










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Pharmacy residency is usually defined as education a pharmacist can pursue beyond the degree required for licensing as a pharmacist, with often a primary clinical focus and a hospital or health system organization environment.1,2 This post-graduate formation permits to increase professional knowledge and experience for applicants and to acquire specific skills and competence in various pharmacy specialties, in particular in the expanding domain of pharmaceutical care.3,4
It is however noteworthy that the nature, modalities and professional goals of pharmacy residency are quite different according to countries. In United States of America (USA), pharmacy residency lasts one or two years and corresponds to accredited programs, mostly concerning clinical pharmacy.1 The first year is generally referred to as post graduate year 1 (PGY1) and is aimed at enhancing general competencies in managing medication-use systems and supporting optimal medication therapy outcomes for patients with a broad range of diseases. The second year, referred to as post graduate year 2 (PGY2), is focused on a specific area of practice state, possibly leading to pharmacy specialty certification.3 In Canada, a pharmacy residency consists of one year of structured rotations in an hospital settling5, covering various aspects such as pharmacy practice and administration, internal medicine, pediatrics, cardiology, surgery, nephrology, gastrointestinal systems, emergency medicine, intensive care, ambulatory care, and toxicology.6 In France, residency for pharmacists, termed "Internat de Pharmacie", lasts four years and takes place in university hospitals associated with pharmacy faculties.7 French pharmacy residents enroll into one of the three defined pharmacy residency specialties: "Medical Biology", "Hospital Pharmacy" and "Pharmaceutical Innovation and Research". "Medical Biology", also known as clinical biology, and corresponding to clinical pathology in USA and United Kingdom or to laboratory medicine in Germany, is a medical specialty, thus accessible not only to physicians via medical residency, but also to pharmacists in France only via pharmacy residency.8 Beside France, pharmacy students can also specialize into clinical biology in some countries, including Portugal, Belgium, Switzerland and Algeria.9 "Hospital Pharmacy" program is primarily aimed at forming French hospital pharmacists10, whereas "Pharmaceutical Innovation and Research" specialty concerns health domains not formally covered by medical biology or hospital pharmacy such as cell therapy, biotechnology, hospital hygiene or nutrition, with a special emphasis on performing along a research program in interest area, i.e., a master of science ideally followed by a PhD thesis.
The modalities for getting a residency program also differ according to countries. In USA, selection occurs through resident matching program (the "Match"), supervised and sponsored by The American Society of Health-System Pharmacists, which places applicants into pharmacy residency training positions.11 By this way, ranking by programs, generally based on applicants' scores calculated using screening tools and onsite interviews12, is confronted to program preferences established by candidates. A similar matching service is also operating in Canada for assigning pharmacy residents to residency positions.13 In France, pharmacist students have access to residency after passing a national, knowledge-based and written ranking examination. This national examination takes place each year and can be passed twice over a 3 year-period, as soon as students reach the 5th year of French Pharm D program. By national ranking order, residency-admitted pharmacy students next choose their specialty, among the three pharmacy residency programs reported above, in a defined university hospital, knowing that twenty-three university hospitals spread over France can receive pharmacy residents. Specialty programs have therefore no influence on the selection of residency candidates in France. Numbers of residency positions available by specialty and university hospital are strictly and jointly regulated by the French ministries of Health and Universities, leading by this way to national quota by specialty.
Various factors have been shown to contribute or predict the success to the resident matching program in the USA.14,15,16,17 Reasons for which pharmacist students decide to pursue a hospital pharmacy residency have also been investigated in North America.18,19 By contrast, little data, if any, about these issues have been reported for French pharmacy residency, notably with respect to the factors involved in the choice of the professional program by residency-admitted applicants. The present study was designed to gain insights about this point, through focusing on the relationship between the national residency examination ranks and the specialty to which French pharmacy residency-postulants were finally admitted.
METHODS
Data about national examination ranks, acceptance in residency specialty and hospital assignment were obtained from public lists of pharmacy residency-admitted candidates, available on the website of the French national center of management in charge of the organization of the residency examination.20 Data were collected from four recent national examinations having taken place in year 2013, year 2014, year 2015 and year 2016. They were included in a dedicated Microsoft Excel data base, allowing next to divide admitted candidates into three categories according to their residency program ("Medical Biology", "Hospital Pharmacy" and "Pharmaceutical Innovation and Research"). For each category, rank median, i.e., the rank that separates the half best ranked from the half worse ranked within the category, and limit rank, i.e., the examination rank of the last candidate admitted in the category, that corresponds to the worse ranked, were determined. Within each category, the number of theoretical specialty choices for students definitively admitted in the specialty was also determined according to limit ranks; data were expressed as percentages of the total population definitively admitted in each specialty having three, two or only one possible choices of specialty.
