










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.3 may./jun. 2006
Palatine perforation induced by cocaine
Perforación en bóveda palatina por consumo de cocaína
Miguel Padilla Rosas 1, 2, 3, Cecilia Irene Jimenez Santos 2, 4, 5, Claudia Lorena García González 1, 3
(1) Doctorado en Genética Humana
(2) Escuela de Odontología, Centro Universitario de Ciencias
de la Salud-Universidad de Guadalajara
(3) Medicina Molecular, Centro Medico Nacional de Occidente,
Instituto Mexicano del Seguro Social
(4) Cirugia Maxilofacial Hospital General de Occidente,
Secretaria Salud Jalisco
(5) Cirugía Maxilofacial Centro Medico Nacional de Occidente,
Instituto Mexicano del Seguro Social. Guadalajara, Jalisco
ABSTRACT
Worldwide, the use of cocaine has an increased over the years, various secondary effects have been described. Here we present a 48 years old female with a 2-month evolution bucconasal ulcer in the hard palate induced by cocaine usage accompanied by swallow and phonation dysfunctions. Ethiopathogenesis, differential diagnoses and treatment are discussed.
Key words: Palatine perforation, recreational drug use, cocaine,palatine lesions.
RESUMEN
El consumo de cocaína va en aumento en la población mundial, los efectos del consumo de esta droga pueden ocasionar efectos secundarios. Se presenta un caso de paciente femenino de 48 años de edad que presenta una úlcera crónica buco-nasal de 2 meses de evolución, la cual le ocasiona problemas para la deglución y fonación.
Palabras clave: Perforación palatina, consumo de cocaína, uso de drogas, cocaína, destrucción palatina.
Introduction
Cocaine usage has a growing incidence worldwide. The most common route of administration is nasal that induces local vasoconstriction and irritation on the exposed tissue due to the effect of both the active substance and others added during its manufacture (1-2). The highest risk group are individuals between 18 to 30 years old regardless of gender, socioeconomic status or occupation (2-3).One of the described local complications is ischemic necrosis in the nasal tissue exposed to the drug, which can be followed by septum perforation and palatine perforation caused by necrosis in the bone and cartilage structure sometimes as soon as 3 weeks of intensive exposure (2-15).In a review by Seyer et al in 2002, 7 cases of palatine perforation were described with perforations in nasal septum or paranasal sinus which progressed into hard palate.2 In these patients usually there were fast destructive processes in the midfacial region, that could suggest other entities with similar lesions, like Wegener´s granulomatosis, NK/T cell lymphoma, infections and other neoplasias, that must be considered in the differential diagnosis (10, 11, 14, 15).Here we describe a case with palatine perforation, nasal septum and maxillary sinus medial wall destruction in a patient with cocaine abuse and discuss possible differential diagnosis.
Clinical case
48 year old female presents to Maxillo facial surgery service from the Hospital General de Occidente, Secretaria de Salud Jalisco, with a two-month of evolution bucconasal communication. Psychosocial interrogation: married 3 pregnancies. Toxic or recreative drug use denied.
Surgeries, transfusions, allergies and hospitalizations denied.
Physical examination reveals flattened facial features with wide and depressed nasal dorsum. Intraoral examination asymptomatic hard palate ulcer 15 x 17 mm without inflammation signs. The patient described it appear suddenly and has had an steady slow growth inducing swallowing difficulties due to food passage to the nasal cavities and phonation dysfunction (nasal voice) (Fig. 1). Nasal fossae examination revealed septum nasal of the destruction.Routine Laboratory test , within normal ranges.

A head CT scan reported absence of nasal septum with destruction of the left maxillary medial wall (Fig. 2).
