at baseline. Weight reduction showed a linear trend during the implantation time of these devices, although the greater decrease occurred in the first three months after the placement (88% of total weight loss). This fact has been linked to the development of gastric adaptation mechanisms to the balloon volume, which lead to the disappearance of the negative feedback on the brain centers of appetite (35). However this study shows that weight loss continues but at a slow rate during all the implantation time (30,36), but whether weight loss might have been higher with more frequent scheduled reviews or changes in the balloon volume remains to be demonstrated.
On the contrary there is a group of obese in whom this treatment shows no effectiveness and different studies have reported it from 10 to 40% depending on how to define a satisfactory result (17,23). In this study failure occurred in 26.4% defined as failing to lose 5% of weight at baseline upon removal of the gastric balloons. This lack of response has been attributed to lack of patient adherence to dietary and exercise recommendations prescribed as those showing better response are those that had higher motivation (23), so it has thought to select candidates for gastric balloon evaluating various personal characteristics that make us foresee a higher response rate. Previous studies have associated a favorable response with young age (32) (32), morbid obesity (36) and continuous vomiting (23,37) while a bad response was related to habits such as binge eating (17,32). Our results showed that several eating habits and obesity in close relatives were associated with lesser effectiveness, though only obesity in first-degree relatives remained statistically significant after multivariate analysis (Table II).


On the other hand the medium and long-term effectiveness of this treatment has not been definitively established and the available data are scarce and heterogeneous ranging from failure if 16% patients maintained weight loss at 12 months from withdrawal (32) to success whether 40% did it (38,39). In the current study there was a progressive weight regain at follow-up, but six month after retrieval weight, BMI and waist losses remained statistically lower than measures at baseline, although at 12 months follow-up only BMI did. An intention to treat analysis showed a LTW ≥ 5% at 12 months and 18 months of the study (6 and 12 months after removal of the balloon) in 45.1% and 28.6% of patients respectively, achieving a LTW ≥ 10% at the same intervals 24.2% and 17.6%. Dastis et al. recently have reported success in a quarter of obese patients after gastric balloon at 2,5 years follow-up (34), although Herve y Kotzampassi found a 50% of obese patients with EWL > 20% at 12 months after balloon retrieval (37,40). In view of these results, the variability regarding the medium-term effectiveness of these devices can be explained by methodological differences in the evaluation of weight as well as to the implementation of interventions during the follow-up. Regarding the variables associated with weight maintenance after gastric balloon, obesity in close relatives was the only variable related to lesser effectiveness.
This item had been associated with less short-term effectiveness as well and an possible explanation could be the feeding behavior of the whole family as it has a higher degree of aggregation (41) being a target to the failure to modify dietary habits of the obese patient that they shares with their family members. However, the existence of genetic factors in this population that could explain this association can not be entirely discarded and the real significance of this variable must be study in prospective studies.
Another factor that has been linked to the effectiveness of this treatment in medium-term is the weight lost while the balloon is into the stomach (30,42). Our results show that patients who succeeded at 6 and 12 month after retrieval were those that had deeply reduced weight at the time of removal of these devices.
In summary, the results found in this study show that gastric balloons associated to restricted diet are an effective therapy in obesity in the maintaining of weight loss in the short term, but effectiveness decreases over time. However, this treatment has lack of effectiveness and intolerance, being important to identify patient characteristics to select best responders to this therapy. It is necessary as well to establish a scheduled follow-up after gastric balloon in order to improve and compare the results (43).
Despite a low mortality and morbidity of fluid-filled balloons, endoscopic procedures concentrate most of the complications considering that air-filled balloons have a worse safety profile but a similar effectiveness that fluid-filled balloons.