Within the categories of "Medical Biology" and "Hospital Pharmacy", a sub-classification by hospital was additionally performed and limit ranks were identified for each sub-category; such limit ranks were next used to rank university hospitals from the most selective (with the lowest limit rank value) to the least selective (with the highest limit rank value). A global index was then determined for each university hospital through adding the rank for "Medical Biology" and that for "Hospital Pharmacy"; this index was finally used for a global ranking of university hospitals, from the global most selective university hospital (with the lowest index value) to the least selective (with the highest index value).
Demographic data about the total number of French pharmacists exerting medical biology as well as that of French hospital pharmacists in exercise on 1 January 2016 were found on the website of the French national college of pharmacists.21 This next allowed to determine rates of number of admitted residents per year versus total number of practitioners for the "Medical Biology" and "Hospital Pharmacy" specialties, i.e., training fluxes per specialty, using the following equation:

Some data relative to examination ranks were graphically represented as box and whiskers plots. The box corresponds to the interquartile range. The line inside the box is plotted at the median, whereas the whiskers go from the smallest rank up to the largest rank.
Descriptive statistics include means and standard deviation (SD) of rank medians and limit ranks for category or sub-categories from the four national ranking examinations included in the study. The statistical test used for assessing differences between more than 2 groups was one-way analysis of variance (ANOVA) followed, if appropriate, by a post-hoc Tukey's test. Correlation of the university hospital ranking according to "Medical Biology" specialty selectivity to that performed for "Hospital Pharmacy" specialty was investigated using the non-parametric Spearman rank-order method. For all of the analyses, a p-value less than 5% was considered significant. The data were analyzed using GraphPad Prism 6 software (GraphPad software, La Jolla, CA).
RESULTS
Numbers of residency-admitted pharmacy students categorized by specialty and by year of examination are summarized in Table 1. The total number of residency-admitted subjects included in the study is n=1948. The largest category corresponds to "Pharmacy Hospital" (n=1175, corresponding to 60.3% of the total population), followed by "Medical Biology" specialty (n=591, representing 30.3% of the total population), whereas the least numerous category is "Pharmaceutical Innovation and Research" (n=182, representing 9.3% of the total population) (Table 1). The means of resident numbers per year and specialty are indicated in Table 1. They were used for determining annual demographic rates of admitted pharmacist residents for the specialties "Medical Biology" and "Hospital Pharmacy" relative to the total number of pharmacists exerting these specialties in France on 1 January 2016 (n=7467 for "Medical Biology" and n=6991 for "Hospital Pharmacy").21 These annual training fluxes are 1.98% and 4.2% for the specialties "Medical Biology" and "Hospital Pharmacist", respectively.
Table 1 Number of pharmacy residency-admitted students enrolled in the study.
| Specialty | Total number | |||
|---|---|---|---|---|
| Medical Biology | Hospital Pharmacy | Pharmaceutical Innovation and Research | ||
| Examination Year 2013 | n=140 | n=292 | n=44 | n=476 |
| Examination Year 2014 | n=147 | n=293 | n=46 | n=486 |
| Examination Year 2015 | n=150 | n=297 | n=46 | n=493 |
| Examination Year 2016 | n=154 | n=293 | n=46 | n=493 |
| Total number | n=591 | n=1175 | n=182 | n=1948 |
| Mean (SD)/examination | n=147.8 (5.9) | n=293.8 (2.2) | n=45.5 (1.0) | n=487.0 (8.0) |
Distributions of examination ranks by specialty and examination year are indicated in Figure 1. For each examination year, examination ranks significantly differ for the three residency categories, with the lowest ranks for the specialty "Medical Biology" and the highest ranks for the specialty "Pharmaceutical Innovation and Research". Such differences between examination rank levels for the three residency specialties were fully confirmed when considering median ranks and limit ranks for each category from the four considered examination years (Table 2). "Medical Biology" was thus the specialty with the significantly lowest median and limit ranks, and appears thus as the most selective specialty, whereas the highest median and limit ranks were observed for "Pharmaceutical Innovation and Research" specialty, that is therefore the least selective (Table 2). According to limit ranks for admission in a specialty, we next determined the number of theoretical specialty choices for each resident category (Table 3). Residents admitted in the specialty "Medical Biology" have theoretically all access to the three residency specialties, whereas those admitted in the specialty "Hospital Pharmacy" have, for most of them (corresponding to 91.9% of the total student population definitively admitted in "Hospital Pharmacy"), only two theoretical choices, i.e., "Hospital Pharmacy" and "Pharmaceutical Innovation and Research". Students retained for the specialty "Pharmaceutical Innovation and Research" have, for the majority of them (representing 64.1% of the total student population definitively admitted in the specialty "Pharmaceutical Innovation and Research"), only accessed to this specialty according to their examination rank (Table 3).