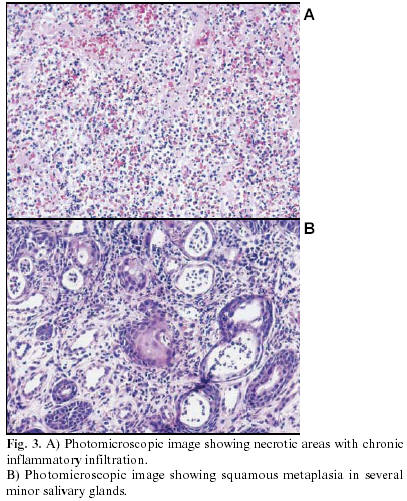
An incisional biopsy was performed revealing necrotic areas with chronic inflammatory infiltration and squamous metaplasia in several minor salivary glands (Fig. 3 A y B).
Based although on the previous data and suspecting a tisular destruction induced by cocaine the patient demied useful drugs, an antidopping test was requested upon ansent approval of the patient revealied evidence of cocaine and marijuana usage; a new interrogatory was performed insisting on the use of recreational drugs the patient confirmed the consumption of alcohol intake since the age of 20, marijuana consumption for 10 years and cocaine usage for 1 year with 1 gr. consumption per day. Final diagnosis chronic ulcer due to cocaine intranasal exposure.
The patient was treated with a palatine obturator and was derived to psychological consultation. A surgical fistulae closure was advised but the patient did not return for follow up.
Discussion
Cocaine is derived from coca leaves. Its production includes the transformation of the leaves into a paste and then into cocaine clorhydrate using catalyst agents like ether, sulphuric acid and gasoline (1).
Cocaine induces vasoconstriction and might cause necrosis in the mucosae and surrounding tissues (cartilaginous and osseous). Frequent contact induces nasal septal destruction, choanae, paranasal sinus walls and palatine (2).
Ulcerative lesions affecting the midface were considered for differential diagnosis including traumatic, infectious and neoplasic, such as Wegener´s granulomatosis, nasal NK/T cell lymphoma and mucormycosis. Though unfrequent rhinoscleroma and other lymphomas must be also considerer (2,16)
Wegener granulomatosis causes a necrotic granulomatose lesion, this is an unfrequent condition that shows respiratory tract should granulomatose ulcers, glomerulonephritis patients develop and in some cases can be developed. This disease stars with purulent nasal discharge, chronic pain in maxillar sinus, fever, nasal congestion and nasal ulceration. Middle ear and epistaxis are also described. 6% of the affected patients have oral involvement. The characteristic lesion is a granulomatose gingivitis with strawberry appearance, the tissue turns fragil and erythematous; osseous destruction and displacement of teeth is also observed.
The diagnosis is base on the clinical and pathological observations aided by laboratory studies like indirect immunoflourecence by the detection cytoplasmic antibodies against neuthrophiles (ANCAs), a useful serologic marker in this diagnosis (3,9,11,12,16)
NK/T cell lymphoma must be considered when studying this type of lesions; this lymphoma is common in Asian population and in some Latinoamerican countires like Peru, Guatemala and Mexico, where it has been associated with Epstein-Barr virus. The affected patients are adults that develop midface destruction in the nasal area with pain and epistaxis. The oral cavity shows a rapidly destructive ulcer in the palate midline inducing a painful buccosinus fistulae with halitosis and general malaise. The diagnosis is achived by accurate clinical and pathological correlation aided by inmunohistochemical studies (3,12).
Mucormycosis is another differential diagnosis. This infection is caused by fungi in the class of Zygomycetes which are opportunistic saprophytic fungi from the genres Absidia, Mucor, Rhizomucor y Rhizopus, that can cause rhinocerebral affection. This is most commonly observed in uncontrolled insulin dependent diabetic patients with ketoacidos and immunosupression.
The usual clinical signs included nasal obstruction, epistaxis, facial pain, headache, periorbital and facial swelling with signs of orbital cellulites, visual, decrease and proptosis and in some cases facial palsy can be observed. The progression of the infection without adequate treatment induces lethargus, blindness, seizures and death. The maxillary sinus is commonly involved in alveolar processes, palate or both. diagnosis is confirmed by the histological finding of characteristic non septate irregular hyphae up to 30 micra in diameter.
