










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
An estimated 250 million children under the age of five in low-and middle-income countries (LMICs) are at risk of failing to reach full developmental potential (Lu et al., 2016). According to the United Nations Children's Fund's (UNICEF) Early Childhood Development (ECD) Index, 36.8% of three and four-year-old children in LMICs do not achieve basic cognitive and social-emotional skills (McCoy et al., 2016). Multiple factors contribute to this developmental deficit: poor maternal health (including mental health), poor maternal nutrition, preterm birth, birth complications, poor infant nutrition, environmental health factors such as limited access to clean water, the amount of nurturing and stimulation in the household, and violence1 and harsh child-rearing practices (Grantham-McGregor et al., 2007). Early child developmental delays can be prevented by ensuring ideal health, social, and environmental conditions for mothers and other caregivers. For example, by assessing 1,307 healthy 2-year-old children of urban, well-nourished, educated mothers enrolled in early pregnancy in Brazil, India, Italy, Kenya, and the UK, Villar et al. (2019) demonstrated that children can achieve developmental milestones as long as pregnant women are healthy, educated, adequately nourished, and receive recommended antenatal care. A meta-analysis of 102 unique randomized control trials demonstrated that parenting interventions provide positive benefits in child cognitive development, language development, motor development, socioemotional development, and attachment, and reductions in behavior problems among children under three (Jeong et al., 2021). However, there are few ECD intervention studies that include a component to address parental attitudes and practices around violence against children, including corporal punishment. For example, in their meta-analysis, Jeong et al. (2021) reference just two studies of family violence prevention programs in East and Southeast Asia (Chen & Chan, 2015; McCoy et al., 2020), but these are not specific to children aged 0 to 3. We are aware of only one ECD intervention program in the Caribbean Region that has examined corporal punishment: the Jamaica-based Irie Homes and Classroom Toolboxes (Baker-Henningham et al., 2019; Francis & Baker-Henningham, 2020, 2021). This program has demonstrated effective violence reduction, emotional support of children by parents and teachers, decreased behavior difficulties among higher risk children, and early learning skills in children (i.e., oral language and self-regulation).
Given the sensitivity of young children's neurodevelopment, the potential negative impact that violence can have on ECD (Cuartas et al., 2021; Gershoff, 2002; Gershoff & Bitensky, 2008; Heilmann et al., 2021), and the high rates of corporal punishment in post-colonial countries, most of which are LMICs (Landon et al., 2017; Ocobock, 2012; Pate & Gould, 2012), this is an important area of investigation. Calling for new policies and programs to minimize violent discipline around the world, Cuartas et al. (2019) have estimated that 62 to 65 percent of 2- to 4-year-old children in LMICs are exposed to aggressive physical and psychological discipline. Cuartas et al. (2021) have also shown that corporal punishment, even if just ‘spanking,' alters neural responses in key areas of the brain needed for processing emotions and making decisions. In Latin America and the Caribbean (LAC) Region, where licks, slaps, and beatings are part of the cultural and religious landscape, an estimated 2 of every 3 children under age 5 are regularly exposed to violent discipline, and one in twenty is subjected to severe corporal punishment (UNICEF, 2018). Poverty and the presence of intimate partner violence against women exacerbate a young child's risk for poor ECD outcomes, and perpetuates intergenerational interpersonal violence. Across the region, 92 percent of children under age 5 possess at least one risk for poor ECD outcomes, with corporal punishment and emotional aggression being the most prevalent among risk factors (UNICEF, 2018). Protective factors include secure attachment of the child to a non-abusing adult family member, nurturing parenting skills, child social competence, and a supportive family environment with social networks and connections (UNICEF, 2018).
While many ECD interventions have been developed and implemented in LMICs, some continue to argue that ECD intervention and assessment remains neglected in resource-poor LMICs (Shawar & Shiffman, 2017; World Health Organization [WHO], 2018). The current challenge is to develop, implement, and assess LMIC caregiver intervention programs that account for the complexity of the ECD landscape in LMICs, including social norms around violence towards children (Chan et al., 2017). None of the 63 nations that have prohibited corporal punishment is a post-colonial LMIC (End Corporal Punishment, 2021). These social norms around violence and corporal punishment, which are more pervasive in post-colonial countries, may limit the beneficial effect of ECD interventions because of the impact that corporal punishment can have on neural development (Cuartas et al., 2021). Whether entrenched attitudes regarding the use of corporal punishment need to be addressed in tandem with evidence-based enrichment paradigms, such as nurturing care to improve ECD, remains an outstanding question in the field.