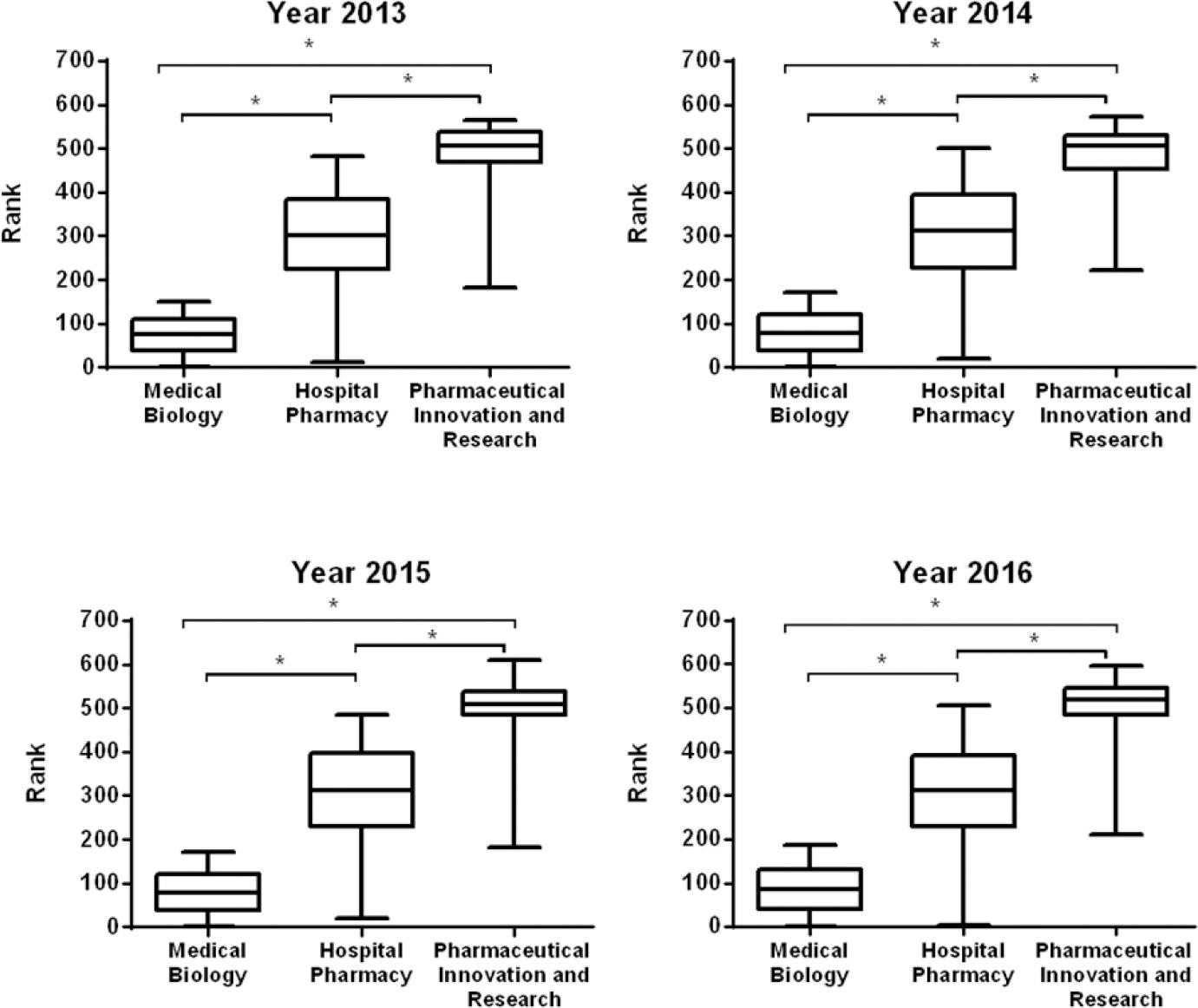
Figure 1 Pharmacy residency examination ranks for admitted postulants categorized by the pharmacy specialty in which they were definitively admitted. *, p<0.05.
