










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The serial transverse enteroplasty procedure (STEP) is an intestinal lengthening procedure originally applied in pediatric patients with short bowel syndrome (SBS) and dilatation of the remnant small bowel. This increases the likelihood of achieving enteral autonomy while avoiding the need for intestinal transplantation 1) (2. Its application in adults has been reported in the literature 3. This technique increases bowel length via the application of sequential stapling on alternating sides in a plane perpendicular to the long axis of the bowel. The end result is the creation of a channel of bowel approximately twice the length and half the diameter of the original segment. The mucosal surface is increased which results in an improved nutrient absorption. Furthermore, tapering of the dilated intestine improves bowel motility, thus reducing the risk of bacterial overgrowth.
Although the duodenum is a challenging segment in autologous gut reconstruction due to its close proximity to bilio-pancreatic structures and the blood supply shared with the pancreas. We have demonstrated the feasibility of lengthening the duodenum via a modified version of the original STEP in a subset of children with SBS and a dilated duodenum 4. Serial transverse duodenoplasty not only gains an additional intestinal length when combined with simultaneous STEP but can also be applied successfully in patients with ultra-SBS. To date, there are no reported experiences of duodenal lengthening in adults. Herein, we report the first successful application of this novel technique in an adult with ultra-SBS and a dilated duodenum.
CASE REPORT
A 25 year old man with extreme SBS on total parenteral nutrition (TPN) secondary to mid-gut volvulus at the age of 19 was referred to our center for intestinal transplant evaluation. The patients´ weight and height were 48 kg and 166 cm, respectively. In addition, he was diagnosed with type 1 diabetes at the age of 4 and had already developed incipient nephropathy in the form of microalbuminuria. Surgical treatment at the time of the intestinal catastrophe consisted of the removal of the fourth part of the duodenum, the whole jejunum, ileon and ascending colon. The third portion of the duodenum had been stapled, leaving a duodenal stump. Moreover, a colonic mucous fistula was created at the level of the transverse colon hepatic flexure. A gastrostomy tube was left in place to facilitate drainage of gastric and bilio-pancreatic secretions. The patient developed acute renal failure postoperatively and required hemodialysis for three months. One year later, he developed cholestasis (direct bilirubin of 7 mg/dl). The liver dysfunction was resolved via optimization of the parenteral formula.
Prior to surgery, he had a history of 3 central-line infections and was colonized by multi-resistant Klebsiella pneumoniae. The gastrostomy tube output ranged from 2.5 to 4 liters/day with TPN requirements of 3 liters/day (1,500 calories/day) administered for 18 hours and an additional 1.5-2 liters per day of I.V fluids for the remaining time. Therefore, the overall time of parenteral nutrition (PN) and I.V. fluid administration was 24 hours. Despite meticulous insulin dosage management, the control of blood glycemia levels was extremely complex with frequent episodes of hypo-hyperglycemia. Hypoglycemia during the PN-free period necessitated I.V. glucose administration. Creatinine clearance was 46 ml/min/BSA. Serum liver function test was as follows: aspartate transaminase at 36 IU/L, alanine transaminase at 54 IU/L and gamma-glutamyl transpeptidase at 135 IU/L. In addition, the plasma citrulline level was 13.6 micromol/L. Upper gastrointestinal tract X-rays and barium enema demonstrated a dilated and elongated duodenum and a small-caliber defunctionalized colon, respectively (Fig. 1 A and Fig. B). Due to the clinical scenario, the patient was placed on the intestinal transplant list combined with pancreas and kidney allografts. Nevertheless, due to our prior successful experience with duodenal lengthening procedures in children 4, the patient asked to be considered for duodenal lengthening.

Fig. 1 A. Upper gastrointestinal series prior to the duodenal lengthening procedure showing the massively dilated duodenum ending in a stump. B. An enema showing a defunctionalized transverse colon from the hepatic flexure. C. Upper gastrointestinal series one week after duodenal lengthening and a duodeno-colic anastomosis.
Written informed consent was obtained from the patient prior to the procedure. Prophylactic preoperative I.V. antibiotics were administered. An iterative mid-line incision was made under general anesthesia. A Kocher maneuver was performed to mobilize the duodenum. The length of the retained duodenum measured from the pylorus was 30 cm. The colonic mucous fistula was taken down and stapled with the construction of an end-to-side duodeno-colonic anastomosis. Duodenal lengthening was performed with 7 sequential transverse applications (5 of 45 mm and 2 of 60 mm) of an endoscopic stapler (Endo GIA Stapler, Covidien LLC, Mansfield, MA, USA) on the duodenal anterior and posterior walls, respecting the pancreatic parenchyma as described elsewhere 4 (Fig. 2). The final length of the duodenum after the procedure reached 83 cm (Fig. 3). The vertexes of the cutting line were reinforced with a 3-0 vicryl U stitch to prevent duodenal leaks. A Jackson-Pratt drain was placed to detect postoperative leakage. The postoperative course was uneventful. Antibiotics were administered postoperatively for 3 days. A radiologic gastrointestinal contrast study on the 7th postoperative day ruled out stricture or leakage before the initiation of enteral nutrition (Fig. 1C) and the Jackson-Pratt drain was removed the same day. The patient was discharged in a good condition 26 days post-surgery.

