










 Servicios personalizados
Servicios personalizados
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Multiple sclerosis is a chronic inflammatory demyelinating disease of the central nervous system that results in neuroaxonal degeneration in the long term1. Clinical presentation is variable as the disease may affect the pyrami dal, extrapyramidal, cerebellar and/or sensitive systems, and result in a neu rocognitive disorder in the long term2. It has a 3:1 predilection for women and a latitude-dependent prevalence: Colombia (1.48-4.89 per 100,000 inha bitants)3, United Kingdom (112 per 100,000 inhabitants), Canada (55-248 per 100,000 inhabitants), USA (65-160 per 100,000 inhabitants) and Spain (50 per 100,000 inhabitants)4.
The accumulating burden of disease results in physical and mental disa bility, which eventually makes patients dependent on caregivers and redu ces their productive lifespan5. Although little is known about what causes the disease, a plethora of different medications are currently available, each with its own mechanism of action and routes of administration6 7 8-9. Multiple sclerosis is considered a high-cost disease. The actual cost varies depen ding on the type of drug used, the complications associated with the given therapy, the relapse rate, and the accumulated disability. A study carried out between 2003 and 2008 in Colombia10, reported that 91.5% of the expenditure during the relapsing-remitting phase corresponded to the di rect cost of disease-modifying therapies (DMTs). Such direct costs, however, tend to go down when patients have moved to the secondary progressive phase. Nevertheless, it is during this phase that indirect costs (associated to disability and disability support) usually experience a significant increase, accounting for 39.1% of the overall expense. In 2008, the cost per patient in Colombia was up to USD 25,714 during the relapsing-remitting phase and up to USD 1,237 for each relapse. In 2014, Colombia spent approximately USD 42,952,209 on treatments for their multiple sclerosis population5.
There is a global trend toward evaluating the economic impact of different treatments in order to determine which should be reimbursed11. The purpose is to generate high-quality healthcare services within a context of limited eco nomic resources12 13-14. The purpose in this paper is to carry out a systematic review of the literature in order to analyze the information published through cost-effectiveness models. The ambition is that the conclusions drawn from this study might contribute to clinical decision-making, thus having a beneficial effect on the rational and appropriate use of public resources.
The main goal of this study was to identify and describe cost-effec tiveness studies that evaluated DMTs in the context of relapsing-remitting multiple sclerosis.
The secondary goal was to review the studies that evaluated first, se cond and third-line therapies.
Methods
A combination of controlled vocabulary (MeSH, Emtree, DeCS, inclu ding exploded terms) and free-text terms (considering spelling variants, synonyms, acronyms and truncation) with field labels (title and abstract), proximity operators (adj) and boolean operators (OR, AND) were used. The sensitivity of the search strategy was enhanced including keywords that were relevant to the types of studies to be considered. Searches were performed in: MEDLINE (through Ovid), Embase (through de Ovid), the Co chrane Library, LILACS, the Tufts Medical Center Cost-Effectiveness Analysis Registry and the National Health Service Economic Evaluation Database. Open Grey was used for "grey literature' searches.
The MeSH (Medical Subject Headings) terms used were: Relapsing-Remitting Multiple Sclerosis, Cost Effectiveness Analysis, Interferon beta-1a, Interferon beta-1 b, Glatiramer acetate, Teriflunomide, Fingolimod Hydro chloride, Dimethyl Fumarate, Natalizumab, Alemtuzumab and Rituximab. DeCS (Descriptores en Ciencias de la Salud) terms included were: Esclerosis Múltiple Recurrente-Remitente, Análisis de Costo-Efectividad, Interferón beta-1a, Interferón beta-1b, Acetato de glatiramero, Teriflunomida, Clorhidrato de fingolimod, Dimetilfumarato, Natalizumab, Alemtuzumab, Rituximab. The search was performed on 1 January 2018.