Table 2 Median and limit examination ranks for the choice of pharmacy residency specialty a
| Examination rank | Specialty | ||
|---|---|---|---|
| Medical Biology | Hospital Pharmacy | Pharmaceutical Innovation and Research | |
| Median rank | 79.4 (5.1)* | 309.9 (5.0)* | 509.4 (7.3)* |
| Limit rank | 172.0 (16.5)* | 492.3 (11.4)* | 585.7 (21.0)* |
aData shown are the means (SD) of ranks from the pharmacy residency examinations having taken place in 2013, 2014, 2015, and 2016.
*p<0.05 when compared to other specialties.
Table 3 Number of possible specialty choices for residency-admitted candidates categorized by their definitive specialty admission.
| Number of possible specialty choices according to examination rank | Percentage of residency-admitted candidates in the specialty | ||
|---|---|---|---|
| Medical Biology | Hospital Pharmacy | Pharmaceutical Innovation and Research | |
| n=3b | 100.0 (0.0%) | 8.1 (3.1%) | 0 (0.0%) |
| n=2c | 0 (0.0%) | 91.9 (3.6%) | 35.9 (7.9%) |
| n=1d | 0 (0.0%) | 0 (0.0%) | 64.1 (7.9%) |
aData shown correspond to percentage of the total population definitively admitted in the specialty and are the means (SD) of values from the pharmacy residency examinations having taken place in 2013, 2014, 2015 and 2016.
bThe three possible choices are Medical Biology, Hospital Pharmacy, and Pharmaceutical Innovation and Research.
cThe two possible choices are Hospital Pharmacy and Pharmaceutical Innovation and Research.
cThe one only possible choice corresponds to Pharmaceutical Innovation and Research.
It is noteworthy that the limit ranks for "Pharmaceutical Innovation and Research" were always beyond the total number of resident positions, thus illustrating the fact that some pharmacist students initially admitted to pharmacy residency according to their examination rank finally renounced to take a resident position. This population of admitted candidates who failed to accept a post-graduate stage corresponds to n=98.7 (SD=14.2) candidates. Their rank median was 518.6 (SD=20.8), indicating that the majority of these students was among the worse ranked ones, that had only access to the specialty "Pharmaceutical Innovation and Research" according to limit ranks for the choice of specialties.
We finally determined limit ranks for each university hospital and for the two specialties numerically the most important, i.e., the specialties "Medical Biology" and "Hospital Pharmacy" (Table 4). For the program "Medical Biology", these ranks ranged from 42.8 (SD=21.5) (for Nantes university hospital) to 167 (SD=13.3) (for Reims university hospital) and were significantly different between university hospitals (p<0.0001). Limit ranks for "Hospital Pharmacy", that ranged from 266.7 (SD=33.6) (for Lyon university hospital) to 487 (SD=17.4) (for Nancy university hospital), also significantly diverged according to university hospitals (p<0.0001). For each specialty, we next ranked university hospitals according to their rank limits, from the most selective university, i.e., that with the lowest limit rank, to the least selective, i.e., that with the highest limit rank (Table 4). Interestingly the university hospital ranking for "Medical Biology" was found to be significantly correlated to that for "Hospital Pharmacy" (Figure 2). Through adding the hospital university rankings for "Medical Biology" and "Hospital Pharmacy", we finally established a global university hospital ranking for residency pharmacy selectivity (Table 4). The university hospital of Lyon, formally termed "Hospices Civils de Lyon", is at the top of this global ranking (Table 4).