The World Health Organization (WHO), United Nations Children Fund (UNICEF), and World Bank Group (WBG) list five components of nurturing care, a framework for optimizing ECD by ensuring children's good health and nutrition, protection from threats, and opportunities for early learning. One of the five components is responsive caregiving, which includes “observing and responding to children's movements, sounds, and gestures and verbal requests” (WHO, UNICEF, WBG, 2018, p. 14). Within this framework, responsive caregiving interventions (1) encourage play and communication activities of the caregiver with the child, (2) promote caregiver sensitivity and responsiveness to children's cues, and (3) support caregivers' mental health (WHO, UNICEF, WBG, 2018, p. 19). The importance of responsive caregiving in forming the foundation for ECD is also consistent with findings from the Lancet series, Advancing Early Childhood Development: From Science to Scale (Britto et al., 2016). Another of the five components of nurturing care is safety and security – protection from physical dangers, emotional stress, and environmental risk. Together with good health, adequate nutrition, and access to early learning, safety, and responsive caregiving combine to maximize the potential for improved ECD outcomes.
Aboud and Yousafzai (2019) classify two types of interventions designed to improve ECD: (1) providing early learning opportunities and (2) promoting responsive caregiving. The first often consists of home visitation by a nurse, community health worker, social worker, or volunteer who engages directly in joint activities with children such as playing games, reading books, and/or allowing them to engage with and explore stimuli such as blocks and puzzles. After providing the stimuli and demonstrations, the visitor encourages the parent to take over the stimulation activities. The second also involves joint parent activities with children, but the key difference is in training the parent to provide a structured environment, recognize the child's cues (i.e., bids for attention) and abilities and respond appropriately. This requires the parent to have knowledge and skills to recognize and regulate her own emotional state, to foster a receptive emotional state in her child, and to be motivated to create a safe and attuned interpersonal environment for the two of them, which can then become the foundation for optimal or enhanced development. For example, parent repetition and extension of the child's actions and words, which are the foundation for the development of language (Black & Aboud, 2011), require motivation, attunement, and self-regulation, demonstrating the importance of the parent-child relationship and social-emotional connection for child development (Julian et al., 2017; MacMillan et al., 2009; Walker et al., 2011).
To heed the call for rigorous research into the delivery of responsive caregiving-based intervention programs and their outcomes (Chan et al., 2017), especially in children two years of age and under (WHO, 2018), we partnered with an existing U.S.-based organization called Conscious Discipline (CD) (Bailey, 2015). We also partnered with an existing community-based home visiting program in Grenada, West Indies, called the Roving Caregivers, who traditionally provided infant stimulation, with little focus on parent training. The purpose was twofold: (1) to change parent beliefs, attitudes, and behaviors around culturally-entrenched and harmful corporal punishment by (2) adapting and implementing a responsive caregiving program that helps caregivers recognize their own and their child's emotions, and builds parent and child self-regulation skills that create a strong social-emotional connection between parent and child. This connection forms the foundation of responsive caregiving and increases opportunities for early learning, maximizing ECD. The program's theory of change is predicated on building social-emotional connections between CD coaches and Roving Caregivers, who then build social-emotional connections between themselves and parents, who then build social-emotional connections between themselves and children, which in turn promotes neurodevelopment in the children.
The study was carried out in the small Eastern Caribbean LMIC island nation of Grenada (population: 113,570) to assess implementation before going to scale in larger, post-colonial LMICs. We hypothesized that: (1) parents exposed to the CD-based responsive caregiving intervention, which included positive, brain-based child-rearing alternatives to corporal punishment, would be less likely to endorse corporal punishment in their beliefs, attitudes, and behaviors compared to parents in the waitlist control group; and (2) children of parents exposed to the CD-based responsive caregiving intervention would show significantly higher neurodevelopmental outcomes at 24-months of age compared to children in a waitlist control group. Given the indirect nature of the intervention on child neurodevelopment, we expected small effect sizes (i.e., Cohen's d of 0.2 to 0.4). We also measured known variables (e.g., nutrition, preterm birth, parent socio-economic status) that can impact child neurodevelopment to allow for a more precise determination of the CD-based responsive caregiving intervention.
Method
Ethics
The study received ethical clearance from the St. George's University Institutional Review Board (IRB protocol #14066), which is registered with the US Department of Health and Human Services. Written consent was provided by all participants who agreed to be part of the study.
The study protocol is registered with ClinicalTrials.gov #NCT04697134 (https://clinicaltrials.gov/ct2/show/NCT04697134).
Study Design
A parallel single-blind, waitlist-controlled trial, post-only design was used in which children and their parents were enrolled in an existing community-based home visiting program called Roving Caregivers. Families were assigned to a CD intervention group versus a waitlist control group. The assignment was not randomized, but instead followed the process of parent-child recruitment carried out by the existing Roving Caregiver program. The study was implemented in Grenada, West Indies, via a partnership between St. George's University and the Roving Caregivers. Grenada is divided into six parishes on the main island, and a separate parish consisting of two smaller islands (Carriacou and Petite Martinique). Grenada is classified as an lower-middle income country by the World Bank, with an annual gross national income per capita of USD 9,840 in 2019. The population is majority Afro-Caribbean (82.4%).
