Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
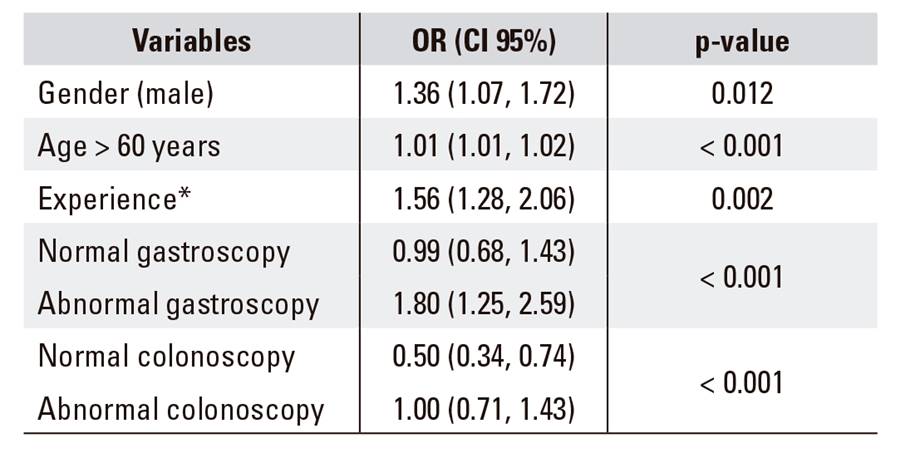
PermalinkDear Editor,
We read the papers by Juanmartiñena et al. entitled "Colonic lesions in patients undergoing small bowel capsule endoscopy: incidence, diagnostic and therapeutic impact" 1 and "Gastroduodenal lesions detected during small bowel capsule endoscopy: incidence, diagnostic and therapeutic impact" 2. Since its introduction into clinical practice in 2000, capsule endoscopy (CE) has become a first-line procedure for the investigation of small bowel (SB) diseases. In fact, more than two million capsule examinations have been performed worldwide to date 3. SBCE begins to capture images from the mouth and continues until the end of the battery life, which usually occurs after reaching the colon. Therefore, it may also allow the detection of lesions in other segments of the gastrointestinal tract and theoretically accessible to conventional endoscopy 4. Juanmartiñena et al. demonstrate that the incidence of gastroduodenal 2 and colonic lesions 1 detected during SBCE is 31% and 9%, respectively. In collaboration with the mentioned authors and following their line of research, we investigated factors that could predict the presence of non-small bowel lesions during SBCE. A statistically significant relationship was found via univariate analysis between non-small bowel lesions and the following variables: male, age > 60 years, NSAIDs, procedure indication, previous endoscopic examinations with findings, procedure timing (< 72 h) and reader experience. However, according to the multivariate analysis (Table 1), only the following variables were associated with an increased risk of presenting non-small bowel lesions: male gender (OR = 0.74), age > 60 years (OR = 1.01), non-experienced reader (OR = 1.56) and both previous gastroscopy (OR = 1.80) and ileo-colonoscopy (OR = 1) with findings. However, these results do not allow us to develop a reliable formula to predict the presence of non-small bowel lesions. Thus, according to that previously reported by Juanmartiñena et al. 1,2, the review of all SBCE images is still high recommended, even those located within the reach of conventional endoscopy.