Table 4 Ranking of university hospitals according to residency examination limit ranks for the pharmacy residency specialties Medical Biology and Hospital Pharmacy.
| University hospital | Medical Biology | Hospital Pharmacy | Global ranking | |||
|---|---|---|---|---|---|---|
| Limit rank a | University hospital ranking b | Limit rank a | University hospital ranking b | Index c | University hospital ranking d | |
| Amiens | 160.7 (9.9) | 20 | 451.5 (24.7) | 17 | 37 | 18 |
| Angers | 85.7 (26.3) | 5 | 358.2 (77.2) | 4 | 9 | 4 |
| Besançon | 132.5 (41.3) | 14 | 485.5 (11.6) | 22 | 36 | 17 |
| Bordeaux | 63.5 (22.8) | 3 | 312.5 (43.4) | 2 | 5 | 2 |
| Caen | 161.5 (16.8) | 21 | 471.7 (7.2) | 20 | 41 | 21 |
| Clermont-Ferrand | 130.7 (15.7) | 13 | 396.5 (13.0) | 9 | 22 | 11 |
| Dijon | 166.3 (22.7) | 22 | 447.7 (26.9) | 15 | 37 | 18 |
| Grenoble | 146.5 (25.7) | 16 | 354.7 (18.9) | 3 | 19 | 9 |
| Lille | 121.2 (37.7) | 10 | 423.7 (10.0) | 13 | 23 | 13 |
| Limoges | 100.3 (25.4) | 6 | 420.7 (36.3) | 12 | 18 | 7 |
| Lyon | 46.2 (14.8) | 2 | 266.7 (33.6) | 1 | 3 | 1 |
| Marseille | 133.0 (15.9) | 15 | 449.7 (25.8) | 16 | 31 | 15 |
| Montpellier | 109.2 (12.0) | 7 | 380.5 (41.4) | 7 | 14 | 6 |
| Nancy | 153.2 (31.6) | 19 | 487.0 (17.4) | 23 | 42 | 22 |
| Nantes | 42.8 (21.5) | 1 | 363.0 (11.8) | 5 | 6 | 3 |
| Paris | 124.0 (10.6) | 12 | 415.5 (22.2) | 10 | 22 | 11 |
| Poitiers | 147.2 (20.6) | 17 | 445.5 (14.5) | 14 | 31 | 15 |
| Reims | 167.0 (13.3) | 23 | 484.5 (17.4) | 21 | 44 | 23 |
| Rennes | 121.2 (14.2) | 10 | 394.2 (45.4) | 8 | 18 | 7 |
| Rouen | 150.5 (13.4) | 18 | 468.0 (5.7) | 19 | 37 | 18 |
| Strasbourg | 120.2 (50.3) | 9 | 452.0 (26.2) | 18 | 27 | 14 |
| Toulouse | 69.0 (10.6) | 4 | 364.2 (28.4) | 6 | 10 | 5 |
| Tours | 116.2 (39.7) | 8 | 420.2 (19.1) | 11 | 19 | 9 |
aData shown are the means (SD) of ranks from the examinations having taken place in 2013, 2014, 2015 and 2016.
bUniversity hospitals were ranking from that having the lowest resident limit rank (the most selective one) to that having the highest resident limit rank (the least selective one).
cIndex is defined as the sum of university hospital rankings for "Medical Biology" and "Hospital Pharmacy" specialties.
dGlobal ranking according to index value, from the most selective (lowest index value) to the less selective (highest index value) university hospital.

Figure 2 Correlation between university hospital rankings according to "Medical Biology" selectivity versus that established from "Hospital Pharmacy" selectivity. University hospitals were ranked from the most to the less selective for pharmacy specialties. Spearman's rank coefficient=0.75 and p<0.0001.
DISCUSSION
In the present study, we demonstrated that the specialty choice for hospital residency-admitted French pharmacy students is highly associated with their rank at the national pharmacy residency examination. The best ranked students, for most of them, retain "Medical Biology" for their specialty whereas the majority of the "worse ranked" ones have only the choice of "Pharmaceutical Innovation and Research" specialty. The candidates displaying an intermediate examination rank, behind that required for "Medical Biology", choose predominantly "Hospital Pharmacy". The examination rank, which can be assumed to reflect background pharmacy academic level, appears thus as a major contributing factor to the choice of pharmacy residency specialty for French pharmacy students. Similarly, the background academic level, exemplified by pharmacy school grade point average (GPA), was higher for postulants who matched to the residency program in USA compared to those who did not.14 This implication of the examination rank/academic level of postulants for the choice of specialty likely results in an implicit hierarchy of French pharmacy residency specialties. The specialty "Medical Biology" is at the top of this ranking, followed by "Hospital Pharmacy" and, at the end, the specialty "Pharmaceutical Innovation and Research". This hierarchy was similarly observed for each of the four annual pharmacy residency examinations analyzed in our study, thus likely indicating that it corresponds to a long-term trend, and not to a random process.