Fig. 2 The first stapler firing was applied on the anterior aspect of the duodenum, 2 cm away from the pylorus. The next firing was similar from the opposite side, creating a duodenal channel 3 cm in diameter. The procedure was repeated approximately every 3-4 cm until the duodeno-colonic anastomosis was reached.
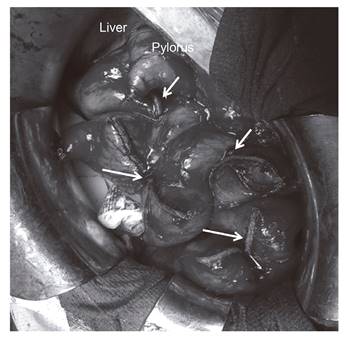
Fig. 3 Intraoperative image of the duodenum after the lengthening procedure showing the cutting and stapled lines (arrows) on the anterior wall of the duodenum. The lengthened duodenum measured 83 cm.
At 12 months post-surgery, citrulline plasma level had increased to 21.6 micromol/L. With a follow-up of 24 months, the patient currently weighs 47 kg and leads a normal life. He is on a PN support volume of 1,750 ml and 500 ml of I.V. fluids administered for 9 hours during the night. He also follows an oral low-fiber diet ad libitum. Calorie requirements have dropped to 800 calories/day and bowel movement frequency is 2-3 per day. Creatinine clearance has remained unchanged from that observed prior to surgery and the liver function test is normal. Apart from insulin, the only drugs administered are proton pump inhibitors. Glycemia control continues to be as difficult as that experienced before surgery. Although, the patient is able to successfully treat hypoglycemia episodes via the oral route.
DISCUSSION
Due to the high risk of death, patients with ultra-SBS are considered potential candidates for a preemptive/rehabilitative intestinal transplantation 5. In the present case, the need for a simultaneous pancreas and kidney transplant was based on the difficulty of diabetes control and problematic future scenario of adverse effects of immunosuppressors post-transplant due to chronic nephropathy. Nevertheless, the use of intestinal transplantation has declined in recent years due to the associated high morbidity and mortality that lead to poorer survival than that seen in patients on home PN 5) (6. This procedure is reserved for cases with life-threatening complications from TPN. Therefore, whenever possible, autologous intestinal reconstruction should be considered before intestinal transplantation.
The restoration of intestinal tract continuity is one of the mainstays of autologous gut reconstruction to obtain the absorptive and digestive properties of the colon. However, the benefit of the procedure in the present case was questionable due to a complete absence of the small bowel and the presence of an incomplete megaduodenum. Similarly, the improvement in quality of life was questionable as the high gastrostomy output could result in a significant postoperative diarrhea following the establishment of the continuity of the intestinal tract.
Megaduodenum facilitates pyloric incompetence with alkaline reflux and dysmotility with stasis of intraluminal contents which may result in bacterial overgrowth and malabsorption. The classical standard duodenal tapering technique reduces the luminal diameter of the dilated duodenum by removing its anti-pancreatic border longitudinally, usually with stapler devices 8. The main advantage of this new technique is that an additional intestinal absorptive surface is obtained without the need to discard any duodenal portion. The most critical surgical issue is the prevention of damage to the biliary and pancreatic ducts. Since these anatomical structures are situated inside the thickness of the pancreatic parenchyma, the risk of injury is circumvented by stapling the anterior and posterior aspects of the duodenum at a sufficient distance from the pancreas.
Although this young man may require an intestinal transplant in the future, the application of this procedure has resulted in an enormous social and psychological benefit as well as the avoidance of immunosuppression therapy. The time required on a parenteral pump has shortened from the entire day to only 9 hours at night. In addition, the volume requirements were also reduced to less than half, with no negative impact on renal function.
One question arises regarding the role of this surgical technique in the adaptation process. Measurement of plasma citrulline (a non-protein amino acid mainly produced by enterocytes of the small bowel) has been proposed as a biomarker of remnant small bowel mass and predicts permanent versus transient intestinal failure 9) (10. In a study of 57 patients with SBS, a level of < 20 micromol/L was associated with patients with a permanent intestinal failure. The positive and negative predictive values were 95% and 86%, respectively 10. In the present case, the pre-lengthening citrulline level had increased from 13.6 micromol/L to 21.6 micromol/L one year post-lengthening, which is above the cut-off for permanent intestinal failure. Similarly, there was evidence that the absorptive surface had increased, as the calorie requirement decreased by half after surgery and is currently only 50% of the basal calorie requirement.
In summary, although this is only one case, the result obtained demonstrates the feasibility and effectiveness of duodenal tapering and lengthening as part of the autologous intestinal reconstruction armamentarium in adults with a dilated duodenum and SBS.