Participants
According to data obtained from the Grenada Births and Deaths Registry, there were 5,278 children aged 0-2 in Grenada at the time of the study initiation. This represented the total population of children available for inclusion in the study. Children over the age of two at the time of recruitment were excluded from the study. In Grenada, the Roving Caregivers canvas villages and communities in all parishes each fall, targeting and recruiting families with children under age two, until the maximum number of families the program can service at any given time, determined by the number of current Roving Caregivers, is reached (the target ratio is 10-11 families for each Roving Caregiver). Thus, inclusion criteria were determined by the recruitment of families by the Roving Caregivers.
The total number of parents and children under age 2 enrolled in this study was 1,043, which represented 19.8% of all children under age 2 in Grenada at that time. A total of n = 752 parents and their children were recruited by the Roving Caregiver program and served by n = 70 Roving Caregivers who had undergone intensive training in CD as well as infant stimulation. These families and their children served as the CD intervention group and represented 14.2% of the total population of 0-2-year-olds in Grenada at that time.
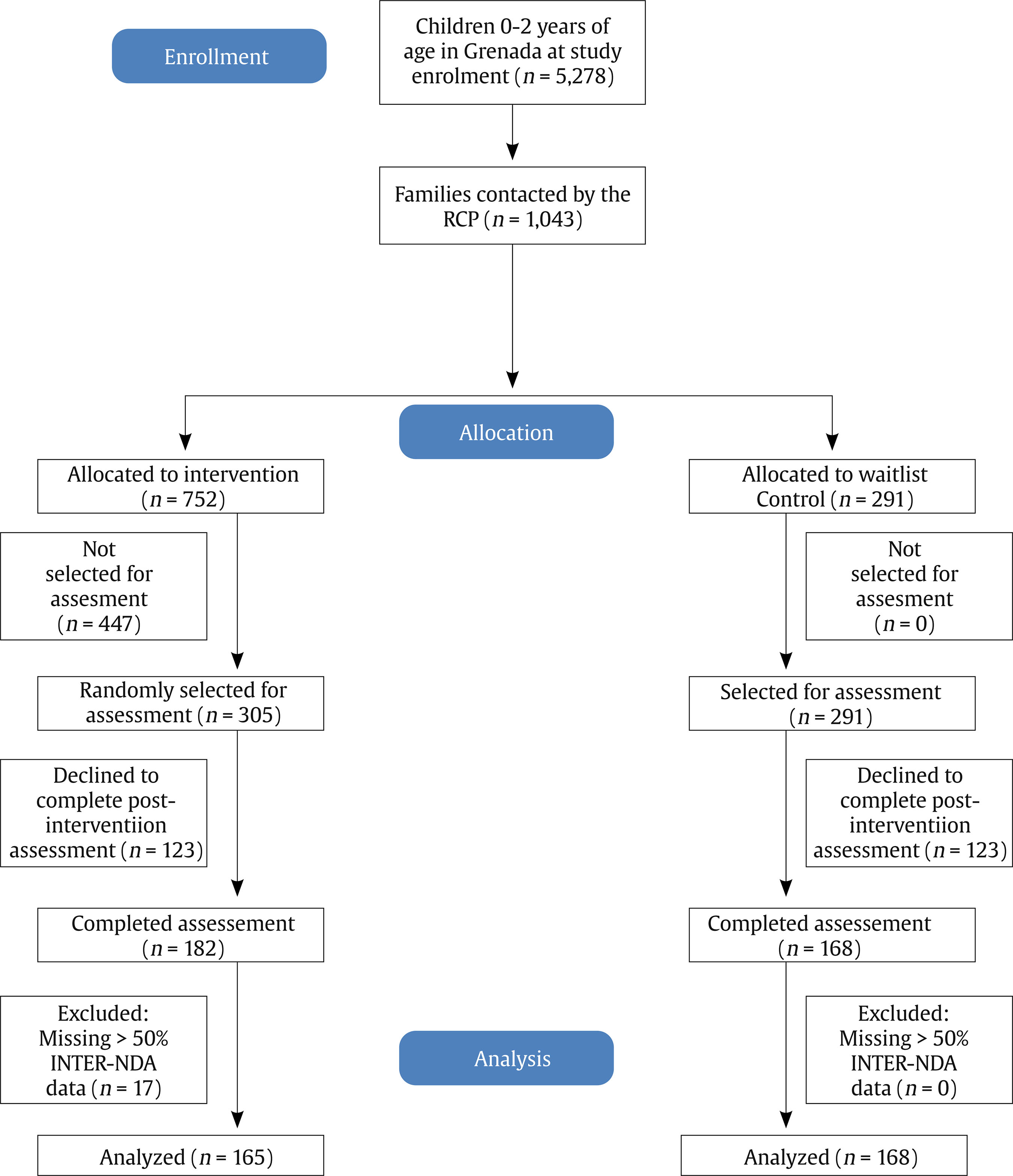
Of the n = 752 families in the CD intervention group, n = 305 (40.6%) were selected via random numbers table to complete a post-intervention assessment. Once the Roving Caregivers reached the maximum enrolment limit of families in the CD intervention group, they continued to recruit families with children under age two into the waitlist control group. The same recruitment procedures used for the intervention group were followed for the waitlist control group, but the parent was informed that the intervention would be delayed until the following year, and that her child would also be exposed to the intervention once s/he was enrolled in pre-primary school (as per a follow-up intervention program now underway by the Saving Brains Grenada team). A total of n = 291 parents and their children were recruited into the waitlist control group.