Original economic evaluation studies were selected if included cost-effecti veness and cost-utility models. An analysis was conducted of those where the endpoint measured was the incremental cost-effectiveness ratio (ICER), i.e. cost/ quality-adjusted life-years (QALY). Regardless of whether the model was purely theoretical or was based on clinical trials, the publications had to include infor mation about patient outcomes and the direct costs of the treatments administe red. Considering that costs typically vary over time, the search was limited to the period January 2010-December 2017 Publications could be written in English or in Spanish. The analyses had to be performed from the payer's perspective13. All kinds of DMTs approved by both the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for 2017 were taken into consideration (these drugs are also authorized for use in Colombia by the Instituto Nacional de Vigilancia de Medicamentos y Alimentos (INVIMA)). Although Rituximab has not been officially licensed, its use is authorized in specific cases taking into ac count the available scientific evidence15 16 17 18-19. Following Hauser et a/.20, drugs were divided into three lines of treatment for analysis and comparison purposes. Studies where the information on outcomes and/or costs was not made clear (such as congress abstracts) were not evaluated. Nor did we evaluate studies that focused only on the adverse effects of DMTs but not on their cost, or those that analyzed drugs approved by only one of the two regulatory agencies mentioned.
Data processing
Two of the authors conducted the literature search independently, scree ning papers by title and abstract. Separately, an analysis was conducted of the methodology, design, quality and bias risk of each of the manuscripts. In the event of discrepancy between the two authors, the assistance of a third evaluator (methodological advisor) was enlisted. Data extraction was also carried out independently, including direct costs (disease-associated costs, relapse costs, medication costs), QALYs, ICER values and methodological data (authors, year of publication, type of study, study sponsor, country/con text, model used, model cycles, origin of data, evaluated interventions, cu rrency and year, method used for effect evaluation, target population, time horizon, discount rate, sensitivity analysis, outcome as evaluated by the mo del, conclusion of the study). Given the risk that there may be some degree of heterogeneity across studies and that the results might prove impossible to group together, it was decided not to perform a meta-analysis21,22. The CCE-MG-EPPI-Centre Cost Converter virtual tool (v 1.5, updated 29 April 2016, http://eppi.ioe.ac.uk/costconversion/default.aspx) was used to convert the different amounts reported in different currencies to a common currency (the US dollar). All ICER values were recalculated in the light of the primary data provided by the model. The Microsoft Office 365 Excel software® (Micro soft Corporation) was used to store all the information obtained in templates structured at the time of designing the protocol.
The QHES instrument (Quality of Health Economic Studies) was selec ted to evaluate the quality of the studies23. The tool was developed spe cifically for cost-effectiveness analyses and provides a quantitative result that allows for more objective comparisons. It is a validated instrument made up of 16 items that provides a score between 0 and 100, where 100 represents the highest quality. Each author independently applied the instrument to each one of the articles included in the analysis. A de cision was made not to use the CHEERS (Consolidated Health Economic Evaluation Reporting Standards) tool24 as it is a qualitative instrument that does not prove useful in helping authors decide whether an article is high quality or not. The risk of bias of each study was evaluated by each author without any tool as there are no standardized instruments available for this purpose. The authors took into consideration the proposal by Evers et al.25. Discrepancies were analyzed in conjunction with a methodological advisor. Biases typical of a systematic review such as the study selection bias, the information bias and the publication bias were carefully considered. Mitigation of intrinsic biases was performed as follows:
Selection bias: each of two authors followed an independent search strategy; the results were compared and discrepancies were resolved with the help of the methodological advisor.
Information bias: each author independently evaluated the quality of each manuscript and carried out a bias search. Discordant results were discussed with the methodological advisor.
Publication bias: the "grey literature' search was performed with the aid of the Open Grey database.
Results
A total of 401 manuscripts were reviewed: 108 from MEDLINE, 161 from Embase, 55 from the Cochrane library, 0 from LILACS, 26 from the Tufts Medical Center Cost-Effectiveness Analysis Registry, 50 from the Na tional Health Service Economic Evaluation Database and 1 from Open Grey. After removing duplicate records, manuscripts published before Ja nuary 2010, those written in languages different from English and Spanish, those where the title and/or abstract had no bearing with the interventions to be analyzed, those who did not correspond to cost-effectiveness studies; and those that were congress abstracts, a total of 22 articles were left to be evaluated in their full form. After reviewing those full texts, 9 references were found to meet the inclusion criteria26 27 28 29 30 31 32 33-34 (Figure 1)35. A total of 13 studies were excluded as they were approached from a social perspective36 37 38 39 40 41-42; they did not calculate the ICER (cost/QALY) when evaluating costs43 44 45-46, or failing to clearly specify the total cost of each drug47,48.

