










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 no.9 Madrid sep. 2018
https://dx.doi.org/10.17235/reed.2018.5563/2018
CASE REPORTS
Endoscopic closure of tracheoesophageal fistula for tuberculosis with an over-the-scope-clip
1Unidad de Gastroenterología y Endoscopia Digestiva. Hospital Pablo Tobón Uribe. Medellín, Colombia
INTRODUCTION
The over-the-scope-clip (OTSC(r), Ovesco system) is a clipping device made of nitinol. The clip is mounted on a cap in the distal tip of the endoscope, similar to variceal ligation band. OTSC(r) has been approved for human use in Europe since 2009 and in the United States since 2010 1,2. This system provides a closing force as tight as a manual suture in porcine models ex vivo 3). It can grasp all layers of the visceral wall and this in turn leads to a full thickness scarring, without causing adhesions 4.
The most common use of OTSC(r) include gastrointestinal (GI) iatrogenic perforations, anastomosis leaks, correction of bariatric surgery fistulae, digestive bleeding and the closure of natural orifices transluminal endoscopic surgery (NOTES) 4. There are few case reports on the use of OTSC(r) for the treatment of tracheoesophageal fistula 5,6,7. There are no described cases to date of tracheoesophageal fistula closure with OTSC(r) in a patient with tuberculosis and HIV-AIDS infection.
CASE REPORT
A 39-year-old male with a history of MSM (men who have sex with men) presented to the Emergency Department due to a dry cough of a three week duration, which worsened after the ingestion of food or fluids. He reported fever, chills, asthenia, fatigue, anorexia and a 5 kg non-voluntary weight loss during the last month. Physical examination identified mucocutaneous pallor and emaciation (weight: 53 kg; height: 167 cm; body mass index [BMI]: 19 kg/m2) with bibasal rhonchus. The patient was hospitalized in order to perform biochemical studies (Table 1).

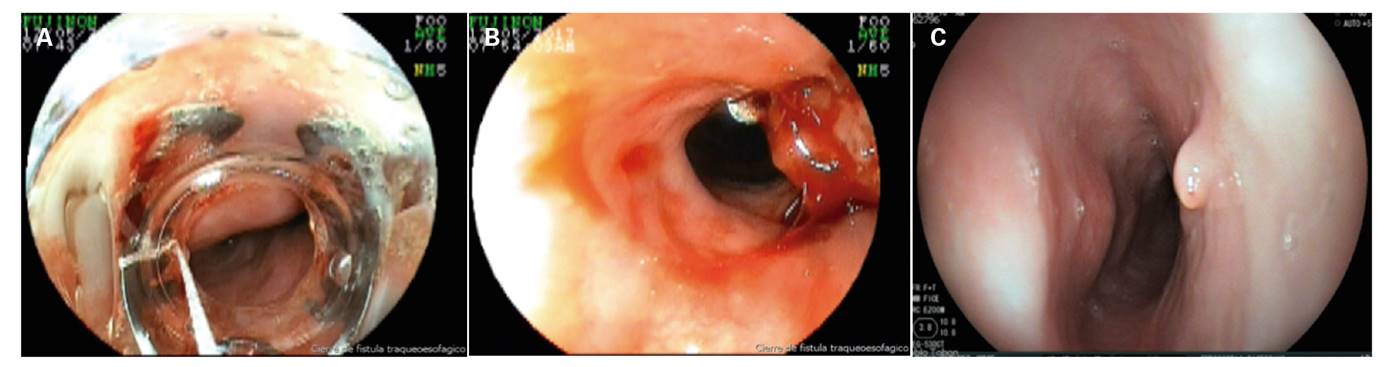
Upper digestive endoscopy identified an orifice with a diameter of 2 cm and marked inflammatory changes at 30 cm from the dental arches; biopsies were also taken (Fig. 1A). A tracheoesophageal fistula was identified via a barium esophagogram (Fig. 1B). Based on these findings, a SEMS was placed. A new endoscopy was performed three days later due to the persistence of symptoms and a SEMS migration into the stomach was identified. The stent was removed and the fistulae closed with an OTSC(r) (Fig. 2A and Fig. B).
Pathology and secretion reports confirmed TB. Anti-tuberculous (isoniazid 300 mg, rifampicin 600 mg, pyrazinamide 1,500 mg and ethambutol 1,200 mg) and antiretroviral (efavirenz 600 mg and tenofovir/emtricitabine 300 mg/200 mg) therapy was initiated with an adequate tolerance. The patient was discharged two weeks later with improvement of symptoms and an adequate oral tolerance. A complete closure of the fistulae was observed six months later during the endoscopic control (Fig. 2C) and the patient was asymptomatic.