References
1. Rubio MA, Salas-Salvadó J, Barbany M, Moreno B, Aranceta J, Bellido D, et al. Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios terapéuticos. Rev Española de Obesidad 2007:7-48. [ Links ]
2. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. 2000; Technical Repor Series no 894. WHO; Obesity and overweight. Global Strategy on Diet, Physical Activity and Health. Available at: www.who.int/nutrition/publications/obesity/WHO_TRS_894/, Geneva: 2003. [ Links ]
3. Heber D. An integrated view of obesity. Am J Clin Nut 2010;91:280S-3S. [ Links ]
4. Adams KF, Schatzkin A, Harais TB, Kipnis V, Mouw T, Ballard-Barbash R,et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med 2006;355:763-78. [ Links ]
5. Martínez-Olmos MA, Casanueva-Freijo F. Avances en el tratamiento de la obesidad. Aplicaciones a la práctica clínica. Medicine 2009;10:3083-90. [ Links ]
6. Tsigos C, Hainer V, Basdevant A, Finer N, Fried M, Mathus-Vliegen E, et al. Management of obesity in Adults: European Clinical Practice Guidelines. Obesity Facts 2008;1:106-116. [ Links ]
7. James VP, Caterson ID, Coutinho W, Finer N, Van Gaal LF, Maggioni AP, et al.; SCOUT Investigators. Effect of sibutramine on cardiovascular outcomes in overweight and obese subjects. N Eng J Med 2010;363: 905-17. [ Links ]
8. Kral J. ABC of obesity management: Part III-Surgery. BMJ 2006;333:900-3. [ Links ]
9. Zago S, Kommuller AM, Agaglioti D, Saber B, Ferrari D, Maffeis P, et al. Benefit from bioenteric intragastric balloon (BIB) to modify lifestyle and eating habits in severely obese patients eligible for bariatric surgery. Minerva Med 2006;97:51-64. [ Links ]
10. Espinet E, Nebreda J, Gómez JA, Muñoz-Navas M, Pujol J, Vila C, et al. Técnicas endoscópicas actuales en el tratamiento de la obesidad. Rev Esp Enferm Dig 2012;104:72-87. [ Links ]
11. Fernandes M, Atallah AN, Soares BGO, Humberto S, Guimarães S, Matos D, et al. Balón intragástrico para la obesidad (Revisión Cochrane traducida). En: La Biblioteca Cochrane Plus, Número 2. Oxford: Update Software Ltd. Cochrane; 2008. [ Links ]
12. Nieben OG, Harboe H.Intragastric balloon as an artificial bezoar for treatment of obesity. Lancet 1982;23:198-9. [ Links ]
13. Lindor KD, Hughes RW, Ilstrup DM. Intragastric balloon in comparison with standard therapy for obesity- a randomized, double-blind trial. Mayo Clin Proc 1987;62:992-6. [ Links ]
14. Hogan RB, Johnston JH, Long BW. A double-blind, randomized, sham-controlled trial of the gastric bubble for obesity. Gastrointest Endosc 1989;35:381-5. [ Links ]
15. Shapiro M, Benjamin S, Blackburn G, Frank B, Heber D, Kozarek R. et al. Obesity and the gastric balloon: a comprehensive workshop. Gastrointest Endosc 1987;33:323-7. [ Links ]
16. Ivan M, Wang S, Newton S, Zimprich C, Sullivan T, Martin T, Hiller J. Intragastric balloons for the temporary management of morbid obesity. 2008 MSAC application 1112. [ Links ]
17. Dumonceau JM. Evidence-based Review of the Bioenterics Intragastric Balloon for Weight Loss. Obes Surg 2008;18:1611-7. [ Links ]
18. Imaz I, Martínez-Cervell C, García-Álvarez EE, Sendra-Gutiérrez JM, González-Enriquez J. Safety and Effectiveness of the Intragastric Balloon for Obesity. A Meta-analysis. Obes Surg 2008;18:841-6. [ Links ]
19. Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg 2008;107:1543-63. [ Links ]
20. Bordas JM, Campo R, González-Huix F, Igea F, Monés J. Documento de consenso de la Asociación española de Gastroenterología sobre sedoanalgesia en endoscopia digestiva. Gastroenterol Hepatol 2006;29:131-49. [ Links ]
21. Dutta SK, Arora M, Kireet A, Bashandy H, Gandsas A. Upper gastrointestinal symptoms and associated disorders in morbidly obese patients: A prospective study. Dig Dis Sci 2009; 54:1243-6. [ Links ]
22. Schreiner MA, Fennerty B. Endoscopy in the obese patients. Gastroenterol Clin N Am 2010;39:87-97. [ Links ]
23. Kotzampassi K, Eleftheriadis E. Intragastric balloon as an alternative restrictive procedure for morbid obesity. Annals of Gastroenterol 2006;19:285-8. [ Links ]
24. Göttig S, Daskalakis M, Weiner S, Weiner RA. Analysis of safety and efficacy of intragastric balloon in extremely obese patients. Obes Surg 2009;19:677-83. [ Links ]
