










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkCASE REPORT
A 56-year-old man was referred to our department for treatment of a mass in the duodenal bulb. Esophagogastroduodenoscopy (EGD) showed a large spherical mass extending from the pyloric canal to the anterior wall of the duodenal bulb (Fig. 1A). Endoscopic ultrasonography revealed a submucosal mass with heterogeneous echogenicity and a cystic structure (Fig. 1B). Computed tomography (CT) showed a solid cystic mass with rim enhancement and a lack of enhancement in the cystic spaces (Fig. 1C). The patient underwent an endoscopic submucosal dissection (ESD), which was uneventful, and a 4 × 3 × 2 cm mass was removed (Fig. 1D).
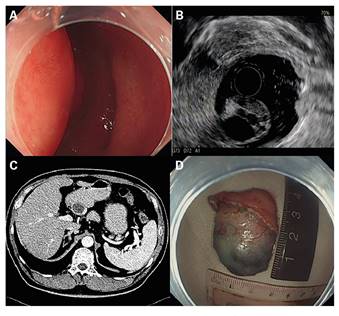
Fig. 1 A. EGD identified a large spherical mass measuring 4 cm in diameter with a clear border, which extended from the pyloric canal to the anterior wall of the duodenal bulb. B. Endoscopic ultrasonography revealed a submucosal mass with heterogeneous echogenicity and a cystic structure. C. CT identified a solid cystic mass with rim enhancement and lack of enhancement in the cystic spaces. D. The patient underwent ESD, which was uneventful, and a 4 × 3 × 2 cm mass was removed.
Histologically, the mass was composed of hyperplastic Brunner's glands (Fig. 2A) and cystic dilations (Fig. 2B). The cysts were lined with a single layer of columnar epithelium similar to Brunner's gland ducts. Brunner's glands cystadenoma was the final diagnosis.

DISCUSSION
Brunner's glands cystadenoma is extremely rare and only two cases have been reported previously 1) (2. The pathogenesis is unclear and a primary tumor in the duodenum may be asymptomatic or cause an obstruction or gastrointestinal hemorrhage. White light endoscopy and CT scan have limitations for diagnosis due to nonspecific features. Endoscopic ultrasonography has an important role in identifying the origin. Cystadenomas have a potential risk of malignancy when they arise from the ovaries or pancreas 3. A large mass may lead to symptoms of obstruction and surgical or endoscopic resection is recommended.