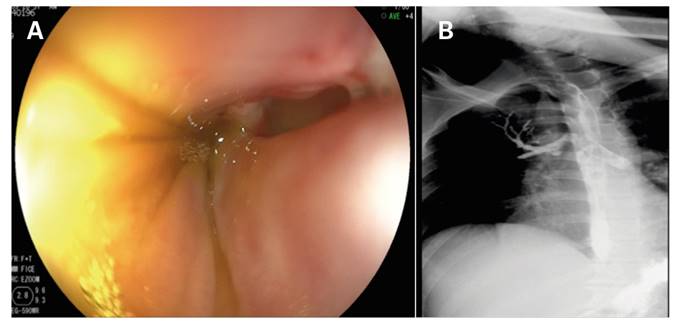
Fig. 1 Active traqueoesophageal fistulae. A. Endoscopic appearance, inflammatory changes and a purulent secretion. B. Esophagogram with an evident contrast leakage to the tracheobronchial tree.
DISCUSSION
Tracheoesophageal fistulae are an abnormal junction between the trachea and the esophagus. It can occur secondary to trauma, neoplasia, necrosis due to prolonged intubation, a rigid nasogastric tube insertion or iatrogenic endoscopic perforations and surgery. Less common causes have been described such as esophagotracheal tuberculosis. There are few reports in the literature of HIV and tuberculosis infection related tracheoesophageal fistulae. Most underwent surgical management, some with endoscopic stenting and only one had a conservative management with percutaneous endoscopic gastrostomy with parenteral nutrition 8,9,10. Conservative treatments with successful outcomes have been reported in small series 10. However, this involves the use of antiretroviral drugs in parenteral or liquid presentation for administration via gastrostomy. Unfortunately, the latter is not available in our center. In addition, there are no guarantees of a successful closure of large defects.
The chronic tracheoesophageal fistulae approach involves thoracotomy for surgical closure of the lesion in most cases. However, this procedure carries a high risk in patients with a poor nutritional status and global deterioration 9,10. Endoscopic stenting has also been used but with unsatisfactory outcomes due to SEMS migration and also local complications such as a worsening of the tracheoesophageal fistulae. However, the experience with stenting in TB-related fistulas has not yet been described.
In our patient, we first placed an esophageal SEMS but this did not resolve the clinical situation, as it migrated. Therefore, OTSC(r) was used as a closure measure of the defect and a complete resolution of the symptoms. The OTSC(r) system is a promising method for the treatment of multiple GI pathologies. It could play an important role in fistulae closure in patients with multiple comorbidities and non-surgical candidates.
BIBLIOGRAFÍA
1. Banerjee S, Barth BA, Bhat YM, et al. Endoscopic closure devices. Gastrointest Endosc 2012;76(2)244-51. DOI: 10.1016/j.gie.2012.02.028 [ Links ]
2. Angsuwatcharakon P, Prueksapanich P, Kongkam P, et al. Efficacy of the Ovesco clip for closure of endoscope related perforations. Diagn Ther Endosc 2016;1-6. DOI: 10.1155/2016/9371878 [ Links ]
3. Voermans RP, Vergouwe F, Breedveld P, et al. Comparison of endoscopic closure modalities for standardized colonic perforations in a porcine colon model. Endoscopy 2011;43(3)217-22. DOI: 10.1055/s-0030-1256072 [ Links ]
4. Junquera F, Martínez-Bauer E, Miquel M, et al. OVESCO: un sistema prometedor de cierre endoscópico de las perforaciones del tracto digestivo. Gastroenterol Hepatol 2011;34(8):538-72. DOI: 10.1016/j.gastrohep.2011.05.007 [ Links ]
5. Bilge U, Salih M, Yalaki S. Endoscopic closure of tracheoesophageal fistulas with the over-the-scope clip system. J Coll Physicians Surg Pak 2014;24(3):S193-5. [ Links ]
6. Monkemuller K, Peter S, Toshniwal J, et al. Multipurpose use of the "bearclaw" (over-the-scope-clip system) to treat endoluminal gastrointestinal disorders. Dig Endosc 2014;26(3):350-7. DOI: 10.1111/den.12145 [ Links ]
7. Traina M, Curcio G, Tarantino I, et al. New endoscopic Over-the-scope clip system for tracheoesophageal fistula. Endoscopy 2010;42:E54-5. DOI: 10.1055/s-0029-1243824 [ Links ]
8. Rosario P, Song J, Wittenborn W, et al. Tracheoesophageal fistula in AIDS: stent versus primary repair. AIDS Patient Care STDs 1996;10:334-5. DOI: 10.1089/apc.1996.10.334 [ Links ]
9. Devarbhavi HC, Alvares JF, Radhikadevi M. Esophageal tuberculosis associated with esophagotracheal or esophagomediastinal fistula: report of 10 cases. Gastrointest Endosc 2003 ;57(4):588-92. DOI: 10.1067/mge.2003.140 [ Links ]
10. Pagano G, Dodi F, Camera M, et al. Tubercular tracheoesophageal fistulas in AIDS patients: primary repair and no surgery required? AIDS 2007;21(18):2561-4. [ Links ]
Received: March 05, 2018; Accepted: April 26, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
