










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.4 Madrid abr. 2017
https://dx.doi.org/10.17235/reed.2016.4403/2016
CASE REPORT
Jejunal pseudodiverticulosis. Three cases report
Pseudodiverticulosis yeyunal. A propósito de tres casos
Beatriz Laiz-Díez1, Juan González-González1, Jaime Ruiz-Tovar1, Javier López-Monclús2 and Manuel Durán-Poveda1
1Department of General and Digestive Surgery. Hospital Universitario Rey Juan Carlos I. Móstoles, Madrid. Spain.
2Department of General and Digestive Surgery. Hospital Universitario Puerta de Hierro Majadahonda. Majadahonda, Madrid. Spain
ABSTRACT
Jejunal pseudodiverticulosis is an uncommon entity. Pseudodiverticulum are usually asymptomatic and an incidental finding. They can have a less frequent acute onset with perforation, obstruction or bleeding and they could have high morbidity and mortality. We report three patients who debuted with an acute abdomen.
Key words: Jejunal psedodiverticulosis. Intestinal obstruction. Intestinal perforation.
RESUMEN
La pseudodiverticulosis yeyunal es una entidad infrecuente que cursa habitualmente de forma asintomática. Cuando produce sintomatología, en muchas ocasiones es como resultado de sus complicaciones (obstrucción, perforación o sangrado) y asocia una elevada morbimortalidad. Presentamos tres casos que debutaron como un cuadro de abdomen agudo.
Palabras clave: Pseudodiverticulosis yeyunal. Obstrucción intestinal. Perforación intestinal.
Case report
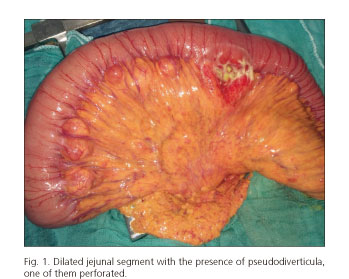
We present three cases of jejunal pseudodiverticulosis with onset symptoms of an acute abdomen. First, we present a 75-year-old male patient with a clinical history of intestinal obstruction. CT scan showed a firm bowel adhesion or internal hernia, thus a surgical treatment was proposed. Secondly, a 90-year-old female patient who was admitted to the Emergency Department with an acute history of vomiting; a CT scan did not show any evidence of an obstructive etiology. Twenty-four hours later the patient suffered a clinical deterioration, with evidence of pneumoperitoneum in a new CT scan; therefore, a surgical intervention was decided upon. The third case is of a 75-year-old male patient who was admitted to the emergency department with a clinical history of abdominal pain. A CT scan showed a perforation of the small bowel diverticula, thus a surgical intervention was performed. An intestinal obstruction with proximal jejunal pseudodiverticula was found during surgery for cases 1 and 2. Cases 2 and 3 presented free perforation of the pseudodiverticula. Surgical treatment consisted of the resection of the affected intestinal loop followed by primary enteroenteric anastomosis. No complications occurred in the postoperative period for any of the patients. Pathologic studies showed the presence of false diverticulum in the jejunum, with anti-mesenteric perforations in two cases without any signs of malignancy.
Discussion
Jejunal pseudodiverticulosis is an uncommon entity (incidence between 0.06-1.5%) (1,2), and is more frequent in males (53%) between the 6th and 7th decades of life (2,3).
Pseudodiverticula originate in the herniation of mucosa and submucosa throughout the muscular layer. This herniation occurs in the points of penetration of the mesenteric microvessels through the intestinal wall. This herniation is secondary to a hyper-pressure in the intestinal lumen (1,2,4). The pseudodiverticula size is variable, their typical location is in the proximal jejunum (1,2) and they can coexist with other pseudodiverticula in the gastrointestinal tract (2,3).
Pseudodiverticula are usually asymptomatic and an incidental finding. Nevertheless, they can cause non-specific abdominal discomfort, dyspepsia and malabsorption. Less frequently, they display an acute onset with perforation, obstruction or bleeding (1-5).
Conservative management should be performed in the absence of complications (3). Surgical management should be offered in complicated cases; intestinal resection and primary anastomosis is the treatment of choice.
References
1. Aydin I, Pergel A, Yucel AF, et al. A rare cause of acute abdomen: Jejunal diverticulosis with perforation. J Clin Imaging Sci 2013;3:31. DOI: 10.4103/2156-7514.115763. [ Links ]
2. Singal R, Gupta S, Airon A. Giant and multiple jejunal diverticula presenting as peritonitis a significant challenging disorder. J Med Life 2012;15;5(3):308-10. [ Links ]
3. Hanna C, Mullinax J, Friedman MS, et al. Jejunal diverticulosis found in a patient with long-standing pneumoperitoneum and pseudo-obstruction on imaging: A case report. Gastroenterol Rep 2015; pii:gov033. DOI: 10.1093/gastro/gov033. [ Links ]
4. Socas M, Rodríguez J, Flores M, et al. Severe gastrointestinal bleeding associated to massive jejunal diverticulosis and Sintrom® treatment. Rev Esp Enferm Dig 2005;97(1):57-8. DOI: 10.4321/S1130-01082005000100007. [ Links ]
5. Kassir R, Boueil-Bourlier A, Baccot S, et al. Jejuno-ileal diverticulitis: Etiopathogenicity, diagnosis and management. Int J Surg Case Rep 2015;10:151-3. DOI: 10.1016/j.ijscr.2015.03.044. [ Links ]
![]() Correspondence:
Correspondence:
Beatriz Laiz Díez.
Department of General and Digestive Surgery.
Hospital Universitario Rey Juan Carlos I.
C/ Gladiolo, s/n.
28933 Móstoles, Madrid. Spain
e-mail: bealaiz@hotmail.com
Received: 27-04-2015
Accepted: 04-05-2016