The reasons that may underlie such an apparent hierarchy of pharmacy specialties for French pharmacy residents remain to be established and are likely to be of various and different natures. One of them may reflect legal monopolistic aspects of the professional exercise of some of the specialties. Indeed, for French pharmacists, exercise of "Medical Biology" as well as now that of "Hospital Pharmacy" are regulatory restricted to pharmacy residents that have validated the specialty; in other words, within the pharmacy profession, residency pharmacists admitted in these two specialties will get the monopole of the exercise of these specialties. By contrast, area theoretically covered by the specialty "Pharmaceutical Innovation and Research" such as cell therapy or biotechnology, are also opened to pharmacists that do not perform residency and also to scientists without the requirement of a PharmD diploma. This lack of a professional monopole may likely correspond to a major reason explaining why "Pharmaceutical Innovation and Research" specialty is a rather neglected specialty for pharmacy residents. The low attractiveness of this specialty is moreover likely highlighted by the fact that a notable contingent of residency candidates, whose examination ranks allowed them to access to only "Pharmaceutical Innovation and Research", prefer to renounce to finally get a residency position. Such students may take the pharmacy residency examination again, with the hope to be better ranked for choosing "Medical Biology" or "Hospital Pharmacy" specialties or, alternatively, they may devote themselves to other pharmacy area such as community pharmacy or pharmaceutical industry.
Another reason that may contribute to the fact that residency-admitted candidates preferentially choose "Medical Biology" specialty may be due to the variety of professional practice models for this specialty. Indeed, pharmacist may exert medical biology as employee in public hospital laboratory, in private hospital laboratory or in private clinical laboratory or as owner of a private clinical laboratory, knowing that this last practice is rather profitable. By contrast, hospital pharmacists are obligatory employed in public or private hospital, without having the opportunity of exerting as independent liberal health professionals and, by this way, of developing their own business. Moreover, the rate of annual formation of new medical biologists via residency pharmacy is rather low, i.e., the annual number of new graduates in "Medical Biology" corresponds thus to approximately 2% of the total number of pharmacists exerting "Medical Biology" in France. This rather strict quota for "Medical Biology" likely contributes to the fact that this specialty is the most competitive. It may theoretically guaranty excellent professional perspectives for residents choosing this specialty and may discard any joblessness through preventing any oversupply of graduates, even if the sector of medical biology in France as in other countries currently displays marked and deep changes.22,23 Indeed, French medical biology laboratories are presently subject to laboratory consolidation, restructuration and accreditation24, with potential implication of commercial companies, which may result in a reduction of the number of positions for clinical laboratory directors in the future.22 With respect to the "Hospital Pharmacy" specialty, the rate of annual formation of new hospital pharmacists (about 4.2%) is approximately twice than that for new medical biologists. This may reflect the fact that the development of new missions for pharmacists, notably related to clinical pharmacy, is expected to result in increased job opportunities for hospital pharmacists, thus requiring a high number of new graduates. However, there is some concerns about the fact that the expansion of the number of pharmacy graduates may in fact lead to an oversupply of pharmacists25; a consequent potential joblessness crisis could therefore happen26, notably in USA and the United Kingdom, which exhibit a recent marked and continuous increase in the total number of pharmaceutical faculties and schools.27 In this context, the adequacy between the relative high number of pharmacy residents enrolled in the "Hospital Pharmacy" way in France and the reality of the French job market for hospital pharmacists in the next years may be questionable, which may prevent some residency-admitted candidates to choose this specialty.