We can conclude that intranasal cocaine abuse can induce necrosis and focal ischemia that causes secondary mucosa and midfacial bone destruction, and must be differentiated from aggressive neoplasias, inflammatory or infectious processes.
![]() Correspondence:
Correspondence:
Dr. Miguel Padilla Rosas
Laboratorio de Microbiologia Molecular
CIBO, IMSS
Sierra Mojada 800,
Col. Independencia,
C.P. 43340, Guadalajara, Jalisco. México.
E-mail: miguelpadilla_rosas@hotmail.com
Received: 15-04-2005
Accepted: 22-01-2006
References
1. Catterall W, Mackie K. Anestesicos locales. En Hardman J, Limbird L, Molinoff P, Ruddon R, Gilman A. Las bases farmacológicas de la terapéutica: México: Edit. McGraw-Hill Interamericana. Novena edición; 1996. p. 353-60. [ Links ]
2. Seyer A B, Grist W, Muller S. Aggressive destructive midfacial lesion from cocaine abuse. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;44:465-70. [ Links ]
3. Williams N. What are the causes of a perforated nasal septum?. Occup Med 2000;50:135-6. [ Links ]
4. Gendeh BS, Ferguson BJ, Johnson JT, Kapadia S. Progressive septal and palatal perforation secondary to intranasal cocaine abuse. Med J Malaysia 1998;53:435-8. [ Links ]
5. Kuriloff BD, Kimmelman CP. Osteocartilaginous necrosis of the sinonasal tract following cocaine abuse. Laryngoscope 1989;99:918-24. [ Links ]
6. Mattson-Gates G, Jabs AD, Hugo NE. Perforation of the hard palate associated with cocaine abuse. Ann Plastic Surg 1991;26:466-8. [ Links ]
7. Gándara JM, Diniz M, Gándara P, Blanco A, García A. Lesion of the oral mucosa in cocaine users who apply the drug topically. Med Oral 2002;7:103-7. [ Links ]
8. Sittel C, Eckel, HE. Nasal cocaine abuse presenting as central facial destructive granuloma. Eur Arch Otorhinolaryngol 1998; 255: 446-7. [ Links ]
9. Becker GD, Hill S. Midline granuloma due to illicit cocaine use. Arch Otolaryngol Head Neck Surg 1998;114:90-1. [ Links ]
10. Sastry RC, Lee D, Har-el G. Palate perforation from cocaine abuse. Arch Otolaryngol Head Neck Surg 1997;116:565-6. [ Links ]
11. Armstrong M. Jr., Shikani AH. Nasal septal necrosis mimicking Wegener´s granulomatosis in a cocaine abuser. ENT J 1996;75:623-7. [ Links ]
12. Kwong YL, Chan AC, Liang, RH. Natural killer cell lymphoma/leukemia: pathology and treatment. Hematol Oncol 1997;15:71-9. [ Links ]
13. Deutsch HL, Millard DR. A new cocaine abuse complex. Arch Otolaryngol Head Neck Surg 1998;114:90-1. [ Links ]
14. Vilensky W. Illicit and licit drugs causing perforation of the nasal septum. J Forensic Sci 1982;27:958-62. [ Links ]
15. Romo T, Sclafani AP, Falk AN, Toffel PH. A Graduated approach to the repair of nasal septal perforations. Plast Reconstr Surg 1999; 103: 66-75. [ Links ]
16. Trimarchi M, Gregorini G, Facchetti F, Morassi ML, Manfredini C, Maroldi R, et al. Cocaine-induced midline destructive lesions: Clinical, radiographic, histopathologic, and serologic features and their differentiation from Wegener granulomatosis. Medicine 2001;80:391-404. [ Links ]
17. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. Philadelphia: W.B. Saunder Company. 1995. p. 175-6. [ Links ]