25. Machytka E, Klvana P, Kornbluth A, Peikin S, Mathus-Vliegen LE, Gostout C, et al. Adjustable Intragastric Balloons: A 12-month pilot trial in endoscopic weight loss management. Obes Surg 2011;21:1499-507. [ Links ]
26. Forestieri P, De Palma GD, Formato A, Giuliano ME, Monda A, et al. Heliosphere® Bag in the treatment of severe obesity: Preliminary experience. Obes Surg 2006;16:635-37. [ Links ]
27. Trande P, Mussetto A, Mirante VG, De Martinis E, Olivetti G, Conigliaro RL, et al. Efficacy, tolerance and safety of new intragastric air-filled balloon (Heliosphere® Bag) for obesity: The experience of 17 cases. Obes Surg 2010;20:1227-30. [ Links ]
28. De Castro ML, Morales MJ, Del Campo V, Pineda JR, Pena E, Sierra JM, et al. Efficacy, safety, and tolerance of two types of intragastric balloons placed in obese subjects: a double-blind comparative study. Obes Surg 2010;20:1642-6. [ Links ]
29. Giardiello C, Borrelli A, Silvestri E, Antognozzi V, Iodice G, Lorenzo M. Air-filled vs. water-filled intragastric balloon: A prospective randomized study. Obes Surg 2012;22:1916-9. [ Links ]
30. Roman S, Napoléon B, Mion F, Bory RM, Guyot P, D Órazio H, et al. Intragastric balloon for "non-morbid" obesity: A Retrospective evaluation of tolerance and efficacy. Obes Surg 2004;14:539-44. [ Links ]
31. Genco A, Cipriano M, Bacci V, Cuzzolaro M, Materia A, Raparelli L, et al. BioEnterics Intragastric Balloon (BIBs): A short-term, double-blind, randomised, controlled, crossover study on weight reduction in morbidly obese patients. International Journal of Obesity 2006;30:129-33. [ Links ]
32. Sallet JA, Marchesini JB, Paiva DS, Komoto K, Pisan CE, Ribeiro MLB, et al. Brazilian multicenter study of the intragastric balloon. Obes Surg 2004;14:991-8. [ Links ]
33. Genco A, Bruni T, Doldi SB, Forestieri M, Marino M, Busetto C, et al. Bioenterics intragastric balloon: The Italian experience with 2515 patients. Obes Surg 2005;15:1161-4. [ Links ]
34. Dastis NS, François E, Deviere J, Hittelet A, Ilah Mehdi A, Barea M, et al. Intragastric balloon for weight loss: Results in 100 individuals followed for at least 2.5 years. Endoscopy 2009;41:575-80. [ Links ]
35. Totté E, Hendrickx L, Pauwels M, van Hee R. Weight reduction by means of intragastric device: Experience with the bioenterics intragastric balloon. Obes Surg 2001;11:519-23. [ Links ]
36. Al-Momen A, El-Mogy I. Intragastric balloon for obesity: A retrospective evaluation of tolerance and efficacy. Obesity Surgery 2005;15: 101-5. [ Links ]
37. Herve J, Wahlen CH, Schaeken A, Dallemagne B, Dewandre JM, Markiewicz S, et al. What Becomes of patients one year after the intragastric balloon has been removed? Obes Surg 2005;15:864-70. [ Links ]
38. Mathus-Vliegen EMH. Intragastric balloon treatment for obesity: What does it really offer? Dig Dis 2008;26:40-4. [ Links ]
39. Escudero Sanchos A, Catalán Serra I, Gonzalvo Sorribes G, Bixquert Jiménez M, Navarro López L. Efectividad, seguridad y tolerancia del balón intragástrico asociado a una dieta hipocalórica para la reducción de peso en pacientes obesos. Rev Esp Enferm Dig 2008;100:349-54. [ Links ]
40. Kotzampassi K, Grosomanidis V, Papakostas P, Penna S, Eleftheriadis E. 500 intragastric balloons: what happens 5 years thereafter? Obes Surg 2012;22:896-903. [ Links ]
41. Provencher V, Perusse L, Bouchard L, Drapeau V, Bouchard C, Rice T, et al. Familial resemblance in eating behaviors in men and women from the Quebec Family Study. Obes Res 2005;13:1624-9. [ Links ]
42. Astrup A, Rossner S. Lessons from obesity management programmes: Greater initial weight loss improves long-term maintenance. Obes Rev 2000;1:17-9. [ Links ]
43. Mazure RA, Bretón I, Cancer E, Mellado C, Abilés V, Avilés J, et al. Balón intragástrico en el tratamiento de la obesidad. Nut Hosp 2009;24:138-43. [ Links ]
![]() Correspondence:
Correspondence:
M.a Luisa de-Castro-Parga.
Department of Gastroenterology.
Hospitalario Universitario de Vigo (CHUVI).
Rúa Pizarro, 22.
36204 Vigo, Pontevedra. Spain
e-mail: maria.luisa.decastro.parga@sergas.es
Received: 20-03-2013
Accepted: 07-10-2013

