










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.9 Madrid sep. 2015
LETTERS TO THE EDITOR
Acute gastric dilatation in the context of bulimia nervosa
Key words: Acute gastric dilatation. Total gastrectomy. Gastric necrosis. Bulimia nervosa.
Dear Editor,
Acute gastric dilatation is scarcely reported in the literature. Gastric necrosis is extremely uncommon due to the rich blood supply of the stomach. A rare complication of eating disorders is the acute gastric dilatation with necrosis. However, it can occur after large intake of food over a short period of time (1-3).
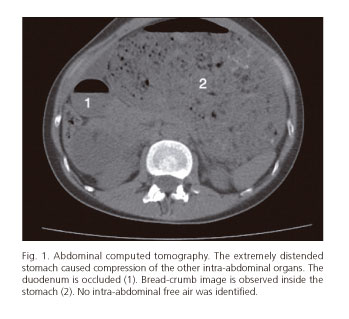
We report a case of a 36 year-old woman that arrived at the emergency room with a sudden onset of epigastric pain that had generalized throughout the abdomen. The patient had had a large intake of food 24 hours before admission. On examination, she was hemodynamically stable, showing a painful, tympanic, and distended abdomen, with signs of peritoneal irritation. The complete blood count revealed neutrophilic leukocytosis without electrolytic disorders. Abdominal X-ray and abdominal CT scan revealed a massive and dilated stomach occupying from the diaphragm to the iliac bone (Fig. 1).
Initial treatment included fluid therapy, analgesia and placement of nasogastric tube. Given the progressive clinical deterioration of the patient, emergency surgery was performed. A massive gastric distension was observed, along with extensive necrosis of the posterior wall and gastric fundus, and patchy necrosis throughout the greater curvature (Fig. 2). The patient underwent total gastrectomy and esophagojejunostomy. The patient was assessed by psychiatrists and admitted for treatment of the eating disorder and was discharged without complications. The total gastrectomy specimen was massively dilated and necrotic, measuring 40 cm along the greater curvature and 11 cm along the lesser curvature.

Acute gastric dilation with necrosis has been described in re-feeding after starvation, diabetes mellitus, bezoars, gastrointestinal tumours, gastric volvulus, gastroduodenal Crohn's disease, etc. (4). Patients with anorexia nervosa and bulimia nervosa have altered gastric motility in approximately 60% of the cases, which makes them prone to developing severe gastric dilatation (5).
Initial treatment with nasogastric tube decompression normally obtains satisfactory results. The use of the endoscope is scant because the gastric contents are usually too dense to be drawn out and there is also a high risk of perforation (6).
The most serious complication is perforation of the gastric wall due to necrosis (3), which is an emergency requiring surgery. Usually, a partial gastrectomy can be performed, preserving most of stomach (7), but there are cases with so extensive necrosis that a total gastrectomy is required (8). This case illustrates that one-stage resection with esophago-jejunostomy can be successful under favourable circumstances.
There are other possible complications, such as intestinal ischemia or bacterial cerebral aneurysm formation (9). Recently, a case of acute limb ischemia secondary to an acute gastric dilatation causing compression of the common iliac arteries has been reported (10).
In cases of acute gastric dilatation without necrosis or perforation mortality may reach 15.4%, so monitoring should be close after decompression. Once gastric necrosis or perforation occurs, mortality rates of up to 73% have been reported (4).
In conclusion, acute gastric dilatation is a condition to be considered in patients with eating disorders. The suspected diagnosis and early management can avoid complications and decrease mortality substantially.
Jorge Panach-Navarrete1, David Moro-Valdezate1, Marina Garcés-Albir1,
Luis Barreda-Estuardo2, Marta M. Bosca-Watts2 and Joaquín Ortega-Serrano1
1General and Digestive Surgery Department.
2Digestive Medicine Department.
Hospital Clínico Universitario de Valencia. Valencia, Spain
References
1. Mishima T, Kohara N, Tajima Y, et al. Gastric rupture with necrosis following acute gastric dilatation: Report of a case. Surg Today 2012;42:997-1000. DOI: 10.1007/s00595-012-0162-4. [ Links ]
2. Nakao A, Isozaki H, Iwagaki H, et al. Gastric perforation caused by a bulimic attack in an anorexia nervosa patient: Report of a case. Surg Today 2000;30:435-7. DOI: 10.1007/s005950050618. [ Links ]
3. Watanabe S, Terazawa K, Asari M, et al. An autopsy case of sudden death due to acute gastric dilatation without rupture. Forensic Sci Int 2008;180:6-10. DOI: 10.1016/j.forsciint.2008.07.005. [ Links ]
4. Franken EA, Jr, Fox M, Smith JA, et al. Acute gastric dilatation in neglected children. AJR Am J Roentgenol 1978;130:297-9. DOI: 10.2214/ajr.130.2.297. [ Links ]
5. Hadley SJ, Walsh BT. Gastrointestinal disturbances in anorexia nervosa and bulimia nervosa. Curr Drug Targets CNS Neurol Disord 2003;2:1-9. DOI: 10.2174/1568007033338715. [ Links ]
6. Luncă S, Rikkers A, Stănescu A. Acute massive gastric dilatation: Severe ischemia and gastric necrosis without perforation. Rom J Gastroenterol 2005;14:279-83. [ Links ]
7. Arenal-Vera JJ, Cendoya-Ansola I, Álvarez-Cuesta LJ, et al. Necrosis of the greater curvature following acute dilatation of the stomach. Rev Esp Enferm Dig 1991;80:405-7. [ Links ]
8. Tamayo M, Lage A, Agea Q. Cirugía conservadora de la necrosis gástrica tras crisis de bulimia. Cir Esp 2002;71:161-2. DOI: 10.1016/S0009-739X(02)71951-9. [ Links ]
9. Matsuyama T, Komeda S, Nobayashi M, et al. Acute gastric dilatation causing bacterial cerebral aneurysm - case report. Int J Eat Disord 2008;41:380-2. DOI: 10.1002/eat.20487. [ Links ]
10. Van Eetvelde E, Verfaillie L, Van de Winkel N, et al. Acute gastric dilatation causing acute limb ischemia in an anorexia nervosa patient. J Emerg Med 2014;46:e141-3. DOI: 10.1016/j.jemermed.2013.11.093. [ Links ]

