










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.8 Madrid dic. 2014
PICTURES IN DIGESTIVE PATHOLOGY
Necrotic left colitis due to hot water enema
Colitis izquierda necrótica por enema de agua caliente
Miguel Ángel Jiménez-Ballester1, Paloma Bebia-Conesa2, Mónica Mengual-Ballester1, María Carrillo-García3, Joana Miguel-Perelló1, Enrique Pérez-Cuadrado-Martínez2 and José Luis Aguayo-Albasini1
Departments of 1General Surgery, 2Gastroenterology and 3Radiology. Hospital Universitario Morales Meseguer, Campus de Excelencia Internacional "Mare Nostrum". Universidad de Murcia. Murcia, Spain
Case report
A 77-year-old man was admitted to emergencies for abdominal pain after instillation of a hot water enema in his home.
On admittance he had a fever of 38 oC, an affected general status, leucocytosis and signs of peritoneal irritation in the lower hemiabdomen. Abdominal CT showed a transmural thickening of the rectosigmoid wall (Fig. 1).

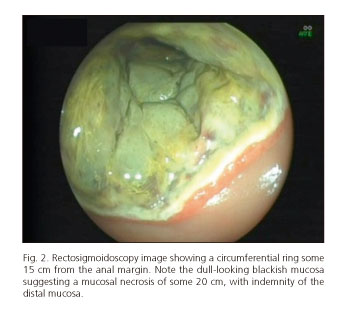
Diagnosed with colitis due to scalding he received a rectosigmoidoscopy at 72 hours (Fig. 2), which from the rectosigmoid junction revealed a necrotic mucosa extending some 15-20 cm. After making good progress he was discharged on the 15th day after admittance.
A month later, the patient presented with rectal tenesmus and episodes of diarrhoea. Colonoscopy revealed an impassable stricture, 3 cm long and some 10 cm from the anus. After two sessions of endoscopic balloon dilatation, which was clinically ineffective, insertion of a biodegradable stent (BDS) was indicated (SX ELLA-BA Stent, Ella CS, Hradec Kralove, Czech Republic). This was fitted 3 months after admittance (Fig. 3) and the patient was asymptomatic a week after insertion and three months (Fig. 4) after degradation of the biodegradable stent (BDS).


Discussion
The most common complication arising from tissue damage due to scalding is the appearance of a cicatricial stricture of the affected segment (1).
The use of a BDP to treat benign cicatricial strictures is generally increasing (2). It could be an intermediate step between balloon dilatation and surgery, but it has still not proved effective for this indication.
In our experience, the use of a BDP after an initial failed attempt at balloon dilatation (3) may be an efficient and alternative technique to surgery (4), although comparative studies are needed to confirm this hypothesis.
References
1. Kim S, Cha JM, Lee CH, Shin HP, Park JJ, Joo KR, et al. Rectal perforation due to benign stricture caused by rectal burns associated with hot coffee enemas. Endoscopy 2012;44:E32-E33. [ Links ]
2. Bong-Hyeon K, Hyung-Jin K, Kang Moon L, Hyeon-Min C. Intractable rectal stricture caused by hot water enema. J Korean Surg Soc 2011;81:350-4. [ Links ]
3. Johansson C. Endoscopic dilation of rectal strictures: A prospective study of 18 cases. Dis Colon Rectum 1996;39:423-8. [ Links ]
4. Garcea G, Sutton CD, Lloyd TD, Jameson J, Scott A, Kelly MJ. Management of benign rectal strictures: A review of present therapeutic procedures. Dis Colon Rectum 2003;46:1451-60. [ Links ]