All n = 291 families in the waitlist control group were selected to complete the post-intervention assessment. Assessment data was collected from n = 182 (59.7% of selected families) in the CD intervention group and n = 168 (57.7% of selected families) in the waitlist control group. The other families in both groups declined to complete the assessment. A frequency analysis was run to identify participants with missing data and unusual responses on the dependent variable (i.e., INTER-NDA). Participants with more than 50% of responses missing from the INTER-NDA were removed from the data set (n = 17). A total of 333 participants (intervention: n = 165, waitlist control: n = 168) remained after the data was cleaned (Figure 1). We compared participants who dropped out of the study to participants who remained in the study to ensure no bias existed in the final post-intervention group comparison.
Procedure
A partnership was formed with the Roving Caregivers to implement a responsive caregiving based social-emotional skills program that builds connections between parent and child through eye contact, touch, presence by the parent to the moment, and a sense of play (Bailey, 2015). Three CD Certified Instructors (CDCIs), along with the curriculum's author and co-author of this report (BB) worked closely with the Roving Caregivers to adapt material and language for a Caribbean context, while fostering positive relationships between and among them. CDCIs undergo lengthy multi-year trainings, using videotapes and participant evaluation data, and are vetted by BB and a small team of Master Instructors. One of the CDCIs, an expert in the application of CD to toddlers, came to Grenada with BB to provide a week-long training for Roving Caregivers following their participation in an eight-week course taught by the two CDCIs in Grenada: one is a psychologist and the other a teacher, both of whom were teaching CD in the region for several years prior to the study. The Roving Caregivers, who provided the home visitation, are female secondary school graduates, some of whom have attended community college. At the time of the intervention there were 70 Roving Caregivers, 4 district supervisors, and the program's parent liaison, who is a retired nurse. In the field, Roving Caregiver supervisors and the parent liaison monitored teams for fidelity. The project manager, who is one of the CDCIs, made periodic home visits with supervisors and focused on building social-emotional connections with Roving Caregivers and their supervisors as well as fidelity to the CD intervention. Fidelity was assessed using a CD skills rubric adapted for the program; the fidelity instrument is included in the CD Responsive Caregiving Manual, available from the corresponding author.
Using a simplified triune brain model (MacLean, 1985) to describe child and adult brain states, and attending to safety and connection between themselves and the families they served, Roving Caregivers taught seven CD responsive caregiving skills to parents: (1) Composure (self-regulation) with which the parent reflects and responds to her child rather than reacting instinctively with overlearned corporal punishment behaviors; (2) Assertiveness (clear communication that is neither aggressive nor passive) by which conflicts can be resolved without violence; (3) Encouragement (noticing, acknowledging) with which positive behaviors such as team effort, belonging, and being of service to others are reinforced; (4) Choices (decision-making) with which adults respond to misbehavior by offering two positive choices, thereby preventing power struggles and fostering self-efficacy and decision making abilities in children; (5) Empathy (acceptance) by which adults understand a child's perspective and respond empathically but assertively, thereby integrating emotion and cognition; (6) Positive Intent (love) by which adults view misbehavior as a call for help or as a skill deficit, and respond accordingly by providing help or teaching a skill; and (7) Consequences (learning) with which adults use responsive, responsible strategies to provide logical, nonviolent consequences that promote learning and sociomoral development (Bailey, 2015). The program's theory of change is predicated on building social-emotional connections as a key foundation of child neurodevelopment.
