










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.6 Madrid jun. 2017
PICTURES IN DIGESTIVE PATHOLOGY
A giant hiatal hernia and intrathoracic pancreas
Hernia hiatal gigante y páncreas intratorácico
Ismael Mora-Guzmán1, Juan Antonio del-Pozo-Jiménez2 and Elena Martín-Pérez1
Services of 1General Surgery and Digestive Diseases, and 2Radiodiagnosis. Hospital Universitario de La Princesa. Madrid, Spain
Case report
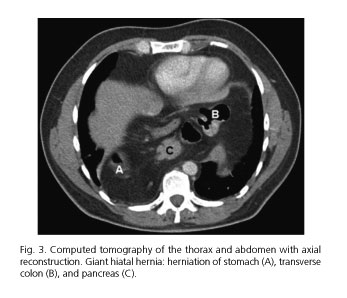
A 49-year-old man with a history of a hiatal hernia and gastroesophageal reflux that had been diagnosed six years earlier presented with cough, dysphagia and dyspnea. A chest radiography (Fig. 1) showed mediastinal air fluid levels above the cardiac contour, suspicious of the presence of intrathoracic hollow organs. Abdominal computed tomography (Figs. 2 and 3) revealed an 8 cm-diaphragmatic hiatus and a giant hiatal hernia with an intrathoracic displacement involving non-ischemic partially volvulated stomach, the transverse colon and part of the body and tail of the pancreas. A surgical repair was performed and the visceral contents of the hernia sac were reduced, the diaphragmatic pillars were fixed and a Toupet fundoplication was performed. The postoperative course was uneventful and the patient was discharged on postoperative day five.


Discussion
Type IV hiatal hernia is the most uncommon type of hiatal hernias (less than 5%), originating from a large defect of the diaphragmatic hiatus and characterized by the presence of abdominal organs other than the stomach (1,2). The presence of the pancreas at this location is very uncommon, and around ten cases have been reported. Only two patients had the pancreas and transverse colon herniated together (2). Most cases involve a symptomatic presentation as acute pancreatitis or other symptoms (2,3). Multidetector computed tomography is the modality of choice that allows the visualization of the anatomy and size of the hiatus defect (3). The treatment of choice is surgical repair for symptomatic cases, and surgery may be recommended for asymptomatic patients with pancreatic herniation in order to prevent potential complications (1).
References
1. Saxena P, Konstantinov IE, Koniuszko MD, et al. Hiatal herniation of the pancreas: Diagnosis and surgical management. J Thorac Cardiovasc Surg 2006;131:1204-5. DOI: 10.1016/j.jtcvs.2006.01.008. [ Links ]
2. Jäger T, Neureiter D, Nawara C, et al. Intrathoracic major duodenal papilla with transhiatal herniation of the pancreas and duodenum: A case report and review of the literature. World J Gastrointest Surg 2013;5:202-6. DOI: 10.4240/wjgs.v5.i6.202. [ Links ]
3. Lal A, Gupta P, Sinha SK. An unusual cause of abdominal pain in an elderly woman. Gastroenterology 2015;148:e11-2. DOI: 10.1053/j.gastro.2014.11.036. [ Links ]