The marked attractiveness of the "Medical Biology" specialty compared to the other pharmacy residency specialties may also result from the variety of area covered by this specialty, including clinical chemistry, microbiology, hematology, immunology and pharmacology and their established, recognized and crucial relevance for medical diagnostic and follow-up, and beyond, to the care and the management of patient. In addition, "Medical Biology" specialty appears as a full medical specialty in France and may therefore be considered to benefit from the prestige of medical activities and to their full and well-recognized professional status according to the sociological concept of professions.28 By contrast, hospital pharmacists, like community pharmacists, have been hypothesized to not entirely fulfill the criteria characterizing a complete profession, notably because they have been claimed to have not gained control of their social object that is the drug.29 Indeed, drugs are primarily and regulatory prescribed to patients by physicians, mostly without direct implication of pharmacists; evaluation of the clinical effects of drugs is also firstly assumed by physicians. By this way, the profession of hospital pharmacist may be perceived by pharmacy residency candidates as exhibiting social power and professional status lower than those attributed to the profession of medical biologist. The new and emerging clinical roles for hospital and community pharmacists3,4,30,31 32 are however likely to challenge this assertion, even if these new clinical missions for pharmacists have been postulated to be less developed for the moment in France than in other countries.33
When applied to university hospitals and for the specialty "Medical Biology" and "Hospital Pharmacy", analysis of limit ranks allowed discriminating university hospitals, from the most selective to the least selective over the 2013-2016 residency examination period analyzed in the present study. Interestingly, the university hospital ranking for the specialty "Medical Biology" was significantly correlated to that for the specialty "Hospital Pharmacy", suggesting that the university hospital rankings likely reflect the global attractiveness of the university hospitals for pharmacy residents rather than that for a defined pharmacy residency specialty. The basis for such a differential selectivity of university hospitals with respect to the pharmacy residents remain to be determined. The ratio number of candidates/number of available resident positions, the repute of each university hospital, notably in terms of scientific research and pharmacy projects, and the attractive geographical location of some of the cities where university hospitals are located may be ones, among others, factors that contribute to the selectivity. Otherwise, each French university hospital is affiliated to one faculty of pharmacy, excepted for Paris university hospital (formally termed "Assistance Publique-Hôpitaux de Paris") to which two faculties of pharmacy, that of Paris-Descartes and that of Paris-Sud, are affiliated. The ranking of university hospital established according to the selectivity for pharmacy residency may consequently be transposed to French faculties of pharmacy, knowing that the two faculties of pharmacy located in Paris cannot been discriminated between them. In this context, it is noteworthy that such a tentative ranking of French faculties is most likely the first to be reported. Indeed, ranking of faculties of pharmacy according to various academic criteria, well-established in USA34, does not presently exist in France.
One of the major limitations of our study corresponds to the fact that our study is only factually descriptive, principally studying the association between the pharmacy residency examination rank and the nature of the specialty in which residency candidates are finally admitted. Beyond the examination rank, the exact nature of the motivations of French pharmacy students to do residency pharmacy and to prefer one residency specialty comparatively to the others, remain therefore to be clarified. This may likely be performed through a survey addressing these issues with pharmacy residency candidates, as already done for identifying predictors for postgraduate matching success in USA14 or factors motivating students to pursue a hospital residency in Canada.19 With respect to our tentative ranking of university hospitals and affiliated faculties of pharmacy, it is noteworthy that such a ranking is based on only one criteria, i.e., pharmacy residency selectivity; it has therefore rather a limited value and has to be improved in a major manner by considering various other criteria as already done in USA.34 In particular, the rate of success to residency for each faculty of Pharmacy, i.e., the ratio number of admitted candidates versus number of initial candidates from each faculty, is likely an important factor that remains to be established. Finally, our study is primarily related to the access and organization of pharmacy residency programs in France. It is therefore likely not directly transposable to other countries. The perception of pharmacy specialties such as "Medical Biology" and "Hospital Pharmacy" by French pharmacy students may however be shared by pharmacy students outside of France, notably in countries in which pharmacy students can have the choice between clinical biology and hospital pharmacy for specializing.
CONCLUSIONS
The present study demonstrated that the specialty choice for hospital residency-admitted French pharmacy students is closely associated with their national examination rank, which may be postulated to formally reflect their academic level. This likely implicitly ranks pharmacy residency specialties in France according to background academic level of residency candidates, with at the first place "Medical Biology", followed by "Hospital Pharmacy" and at the end "Pharmaceutical Innovation and Research". Such a hierarchy may have to be taken into account by French pharmacy academic and hospital stakeholders when considering pharmacy residency specialties, especially owing to their present status and perception by French pharmacy students and their expected evolutions in the future.