A total of 70 Roving Caregivers visited homes in teams of two on a minimum weekly basis to meet with parents and their children to implement the curriculum. Each session was scaffolded on knowledge and skills imparted in previous sessions and followed a protocol as outlined in the CD-based Responsive Caregiving Manual, which is available from the corresponding author. The intervention included activities such as ‘Stop and Go,' ‘I Love You Rituals,' visual schedules and greetings, and reading Sophie books to impart the seven CD ‘brain smart' skills. Prior to rolling out the intervention in the field, each of the Roving Caregivers received 40 hours of in-person training in CD-based Responsive Caregiving and met pre-established criteria for knowledge and fidelity. They were reassessed every three months and ‘top-up' trainings were provided monthly. The intervention lasted up to 24 months. The number of intervention sessions varied by family depending on how many sessions the family attended and when the child turned 24 months of age, at which point neurodevelopmental assessment was carried out by a team of trained assessors. The total number of intervention sessions ranged from 1 to 52, with a median of 11. Given the community-based, voluntary nature of the intervention, parents could choose to withdraw at any time. Once children in both the CD intervention and waitlist control groups turned 24 months of age, they completed a neurodevelopmental assessment, allowing for a direct comparison between the groups.
Given entrenched and oftentimes emotional attitudes towards corporal punishment in the Caribbean region (Bailey et al., 2014), and based on the resistance we encountered during community engagement and child advocacy work for several years prior to the study, the researchers decided to refrain from speaking or writing about corporal punishment and other violence towards children in communications about the program, instead following the CD principle to “focus on what you want more of” (i.e., responsive caregiving and strong social-emotional connections). Although the relationship between alternative, responsive caregiving discipline practices and a reduction of violence directed towards children was implied and expected, we believe that families were more receptive to knowledge and skills when cultural norms were not directly challenged.
Primary Outcome - Neurodevelopmental Measure
The INTERGROWTH-21st Neurodevelopment Assessment (INTER-NDA) (Fernandes et al., 2014; Murray et al., 2018) is a multi-dimensional, standardized assessment tool measuring cognition, motor, language, and behavior outcomes in children aged 22 to 30 months. It was developed for and has been implemented in low-middle, and high-income populations (Fernandes et al., 2014). It was used as the dependent variable in the present study. Its 37 items are scored on a 5-point scale, characterizing the child's performance across a spectrum. It utilizes a mixed methodology psychometric approach consisting of directly administered tasks, concurrent observation of the child's skills, and caregiver recall, which offers several advantages over each approach used alone in the characterization of a child's neurodevelopment skills. Despite its fewer items, shorter administration time, and administration by non-specialists rather than specialists, it has shown good agreement with the Bayley Scales of Infant Development, 3rd edition (BSID III) (Bayley, 2006) (intraclass correlation coefficients between .745 and .883, p < .001, for all subscales) (Murray et al., 2018) and substantial inter-rater (k = 50.70, 95% CI [0.47, 0.88]) and test-retest reliability (k = 50.79, 95% CI [0.48, 0.96]) (Villar et al., 2019). It is administered and scored in 15 minutes and is amenable to administration in the field by trained non-specialists (Villar et al., 2019). Its norms are international standards of child development, constructed according to the WHO Multicenter Growth Reference Study's prescriptive approach, rather than descriptive population-specific references (Fernandes et al., 2020). Neurodevelopment assessors were drawn from various disciplines but all had a minimum bachelor's degree in a related field. The assessors received one-week of intensive training in the administration of the INTER-NDA by the measure developer and co-author (MF). More information about the assessor training and adaptation of the INTER-NDA for this study is available elsewhere (Waechter et al., 2022).
Secondary Outcomes – Maternal Mental Health, Home Environment, and Corporal Punishment Measures
Anticipated indirect effects of the CD intervention include improved maternal self-regulation and home environments, enhanced psychosocial stimulation, and a change in attitudes and behaviors towards corporal punishment. The following measures were included to determine the effect of the intervention on caregivers and their home environments: (1) General Health Questionnaire (GHQ-12) and (2) the Home Observation for Measurement of the Environment (HOME) questionnaire, the Confusion, Hubbub, and Order Scale (CHAOS). Questions were also included to assess differences in beliefs, attitudes, and behaviors around corporal punishment between the CD intervention and waitlist control groups (see Appendix).
Sociodemographic Covariate Measures
To assess the impact of the CD intervention on child neurodevelopment, and to determine the equivalence of the CD intervention and waitlist control groups at study initiation, parent surveys collected demographics, socioeconomic status, and information on the child and his/her home environment. The following measures were included in the study to assess and control for potential covariates of the relationship between the intervention program and child neurodevelopment: (1) demographics questionnaire; (2) infant birthing questionnaire; and (3) the USDA Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access.
