










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Worldwide, 56 million people died in 2017, 31.8% of whom (17.79 million) died from cardiovascular disease (CVD), which remains the leading cause of mortality across the world.1 In Portugal, the Portuguese General Health Directorate in collaboration with the National Statistics Institute monitors the CVD mortality and morbidity indicators after receiving the database of diagnosis-related groups of inpatient episodes from the Central Administration of the Health System. CVD has been the leading cause of death in Portugal since 1955 (26.5% of total deaths), reaching a peak of 44.3% in 1985, stabilizing in 1990, and then declining over the last three decades due to risk factor control.2 However, in 2018, CVD, particularly stroke and coronary heart disease, continued to be the leading cause of death in Portugal and was responsible for 29.0% of total deaths.3 Despite improvements in mortality and CV morbidity indicators, it is necessary to continue to reduce premature deaths and delay the development of CVD. The Portuguese General Health Directorate, through the "National Program for the Prevention and Control of CVD" intended to improve the monitoring of CV risk factors at the primary health care level by promoting periodic health examinations comprising a systematic assessment of global CV risk as a daily professional practice of physicians.4 In 2017, with the "National Program for Cardiovascular and Cerebrovascular Diseases", the main goals were shifted towards secondary prevention, and the systematic assessment of global CV risk as a daily professional practice for all patients was removed.5 However, a comprehensive CVD prevention and control program should include both effective treatment interventions and population-wide interventions to reduce the levels of upstream CVD determinants. Thus, it will be important to continue to monitor CVD risk factors in screening programs, and community pharmacists can be included to maximize universal health coverage, as pharmacies have an optimal wide geographical coverage and the required qualifications; this would expand the scope of professional practice for pharmacists.6,7 Assessing the global CVD risk in individuals is of major importance to identify and adequately manage patients and their modifiable risk factors, such as dyslipidemia, tobacco use, diabetes, hypertension, obesity, physical inactivity, harmful alcohol use, and unhealthy diet, which account for approximately 90% of myocardial infarction risk in women and men and all age groups around the world.8 Nonidentification and inappropriate monitoring of at-risk groups can have serious consequences, as 25% of CVD patients have sudden cardiac death or nonfatal myocardial infarction without prior symptoms or knowledge of their existing CVD.9
Early detection of at-risk patients through global CVD risk estimation is crucial to reduce the development of CVD.10,11,12,13 A method for estimating global CVD risk of the population is to implement standardized community-based CV risk assessment programs, which require the involvement and coordination of all health professionals who assist the patients.14,15 The Portuguese community pharmacist scope of practice was expanded in 2018 to include new services routinely provided and established by law: nutrition appointments; therapy adherence programs, medicine reconciliation, services utilizing multicompartment aids, and education programs on the use of medical devices; performance of rapid tests for HIV, HCV, and HBV screening (point-of-care tests), including pre- and posttest counseling and referral of positive cases to hospital care; and plain nursing services.16 Pharmacies may also promote campaigns and programs for health literacy, disease prevention and healthy lifestyle promotion. Most Portuguese pharmacies have point-of-care tests that enable CVD risk screening. These services are freely priced by pharmacies and paid out-of-pocket by users, but there are no publicly available data on the number of services or pricing.17
In recent years, there have been efforts to broaden the role of community pharmacists beyond the traditional product-oriented functions of dispensing medication and to take a proactive, responsible role in public health.18 Patient outcomes can be improved by extending the scope of services provided by community pharmacists to CVD risk assessment and cardiovascular health management if pharmacy users accept new pharmacy care services.19-24 A large body of evidence shows that community pharmacist-led screening programs for CVD have been successful, as a significant number of previously unknown cases of CVD risk factors such as hypertension, hypercholesterolemia and diabetes have been identified, and that services for CVD risk screening have a positive impact.25-27 An example of a CVD risk screening program in community pharmacies in Iran also showed success in identifying patients with CVD risks.28
Preventive health checks are a key feature of anticipatory care, and the effectiveness of CVD prevention programs depends on participation rates.30 Therefore, high and equitable participation is crucial to ensuring health gain and preventing health inequalities, and it requires patients and physicians to recognize the clinical skills of pharmacists.31,32 A study by the National Health Service on the CVD risk profile of the Portuguese population revealed a high prevalence of CVD risk factors and the need for health authorities to develop strategies to screen the general population for CVD risk factors.33
This study aims to evaluate the feasibility of the whole process of CVD risk screening in Portuguese community pharmacies, including the characterization of the profile of the community pharmacy customers, the evaluation of their acceptability of CVD risk assessment by the pharmacist, the evaluation of the reasons for nonattendance, and the assessment of CVD risk status and CVD risk factors identified among the customers.
METHODS
Study design
In May 2015 (first period) and December 2016 (second period), a single-center cross-sectional study was conducted to characterize the profiles of pharmacy customers at two different time points. Afterwards, from April 2017 to October 2017, those who visited the pharmacy in the second period were invited to have their CVD risk assessed.