Study characterization
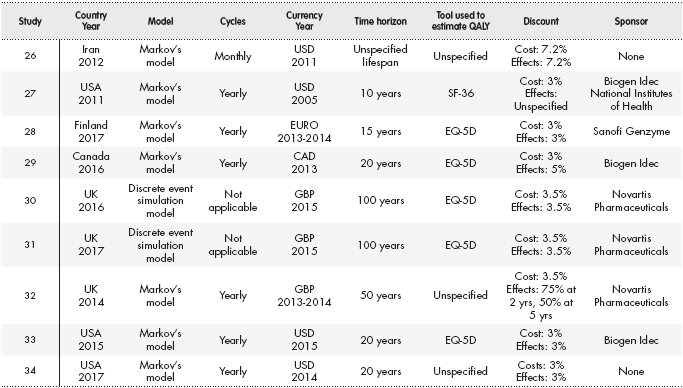
Of the nine studies included in the analysis, seven were conducted un der the sponsorship of a pharmaceutical company27 28 29 30 31 32-33. Seven studies were based on Markov's model26 27 28-29,32 33-34, and two on a simulation of discrete events30,31. Three studies analyzed first-line drugs26 27-28, two looked into se cond-line medications32,33, one study compared second-line with first-line medications29, two compared third-line medications with one second-line drug30,31, and another compared sequential interventions from the first to the third line34. There was significant variability in the currencies used: some studies used US dollars (USD), others euros (EUR) and others used pound sterling (GBP). As regards the effects measured, quality of life was determi ned using the EuroQol-5D instrument in over half the studies27 28 29 30-31,33, the others leaving the tool used to calculate QALYs unspecified. The time horizon was variable; in some cases it was between 10-15 years27,28 while in others it was 100 years30,31. Discount rates were very similar, mostly between 3% and 5%. The specific details of each study are shown in Table 1.
Bias
Pre-study phase: All nine studies reviewed present a narrow perspec tive bias as they were all conceived from the payer's point of view, as specified in the Methods section13. Four studies were found to contain an inappropriate comparison bias: three compared drugs with placebo26 27-28 and one study compared two drugs in the context of highly-active multiple sclerosis but no studies were cited that demonstrated the effectiveness of the control drug in that setting31. A cost omission bias was detected in three studies26,27,34 and an intermittent data collection bias was observed in two studies26,27.
Study phase: There were no cases with an invalid valuation bias. Nor were there ordinal ICER biases or double counting of costs. Inappropriate discount and limited sensitivity analysis biases were identified26,27.
Post-study phase: No biases were identified with respect to the disse mination and reporting of the analyses. Six studies contained a potential bias with respect to the study's sponsor and the cost-effectiveness results presented28 29 30 31 32-33: Three studies were sponsored by Novartis Pharmaceuti cals, manufacturer of fingolimod30 31-32, two studies were sponsored by Bio gen Idec, manufacturer of dimethyl fumarate and natalizumab29,33, and one study was sponsored by Sanofi Genzyme, manufacturer of teriflunomide28. A study sponsored by Biogen Idec showed no results in favor of interferon beta-1a27.
Quality of the studies included
Overall, studies obtained satisfactory quality scores (Table 2). None of them was in the low quality category and only one was rated as "class 2"26. The remaining eight publications were considered to be "class 4", the highest quality rating27 28 29 30 31 32 33-34 (Table 2). All the studies expounded their pur pose clearly, calculated costs appropriately and made a straightforward description of the methodology used. They also provided details of the economic model used and of the numerator and denominator components of the ICER. All of them justified their conclusions based on the results obtained and disclosed their funding sources. Most publications26,28 29 30-31,33,34 failed to discuss potential biases and their relationship with the results obtained.

Incremental cost-effectiveness ratio of the studies
As the protocols and the outcomes of each study were too heteroge neous to allow a statistical analysis of grouped data, the results are pre sented using a descriptive analysis approach (Table 3). The line of therapy evaluated in each study was clearly designated as a function of the drug used as a control for the pharmacoeconomic analysis; when the control drug was a placebo, the study was considered to be concerned with the line of therapy which the drugs evaluated belonged to. Three studies analy zed the first line of treatment26 27-28, five studies looked at the second line29 30 31 32-33, and one study focused on the third line34.
Table 3. Results of the studies evaluating the incremental cost-effectiveness ratio (cost/QALY)

ICER: Incremental cost-effectiveness ratio; QALY: quality-adjusted life-years.
*Direct costs converted to 2016 United States dollars.
**Threshold converted to 2016 United States dollars and expressed as cost/QALY (threshold published in the study).
First-line medications:
Three studies compared subcutaneous (SC) and intramuscular (IM) interferon beta-1a and interferon beta-1b26 27-28 with placebo. Two of those studies also evaluated glatiramer acetate27,28 while one study analyzed teriflunomide and dimethyl fumarate28. Imani et al.26, who chose their cost-effectiveness threshold in a random manner, reported that none of the DMTs analyzed stood below the willingness to pay (WTP) per QALY threshold. Noyes et al.27 and Soini et al.28 did not define a cost-effective ness threshold. In the first study, none of the therapies was cost-effective; while in the second interferon beta-1b was shown to be dominant over placebo, and teriflunomide proved to be dominant over glatiramer ace tate and interferons. Cost, QALY, threshold and ICER values are presen ted in Table 3.
Second-line medications:
Dimethyl fumarate was evaluated in three studies29,32,33; fingolimod in four studies30 31 32-33; glatiramer acetate in two studies29,33; and SC interferon beta-1 a, natalizumab and alemtuzumab in one study each29,30,32. The selected cost-effectiveness threshold stood between USD 20,000 and 50,000 in four articles29 30 31-32; one of the studies failed to establish a cost-effectiveness threshold33. According to Su et al.29 dimethyl fumarate was a cost-effective option as compared with glatiramer acetate and SC in terferon beta-1a; Mauskopf et al.33 showed this drug to be dominant over glatiramer acetate and fingolimod. According to Maruszczak et al.32, fingolimod was cost-effective in 73% of cases when compared with dimethyl fumarate. Montgomery eta.30 showed natalizumab to be more cost-effective than fingolimod, and the same author demonstrated ale mtuzumab to be dominant over fingolimod in another study31 (Table 3).
• Third-line medications:
Bin Sawad et al.34 compared IM interferon beta-1 a, natalizumab and alemtuzumab with symptomatic management, considering them sta ges along an increasing therapeutic potency medication journey. They established a cost-effectiveness threshold of USD 50,000-100,000. Although none of the DMTs turned out to be cost-effective with respect to that threshold, alemtuzumab did prove dominant over natalizumab, regardless of the WTP per QALY threshold (Table 3).
Discussion
The results of the present study show that placebo was cost-effective as compared with first-line medications26,27. Only one study, which compared the different drugs to one another, favored the use of teriflunomide over all the other therapies28. For the second line of treatment, dimethyl fumarate proved cost-effective29,33; fingolimod, alemtuzumab and natalizumab were also cost-effective, each in one separate study30 31-32. Also in the second line, two studies compared dimethyl fumarate with fingolimod, each obtaining different results as a function of the model applied. With respect to the third line, alemtuzumab was found to be dominant over natalizumab34.
Interpretation and application of these results need to be made with caution as ICER values exhibited a wide variability, even within one same treatment and using the same control medication. This variability is heavily dependent on 1) the parameters selected to develop the pharmacoecono mic model; 2) the choice of the control medication; and 3) the WTP per QALY threshold established. On the other hand, there are a few similarities such as the use of one same tool to calculate quality of life and discount rate values. First-line drugs were the most commonly analyzed probably because their cost tends to be lower than that of the most innovative therapies. Three publications26 27-28 used placebo, which is usually the least costly of all medications, as the control drug. Studies that evaluated the same drugs took their data from different sources, which may interfere with their comparability. Moreover, different models were used for the economic analysis (Markov's model, decision analysis model and discrete event simulation model). There were also differences in terms of the cu rrencies used in the different cases, the amounts of the costs, the models' time horizons and the outcomes evaluated. All of this poses a significant challenge for the current study in terms of extracting the data and selec ting the most relevant of those data making sure they are comparable, at least from a descriptive point of view. All the studies had biases inherent in the model used; there were cases of sponsorship bias, which required a rigorous analysis of both the model itself and the results obtained. The evaluation made using the QHES instrument revealed that the majority of studies were of the highest quality and sought to present information as clearly as possible.
In Colombia, the approval granted to the drugs used to treat relap sing-remitting multiple sclerosis does not preclude their use in the first-line setting, which makes it possible to offer each patient a customized treatment. Based on an understanding that monoclonal antibodies and fingolimod are the most costly of all the drugs in this category, the autho rities tend to promote a more rational use of financial resources by sepa rating therapies into different lines so as to gradually increase therapeutic potency according to the patients' requirements and each drug's safety profile. Taking into account this local therapeutic approach (unpublished information), a modification was made to the proposal by Hauser et a/.20 to execute the information analysis. First-line treatments were considered to include injectable therapies and teriflunomide given their lower effec tiveness and higher safety, and the existence of trials with patients with clinically isolated syndrome. The second line included dimethyl fumarate and fingolimod given their higher potency as compared to injectables, regardless of the higher safety profile theoretically associated with di methyl fumarate. The third line included monoclonal antibodies because of their higher effectiveness, higher risk of adverse effects and higher cost in the country. Regardless of the comparison that could be drawn based on the classification of the different medications, the heterogeneity of the models used inevitably poses a significant limitation on the comparison of the different ICER values.
Three previous systematic reviews looked into pharmaco-economic outcomes in the context of multiple sclerosis treatment49 50-51. Clegg et al. set about investigating the effectiveness of therapies used within the di fferent lines of treatment, including such non-disease-modifying drugs as methotrexate, cyclophosphamide and azathioprine49. They only found pharmaco-economic cost-effectiveness and cost-utility studies for interferon beta-1a, interferon beta-1b and glatiramer acetate, with significant variabi lities and highly heterogeneous outcomes that are difficult to interpret out of context. As regards the reviews by Yamamoto et al.50 and lannazzo et al.51, although findings are similar to those of the present study, the authors included studies with a social perspective, which further increased the he terogeneity of results and limited the strength of any conclusions drawn13. Additionally, in lannazzo et al.51, the method used to convert prices is not ideal. Although the present review specifies the difficulties inherent in working with heterogeneous information, it, at the same time, identifies a full range of therapeutic options as well as further studies with active con trol medications. The present study therefore seeks to analyze the whole range of DMTs authorized by the two most important regulatory agencies worldwide (EMA and FDA).
From the patient's point of view, the most interesting thing to determine would be each drug's potential to reduce disability, improve quality of life and extend the individual's productive lifespan. Accordingly, an effective pharmacoeconomic assessment should include outcome measures that are important for both the patient and the payer in the long term. Unfor tunately measuring these indirect costs is not easy given the scarcity of data and the vagueness of values and utilities. For this reason, a decision was made to limit the scope of the present paper in order to obtain results that would be comparable across different studies. The payer's perspective is usually narrower, with outcomes that tend to be of greater interest to the healthcare system, which reduces the social impact created by the conclusions obtained. One of the most significant limitations of the present study is the inability to determine the real economic and social impact of the different therapies given the large number of variables to be considered. Indeed, none of the studies reviewed achieved such a large scope, especially in Latin America where no cost-effectiveness evaluation was found for the local population Adapting and extrapola ting the information obtained to other countries' models and currencies is difficult and could even be inappropriate. This means that apart from the results that could be obtained, it is not feasible to generate a healthcare policy for a specific country without local data. Another limitation of this study is the selection bias resulting from having excluded studies written in languages different from Spanish and English. Only one (Russian lan guage) manuscript (repeated three times) was excluded from the analysis, but given the model used (mentioned in the abstract) it is unlikely that it would have affected the results. Restricting searches to the period bet ween 2010 and 2017 could also be construed as another limitation of the present paper, but taking into account that currencies tend to fluctuate significantly over time and that adjustments for inflation are not always correctly made, including older studies would have a strong impact of a cost-effectiveness model.
Further studies are required, designed on the basis of as homogeneous a set of models as possible (in terms of perspective, currency, time horizon, discount rate, target population, model cycles, interventions to be evalua ted, outcomes to be measured), which are free from sponsorship bias and which take into consideration the factors that have the greatest impact on patients' lives such as disability and productive life years.
The present study shows that, in spite of the effort to homogenize the high level of methodological variability of cost-effectiveness studies, it is not possible to determine which DMTs are the most cost-effective in the multiple sclerosis relapsing-remitting setting. Some of the studies in the literature even provide mutually contradictory results. Given the dearth of evidence available to answer the research question, further and more methodologically uniform studies are required to provide reasonable and effective cost-related recommendations to patients and to the healthcare system at large.