Statistical Analysis
Maximum sample size was limited to the number of families recruited by the Roving Caregivers. Due to budgetary constraints, it was not possible to run assessments on all 1,043 families enrolled in the study. However, a post-implementation power analysis with the achieved sample sizes that received the neurodevelopmental assessment at 24 months of age (n = 153 CD intervention and n = 151 waitlist control) confirmed that enough participants were recruited and assessed to detect a significant difference between the groups (power = .963) (Figure 1).
All data were entered and checked for errors in entry, missing values, and outliers using Excel software (Microsoft Corp). We compared participants who dropped out of the study to participants who remained in the study to ensure no bias existed in the final post-intervention group comparison. CD intervention and waitlist control groups were compared across sociodemographic variables to ensure equality between the groups on these potential confounders. INTER-NDA mean scores were calculated for cognition (13 items), fine motor (4 items), gross motor (3 items), language (12 items), and behavior domains (3 positive behavior items and 2 negative behavior items) using the procedure described by Fernandes et al. (2020). Mean scores were converted to standardized scores and compared to international INTERGROWTH-21st Project (INTER-NDA) standards to determine age-based performance (Fernandes et al., 2020). Differences in domain scores were then compared between intervention and waitlist control groups using mixed models. All data were analyzed using the Statistical Package for the Social Sciences (SPSS) v. 25 (IBM Corp).
Results
First, participants in both the CD intervention and waitlist control groups who dropped out of the study (n = 246) were compared to participants who remained in the study (n = 350) to ensure no bias existed in the final post-intervention group comparison. The only variable that differed between those who dropped out and those who remained in direction of potential bias was partner education, in that waitlist control group participants who remained in the study showed a lower level of education (60% primary, 32%% secondary, 8% tertiary) than participants who left (41% primary, 54% secondary, 5% tertiary), χ2(2) = 6.04, p = .049. Thus, we included partner education level as a covariate in the main outcome analysis of INTER-NDA scores in the CD intervention group versus the waitlist control group. Partner education level did not significantly impact any of the INTER-NDA outcome scores in the children when included as a covariate, as reported below.
The CD intervention and waitlist control groups were then compared across demographics and potential confounding variables to ensure baseline equivalence between them using chi-square and two-tailed, independent samples t-tests. Children in the CD intervention group were significantly older than children in the waitlist control group by five weeks, t(331) = -3.52, p < .001, while the gender ratio was equivalent between the groups (Table 1). Given this difference, age was included as a covariate in comparisons of INTER-NDA domain scores between the CD intervention and waitlist control groups.

Parents of children in the CD intervention and waitlist control groups were compared across sociodemographic variables using chi-square tests. Parents in the waitlist control group were more likely to have attained a higher level of education, χ2(2) = 6.26, p = .044, and earn higher incomes χ2(3) = 20.20, p < .001, versus parents in the CD intervention group (Table 1). Given these differences, education level and income were included as covariates in comparisons of INTER-NDA domain scores between the CD intervention and waitlist control groups. Maternal questionnaire responses were compared across the CD intervention and waitlist control groups using chi-square and two-tailed, independent samples t-tests. No significant differences were detected between the groups in gestation (early, term, late), substance use during pregnancy, domestic violence, mode of delivery, complications during birth or infant problems after birth, breastfeeding, and food security in the home. The CD intervention and waitlist control groups were equivalent across these potential confounding variables.
The first hypothesis was that parents exposed to the CD intervention would be less likely to endorse corporal punishment in their beliefs, attitudes, and behaviors compared to parents in the waitlist control group. The results did not support this hypothesis: there were no significant differences in corporal punishment beliefs, attitudes, and behaviors, between the CD intervention group and the waitlist control group. A composite score of eight items in the attitudes to corporal punishment scale (Appendix) also showed no significant differences in attitudes between the CD intervention and waitlist control groups, t(315) = -1.052, p = .293 (Table 2). In fact, high rates of corporal punishment endorsement were reported across both the CD intervention group and the waitlist control groups; 59-67% of parents believed that corporal punishment should be used to discipline students in school; 72-75% of parents believed that corporal punishment helps build respect for authority figures; 71% of parents believed that corporal punishment helps children become successful adults; 91-95% of parents reported smacking/beating their child; 75-76% reported smacking/beating their child in the last week of that question being asked (Table 2). Note that the children being referred to in these last two questions are around two years of age.
Table 2. Parent Beliefs, Attitudes, and Behaviors Toward Corporal Punishment for Intervention and Control Groups (Appendix)

The second hypothesis was that children of caregivers exposed to the CD intervention would show significantly higher neurodevelopmental outcomes at 24-months of age compared to children in a waitlist control group. A mixed model analysis was used to determine the difference between the groups across the INTER-NDA domain scores after controlling for ECD assessor, and parent address (i.e., the parish where the child lived). ECD assessor had a significant impact on the INTER-NDA scores (p < .001), parent address did not have a significant impact on the INTER-NDA scores (p = .086). There were no changes in significance (i.e., > or < p = .05) on INTER-NDA domain scores between the CD intervention and waitlist control groups when the assessor covariate was not included in the analysis versus when the assessor covariate was included in the analysis, so only results are reported for when the assessor was included in the model. Address is not included given its non-significant impact on INTER-NDA scores.