The recruitment process occurred in a community pharmacy of a central Portuguese city during two 70-hour working weeks. The pharmacist performed the CVD risk assessment for all participants who agreed to participate in the study in a dedicated counseling room, where privacy could be maintained within the pharmacy with no interference by routine pharmacy processes.
The inclusion criteria were customers who entered the pharmacy during the two periods. Each pharmacy customer of the second period was invited to participate in a CVD risk assessment. The exclusion criteria were customers aged <18 years, pregnant customers, and mentally disabled persons who were unable to consent.
Data collection
To understand the profile of the community pharmacy customers, we analyzed their characteristics and the purpose for entering the pharmacy, which was determined in two different periods, to observe the variability and consistency of the sample. Every pharmacy user was characterized by name, gender, age and reason for entering the pharmacy. The reasons for entering the pharmacy are listed in Table 1.
Table 1. Reasons to enter the pharmacy
| Acquisition of medicines | Prescription-only medicines; over-the-counter medicines; veterinary medicines; homeopathic medicines. |
| Acquisition of health products | Cosmetic/ body hygiene/ comfort and special nutrition products; plant protection products; food supplements; childcare articles; medical devices. |
| Assessment of physiological and biochemical parameters | Blood pressure; total cholesterol, triglycerides, glycemia, etc. |
| Information on medicine and health products | Enter the pharmacy to request information on medicines and health products. |
| Other reason | Accompany another user; make a purchase for another person; pick up a reservation; pay a bill; just to greet. |
To avoid any selection bias, the pharmacist contacted each customer, used a standard invitation speech in every phone call, clarified possible doubts, scheduled an appointment for data and sample collection, and informed the customer about the requirement to fast beforehand and bring all medications. The pharmacist registered the readiness to accept and the reasons for nonattendance indicated by the contacted customers.
The reasons for nonattendance were categorized as follows: lack of time; being unaccustomed to participating in this type of service; being bedridden or in an institution/having cognitive impairment/being deceased; not needing a follow up at the pharmacy/being followed up by the physician; and the location not being the usual pharmacy/emigration/lack of transport.
All participants gave their written, informed consent before the encounter was initiated, and they had the opportunity to have any doubt or question they considered relevant clarified before they began their assessment.
The sociodemographic characteristics and health data were self-reported and ascertained via questionnaires. The pharmacist collected capillary blood for the analysis of blood glucose level, total cholesterol (TC), high-density lipoprotein (HDL), and triglycerides (TG) and calculated low-density lipoprotein (LDL) for in-pharmacy point-of-care testing, obtaining the results in a 6-minute workflow. The pharmacist also performed a physical examination comprising evaluation of the systolic and diastolic blood pressure (BP), heart rate, weight, height and abdominal perimeter at waist level.
Each participant was offered a card with the results obtained and the attributed CVD risk category. The pharmacist provided patient counseling regarding the CVD risk factors found, including educating on how the risk could be decreased, recommending that the results be shown to the physician at the next visit, and, whenever markedly elevated risk factors were found, verbally referring the participant to the assigned physician. For the analysis of this screening study, we included only participants who were not on CV pharmacotherapy.
The devices and the training of the pharmacist on equipment operation were provided by World Care & Diagnostics. The blood glucose levels were measured with an Accu-Chek Performa device from Roche; lipids were measured from whole blood with a Cobas b101 system from Roche. The physical examination was performed with a Tensoval Duo Control® monitor, an Exclusivas Iglesias electronic stadiometer and an anthropometric measuring tape.
Risk estimation systems have been developed to assist the assessment of CVD risk, as CVD is the product of many causal risk factors, which, in combination, result in a higher risk than single factors. In this study, SCORE charts were applied as the risk estimation systems perform better in populations that are similar to the one used to derive the system. The SCORE charts were developed by the European Society of Cardiology (ESC) retrospectively from data originating from 12 European cohorts and are calibrated to allow for different CVD mortality rates and different risk factor distributions in high- and low-risk countries. It is an objective, easy-to-use screening tool that establishes a common language of risk for healthcare professionals. The pharmacist performed the CVD risk assessment with the risk chart for low-risk European countries, in which Portugal is included, for participants 40 to 65 years of age, the relative risk chart for participants 18 to 39 years of age and women younger than 50 years, and SCORE-OP for participants older than 65, as advocated by the ESC.34,35 The variables included in the SCORE algorithm were age, sex, and three major risk factors (systolic BP, total cholesterol, and current smoking habits).
According to the ESC guidelines, the participants were classified into the following risk categories: very high risk - a calculated SCORE ≥10%; high risk - participants with markedly elevated single risk factors, in particular total cholesterol >310 mg/dL or BP ≥180/110 mmHg, or a calculated SCORE ≥5% and <10%; moderate risk - a calculated SCORE ