










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Neuropathic pain can be caused by damage produced at any point in the nociceptive pathway, from the nociceptors to the cortical neurons of the brain1. Depending on the location of the damage, neuropathic pain can be classified as central or peripheral; according to its distribution as localized or diffuse; According to its etiology, it is classified as metabolic, secondary to ischemia, secondary to inflammation, paraneoplastic, neurodegenerative or traumatic2,3.
Painful Traumatic Trigeminal Neuropathy (PTTN) occurs in 3.3 % of patients with trigeminal nerve injury. In patients with fractures of the zygomatic-maxillary complex, anesthesia or hypoesthesia is frequently observed at examination of territory corresponding to the innervation of infraorbital nerve. However, the development of persistent neuropathic pain occurs only in 3.3 % of cases1,2.
Injury to a nerve delivers negative symptoms in an early stage such as anesthesia, hypoesthesia, or hypoalgesia. Later, it presents positive symptoms such as formication paresthesia, which corresponds to abnormal activity of Ab fibers, and pain. The latter can be spontaneous or provoked, which can be of a burning nature, which suggests discharges of type C nociceptors, or lancinating, which suggests ectopic discharges originating in the axon of the A delta fiber1,3.
PTTN, unlike essential trigeminal neuralgia, usually presents as a persistent pain although it may have paroxysmal attacks on a painful basis; it is normally of a burning nature, although it may also have a lancinating component, and reaches a moderate to severe intensity3. Patients usually complains of swelling, heat or cold, and erythema in the area that hurts4,5. It shares other characteristic of all neuropathic pain, such as having a strict distribution to the affected dermatome and presenting allodynia and/or hyperalgesia.
According to the International Headache Society there are the following diagnostic criteria for PTTN:
Unilateral facial and/or oral pain that meets criterion 3.
History of identifiable trauma to the trigeminal nerve, with positive and/or negative clinical signs, these evidences of trigeminal nerve dysfunction.
Causality is demonstrated by the following two criteria: a) The pain follows the same distribution of the affected trigeminal nerve branch. b) The pain occurs between the third and sixth month after the trauma.
Absence of explanation for another diagnosis6.
The management of neuropathic pain should be early and multimodal in nature, considering all therapeutic alternatives, both pharmacological and non-pharmacological7.
The management of PTTN generally follows the recommendations for peripheral neuropathic pain, where membrane stabilizers and tricyclic antidepressants are the main drugs8 (Table 1, Table 2, Table 3).
A small number of patients may have very little or no response to pharmacological treatment and neurosurgical procedures appear as an alternative to this group of patients. These include radiofrequency rhizotomy, stereotaxic radiosurgery, open section of trigeminal nerve roots, and deep cerebral or cortical electrostimulation, but reports have shown disparate results for different conditions of neuropathic and non-neuropathic pain of the face9.
Table I.
First-line drugs for the treatment of PTTN in the maxillofacial territory.
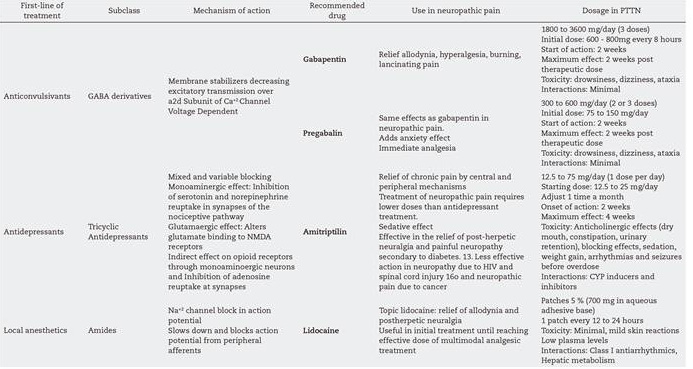
Table II.
Second-line drugs for the treatment of PTTN in the maxillofacial territory.

Tabla III.
Third-line drugs for the treatment of PTTN in the maxillofacial territory.

CASE REPORTS
First case of a 43-year-old female (Figure 1. A) patient with a left zygomatic fracture, for wich she underwent surgery for reduction and osteosynthesis. Nine months later, the patient consulted for pain assessed according to the visual-analog-scale (VAS) as 8 on the left side of the face, wich described it as lancinating in the skin of the left genial region and the left side of the upper lip. At the touch of the area she reported 10 in VAS, and hypoesthesia of the left suborbital skin, left side of the upper dentoalveolar region. The finding of mechanical allodynia manifested by touch of the innervation territory corresponding to the left infraorbital nerve was evident.

Figure 1. Case 1. A. 43-year-old female patient with a left maxillary-zygomatic fracture. B. Postoperative control CT-3D reconstruction.
The postoperative control image (Figure 1. B) showed a single osteosynthesis plate located in the zygomatomatoalveolar-buttres on the same side. Was diagnosed as a PTTN that affected the left suborbital nerve. With this, treatment with pregabalin was started with an initial dose of 75mg/day, after two weeks was has decrease in the severity of pain of 2 points in VAS was achieved, the dose was increased to 75 mg every 12 hours and carbamazepine 200mg per day was added to take as a single intake at the end of the day. After one month, the patient experienced pain relief that reached 50 % reduction in the value of VAS. Five months later a pain relief of 50 % was maintained but had isolated episodes of increased pain severity which maintained its characteristics. It was decided to add amitriptyline in doses of 12.5 mg per day. At the seventh month after the start of the therapy, the patient reported relief of the severity of the pain giving a 2 in VAS, which meant an improvement of 70 %.
The second clinical case corresponds to a 62-year-old male patient (Figure 2. A), who suffered an accident wich resulted in a left side maxillary-zygoma fracture. He underwent surgery in another maxillofacial-surgery service, and three months later he began with a persistent lancinating sub-eyelid pain on the same side as the fracture, which reached a 5 in VAS and reached 9 with touch of the area or with movements of facial mimic muscles. Also had anesthesia in the same area of the pain that was present since the accident. On examination, the patient had allodynia to the touch of the left sub-palpebral territory, left nasal wing, and anterior area on the left side of the maxilla.
The CT scan (Figure 2.B) showed an operated left side zygomatomaxillary fracture, with osteosynthesis installed in the left frontozygomatic suture, infraorbital rim, zygomatomaxillary buttres and a mesh that covered the left infraorbital hole.
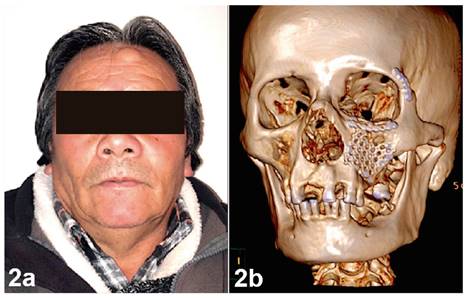
Figure 2. Case 2. A. 62-year-old male patient with a left side maxillary-zygomatic fracture. B. CT-3D reconstruction showing an operated left side zygomatomaxillary fracture.
Given the described disposition of the mesh, it made suspect a possible compression of the suborbital nerve, so it was decided to remove it. At the surgery, the compression exerted on the affected nerve was verified. The patient was treated with pregabalin at a dose of 75 mg every 12 hours and lidocaine patches to be used 1 every 24 hours in the affected territory. One month after starting this treatment, the patient evolved favorably, reporting a VAS assessment of 4. Considering it still compromised the quality of life of the patient, amitriptyline was added in a single daily dose of 25 mg/day, after which, evolving favorably after one month reporting complete pain relief, assessing it according to VAS as 0.
DISCUSSION
The low incidence of neuropathic pain in these cases has been explained because of the trigeminal nerve experiencing markedly lower ectopic discharges compared to other peripheral nerves10. As pathophysiological considerations for neuropathic pain in the cases described, we can explain its occurrence through the formation of a neuroma or areas of demyelination in the suborbital nerve, given the bone displacement caused by the fracture.
We could argue that the best treatment is the prevention of neuropathic sequelae after trauma. This means that the indication for surgery should be considered promptly after having suffered the accident in maxillofacial fractures that compromise any branch of the trigeminal nerve, which at first will manifest with a negative neurological clinical sign (anesthesia, hypoesthesia or hypoalgesia), although the bone displacement is less, trying to achieve an anatomical reduction. This give a favorable anatomical territory to allow or provide an opportunity for a repair of the affected nervous trunk to occur, thus avoiding areas of demyelination or the formation of a neuroma.
The treatment of this condition must be done with drugs of first line or in combination with others of second or third line, always considering the strategy of multimodal analgesia because of its effectiveness in pain control with lower incidence of side effects. The consequences in the quality of life of the patients who suffer PTTN can be devastating, given this, it's essential that the maxillofacial surgery teams be trained in the diagnosis and treatment of this type of condition, in order to achieve timely and effective treatment.