Results of the mixed model analysis showed that children whose caregiver(s) received the CD intervention scored significantly higher across the INTER-NDA domains of cognition, fine motor, gross motor, and language compared to children who were allocated to the waitlist control group (Table 3). The effect sizes for the CD intervention group ranged from small (.216 for cognition) to medium (.524 for fine motor). Children whose parents completed higher levels of education scored significantly higher across the INTER-NDA domain scores of cognition and language compared to children whose parents completed lower levels of education. The effect sizes for the group with higher levels of education were small (i.e., .228 for cognition, and .230 for language). Finally, as expected, older children scored significantly higher across all the INTER-NDA domain scores than younger children, with very small effect sizes ranging from .008 (gross motor and negative behavior) to .023 (cognition). The CD intervention accounted for the greatest proportion of variability in explaining performance on the INTER-NDA of all the variables included in the model, except in the cognition domain. Specifically, the CD intervention accounted for .524 (medium effect) of the performance in the fine motor domain compared to .011 for child age; .238 (small effect) of the performance in the gross motor domain compared to .008 for child age; .259 (small effect) of the performance in the language domain compared to .015 for child age and .230 for parent education level. In the cognition domain, the intervention accounted for a slightly lower .216 (small effect) of the performance compared to .023 for child age and .228 for parent education level. Parent monthly income did not significantly contribute to outcomes on any of the INTER-NDA domain scores.
Once the impact of the CD intervention on INTER-NDA scores was confirmed, the raw mean scores were converted to standardized scores using the procedure described by Fernandes et al. (2020). Standardized scores between the CD intervention group and the waitlist control group were compared using a general linear model (GLM). The following covariates were included in the analysis: infant age (at testing), parent monthly income, and parent and partner education level. The total sample size across groups decreased from n = 333 to n = 304 due to missing data for some of the covariates. Results of the GLM confirmed that the CD intervention group scored higher than the waitlist control group across all INTER-NDA domains except positive and negative behavior (Table 3), mirroring the results of the mixed model analysis after adjusting the model for the assessor covariate as reported above.
A t-test analysis examined the differences between the intervention and waitlist control groups on the secondary outcomes: maternal general health (GHQ), household chaos (CHAOS), and the home environment (HOME). Results of this analysis indicated no significant differences between the groups on the GHQ (p = .325), CHAOS (p = .428), and HOME (p = .759) measures.

Discussion
Children whose caregivers received the CD intervention training scored higher on measures of cognition, fine and gross motor skills, and language compared to children whose parents were assigned to a waitlist control group. These results held when the potential impact of different neuropsychological assessors was factored into the model. The effect sizes of the CD intervention on child neurodevelopmental outcomes were small-to-medium as hypothesized (i.e., cognition: d = 0.216 to fine motor: d = 0.524). This was expected given the complexity of the ECD landscape and the indirect impact of the CD intervention on child neurodevelopment, as outlined in the theory of change. These results are consistent with previous studies that examined the neurodevelopmental impact of ECD intervention programs (e.g., Aboud et al., 2013; Cooper et al., 2009; Gardner et al., 2003; Gianní et al., 2006; Kagitcibasi et al., 2001; Singla et al., 2015).
After controlling for significant factors such as infant age, parent, and partner education level, and parent monthly income, the CD intervention contributed more variance to fine motor, gross motor, and language development and just slightly less variance to cognitive development than parent education level. This is not surprising given the known relationship between parent education level and IQ and cognitive development in young children (Rindermann & Ceci, 2018; Roberts, et al., 1999). Interestingly, parent monthly income did not significantly contribute variance to any of the neurodevelopmental subscales examined in the current study. This, combined with the variance contributed by the CD intervention versus parent education level, suggests that the CD intervention can enhance ECD outcomes among families with low levels of formal education, and in a reduced timeframe of implementation and cost. By partnering with an existing community-based ECD program, the estimated cost of our intervention was relatively low, at USD 102.10 per child.
