










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkDear Editor,
In relation to the article published in this journal by Alberto Herreros de Tejada et al. 1, we recently diagnosed a case of adenocarcinoma of the proximal anal canal with an exceptional immunohistochemistry. This was identified as an incidental finding after a hemorrhoidectomy in a patient with serrated polyposis syndrome (SPS).
Case report
We present the case of a 48-year-old female, current smoker, with a history of endoscopically controlled SPS. The patient was assessed for grade III hemorrhoids, and a hemorrhoidectomy in accordance with the Milligan-Morgan technique was performed. Pathological analysis of the specimen revealed a poorly differentiated infiltrating adenocarcinoma that originated from a tubular-villous adenoma with high-grade dysplasia at the squamocolumnar junction (Fig. 1A and B). The superficial adenomatous lesion and the infiltrating component were identical and expressed cytokeratin 7 intensely, and were negative for cytokeratin 20 (Fig. 1C). A multidisciplinary committee decided to widen the previous resection margins after a computed tomography (CT) scan confirmed the absence of distant or lymph node disease. No residual tumor infiltration was found in the surgical specimen. PET-CT after three months follow-up showed lymphadenopathy at the sigmoid colon mesenterium. Given these findings and the history of SPS, a proctocolectomy with end ileostomy was performed. Histopathological analysis identified multiple serrated adenomas with low-grade dysplasia with metastasis of poorly differentiated carcinoma that was morphologically the same as that observed in the anal canal in 2/109 lymph nodes analyzed (pT0N1bM0). The patient started adjuvant chemotherapy.
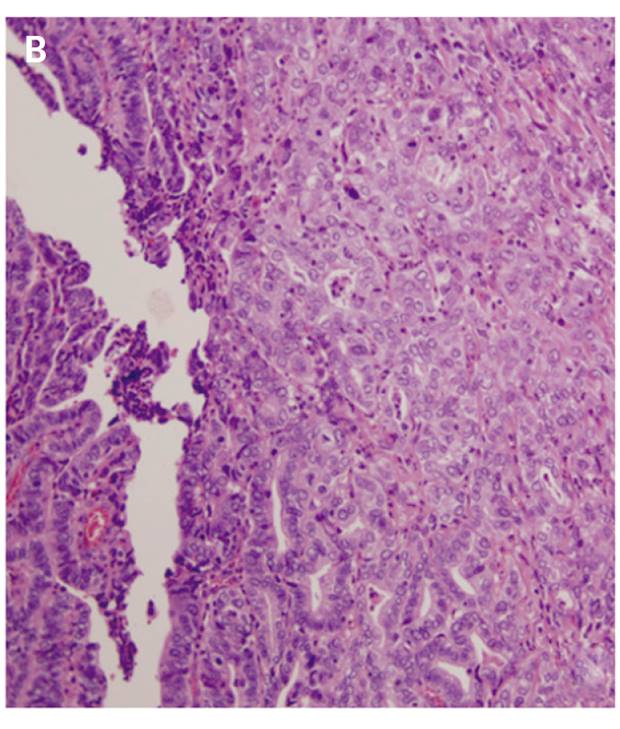
Fig. 1 A. Microscopic image of the epithelium in the squamocolumnar transition zone (arrow); the polyp mucosa is cranial to it (hematoxylin-eosin). B. Microscopic image of infiltrating tumor foci in the submucosa, with poorly differentiated and disorganized cells with nuclear pleomorphism (hematoxylin-eosin). C. Immunohistochemistry of the polyp at the hemorrhoid. Submucosal tumor clusters in the center and on the right (arrows), both reaching the limit of the resection plane, hindering a proper assessment of the deeper margin.
Discussion
Anal adenocarcinomas account for up to 10% of anorectal tumors 2. They are more commonly located proximal to the dentate line and are histologically and immunohistochemically similar to rectal carcinomas (CK7- and CK20+). The main clinical implication is regional lymphatic dissemination 3. Intense CK7 expression makes it necessary to rule out both ductal anal carcinoma and metastatic lesions. In rare cases with a high-grade and poorly differentiated colorectal phenotypes, expression of CK20 may be replaced by CK7 4. As a T1 lesion with no evidence of lymphatic or distant disease was identified via a CT scan, we opted for close surveillance following margin extension. With regard to SPS, factors associated with malignancy are serrated adenomas with dysplasia and their multiplicity 1.

