










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.8 Madrid dic. 2014
LETTERS TO THE EDITOR
Neuroendocrine carcinoma of the common bile duct
Carcinoma neuroendocrino de vía biliar extrahepática
Key words: Neuroendocrine tumor. Extrahepatic bile ducts. Bile duct resection.
Palabras clave: Tumor neuroendocrino. Conductos biliares extrahepáticos. Resección vía biliar.
Dear Editor,
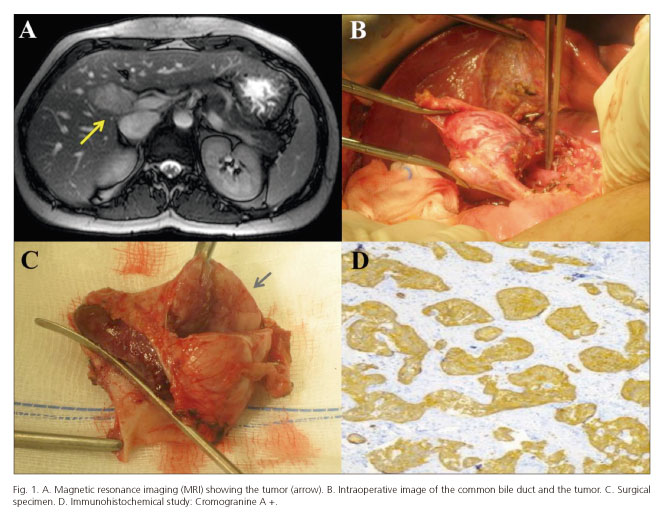
A 37-year-old female patient was admitted to the Emergency department complaining of itching, vomits, diarrhea, and abdominal discomfort for months. On examination the patient presented good general condition, with slight muco-cutaneous pallor, no jaundice, and mild discomfort in lower abdomen. Blood tests revealed an elevation of liver enzymes (GOT 118 UI/l, GPT 215 UI/l, GGT 187 UI/l, and alkaline phosphatase 214 UI/l) without any other alteration in biochemical parameters. Coagulation tests, blood count and tumor markers (alpha-fetoprotein 1.5 ng / ml) were within normal range. An abdominal ultrasound was performed showing a nodular image of 4x3 cm adjacent to the hepatic hilium that compressed the common bile duct at this level and caused dilatation of the intrahepatic bile ducts. The screening was completed with a computed tomography scan (CT) and a magnetic resonance imaging (MRI) (Fig. 1A), which showed an apparently benign mass compressing the common bile duct and hampering bile flow without causing a complete obstruction of the bile duct. The patient underwent surgical exploration, finding a large tumor solely dependent of the common bile duct (Fig. 1B), with no hepatic infiltration (proved with intraoperative ultrasound). A resection of the bile duct, from the upper pancreatic edge to the bile ducts confluence at the hepatic hilium, was performed (Fig. 1C), with a lymphadenectomy and a Roux-en-Y hepaticojejunostomy. The patient had a favorable postoperative recovery and was discharged without complications. Histological study informed of a well diferentiated neuroendocrine carcinoma of the common bile duct, TNE G2 (mitotic index: 3x10 HPF, Ki-67 3 %), with free margins and no nodal infiltration. Typical immunohistochemical properties were positive: chromogranin A +, synaptophysin+, CD56 +, CK AE1/AE3 + (Fig. 1D).
Discussion
Biliary neuroendocrine tumors (NETs) are extremely rare, accounting for 0.1 %-2 % of all gastrointestinal neuroendocrine tumors (1). The most common anatomical locations are the common bile duct (58 %), perihiliar (28 %), cyst duct (11 %) and common hepatic duct (3 %). They are more prevalent in women, during the fifth decade of life (2,4).
Although NETs may be hormonally active, most cases are not-functioning and the symptoms result from bile duct obstruction, like itching or biliary colic, which is difficult to be identified on imaging studies. The submucosal location of these tumors determines a large number of false negative results on brush biopsy, making it difficult to achieve a correct preoperative diagnosis. Differential diagnosis must be established with other hepatic and biliary tumors. The definitive diagnosis is established by histopathological and immunohistochemical analysis of the surgical specimen (3,5).
Radical resection of the tumor is the main prognostic factor in patients with biliary NETs. Complete resection of the extrahepatic bile ducts with a biliodigestive reconstruction (Roux-en-Y hepaticojejunostomy) with portal lymphadenectomy must be performed, that achieves a long-term high survival rate. Large tumors that infiltrate the proximal pancreas may require a cephalic duodenopancreatectomy.
José Aurelio Navas-Cuéllar, José María Álamo-Martínez, Carmen Bernal-Bellido, Beatriz Martín-Pérez,
Luis Miguel Marín-Gómez, Gonzalo Suárez-Artacho, Juan Serrano-Díez-Canedo,
Miguel Ángel Gómez-Bravo and Javier Padillo-Ruiz
Hepatobiliopancreatic Surgery and Transplantation Unit
Department of General Surgery and Digestive Diseases
University Hospital Virgen del Rocío. Seville, Spain
References
1. Sethi H, Madanur M, Srinivasan P, Portmann B, Heaton N, Rela M. Non functioning well-differentiated neuroendocrine tumor of the extrahepatic bile duct: An unusual suspect? Hepatobiliary Pancreat Dis Int 2007;6:549-52. [ Links ]
2. Kim DH, Song MH, Kim DH. Malignant carcinoid tumor of the common bile duct: Report of a case. Surg Today 2006;36:485-9. [ Links ]
3. Caglikulekci M, Dirlik M, Aydin O, Ozer C, Colak T, Dag A, Canbaz H, Aydin S. Carcinoid tumor of the common bile duct: Report of a case and a review of the literature. Acta Chir Belg 2006;106:112-5. [ Links ]
4. Nafidi O, Nguyen BN, Roy A. Carcinoid tumor of the common bile duct: A rare complication of von Hippel-Lindau syndrome. World J Gastroenterol 2008;14:1299-301. [ Links ]
5. Tallón-Aguilar L, Jurado-Marchena R, Tejada-Gómez A, Balongo-García R, Naranjo-Rodríguez PL. Ampullary carcinoid tumor. An atypical location. Rev Esp Enferm Dig 2012;104:335-6. [ Links ]