No differences in parent mental health, as measured by the GHQ-12, were detected between the CD intervention or waitlist control groups. This was unexpected given that the GHQ has demonstrated validity in detecting postnatal depression, anxiety, and adjustment disorders (Navarro et al., 2007). Thus, it is likely that the current intervention did not impact maternal mental health, or that not enough time passed between the CD intervention and the post-intervention assessment to detect changes in maternal mental health. There were also no differences detected between the CD intervention and waitlist control groups on the CHAOS or HOME environment measures. No differences in beliefs, attitudes, or behaviors towards corporal punishment were detected between the CD intervention and waitlist control groups. This was an unexpected finding, as it was hypothesized that, at a minimum, these beliefs would be moderated among those parents who received training in the importance of a strong social-emotional connection for optimal brain development, and concrete skills for building that connection. This methodology was followed given evidence that violence and corporal punishment may continue to occur when parents feel that there is no alternative (UNICEF, 2018). While the intervention did not include an explicit discussion of the impact of violence, including corporal punishment, on children's brains given its entrenchment within the culture (Bailey et al., 2014), it was expected that corporal punishment would diminish as alternative child-rearing practices increased. No evidence of this was detected in the current study. Considering the improvement in cognition, fine and gross motor skills, and language measured in the current CD Intervention, it is possible that entrenched attitudes regarding the use of corporal punishment do not need to be addressed in tandem with evidence-based enrichment paradigms such as nurturing care to improve ECD. While this is an interesting possibility, other factors must be considered. Perhaps if the current intervention had explicitly addressed the violence issue by telling parents about the potential negative impact of corporal punishment on children's brain development and told them they should not use corporal punishment while also providing alternative skills, differences in beliefs, attitudes, and/or behaviors regarding corporal punishment would have been seen between the CD intervention versus waitlist control groups.
Likewise, perhaps if the intervention had more specifically addressed parent mental health or home environments, differences would have been detected between the groups; however, these variables were not the direct focus of this intervention (although they raise interesting possibilities for future research). It may also be the case that not enough time passed between the provision of the CD intervention and our post-intervention assessment of beliefs, attitudes, and behavior regarding corporal punishment. Perhaps more time needs to elapse before parents demonstrate these changes. This is an interesting possibility that requires further exploration. Finally, whether differences in neurodevelopment between the waitlist control group and the CD intervention group would have been greater with a concomitant reduction in corporal punishment beliefs, attitudes, and/or behaviors in parents, or whether neurodevelopment can be optimized regardless of changes in corporal punishment remains an open question. Based on previous work that outlines the negative impact of violence and corporal punishment on child brain development (Cuartas et al., 2021; Gershoff, 2002; Gershoff & Bitensky, 2008; Heilmann et al., 2021), it is likely that reducing corporal punishment in conjunction with evidence-based responsive caregiving programs will result in greater ECD outcomes, and this is consistent with the nurturing care paradigm.
There are several limitations to the present study that must be considered. The families and their children in the intervention group represented 14.2% of the total population of 0-2-year-olds in Grenada at the time of study enrolment, which is a relatively small percentage. Recruitment was carried out in cohorts in which the first batch of families received the intervention, and the second batch were wait-listed rather than individual families being randomized to intervention and control groups. It was not possible to collect baseline child development data prior to the intervention, which would have allowed for an assessment of neurodevelopmental equivalence between the CD intervention and waitlist control groups going into the study and a pre-post analysis of changes in child development. Not all potential confounding variables were measured nor included in the study design, making it impossible to rule out unknown variables on child development outcomes. Given the recruitment process via a partnership with an existing community-based program, there was high variability in the number of contact points between parents and the Roving Caregivers as determined by the availability of the parents when the Roving Caregivers visited their community. This resulted in families receiving anywhere from 1 to 52 visits, with a median of 11. The study did not investigate the impact of individual CD interventionists (Roving Caregiver teams), which is a potentially important variable given the program's relational focus. Despite this, systematic developmental differences between children allocated to the CD intervention group versus the waitlist control group are unlikely, as both groups were recruited via the same procedures and by the same community program and there were very few significant differences in measured sociodemographic and confounding variables between the groups. The CD intervention contributed significant variance to child developmental outcomes after controlling for these significant differences.
The current study demonstrates the importance of responsive caregiving in forming the foundation of ECD in the critical first 1,000 days of life, in the absence of changes in beliefs, attitudes, and behaviors towards corporal punishment. This study addresses the need for knowledge about the feasibility and process of adapting/designing, implementing, and assessing a community-based ECD intervention for a normative population in the Caribbean region (Chan et al., 2017; Lu et al., 2016; McCoy et al., 2016; Shawar & Shiffman, 2017; WHO, 2018) while accounting for beliefs, attitudes, and behaviors around corporal punishment. The CD intervention had a significant positive impact on child neurodevelopment by focusing on three components of nurturing care (i.e., safety, connection, and learning) through a hierarchical brain model of neurodevelopment consistent with the responsive parenting approach (Aboud & Yousafzai, 2019; WHO, 2018). Whether a concomitant change in maternal mental health, home environment, and/or corporal punishment would result in a greater impact on child neurodevelopmental outcomes remains an outstanding question.


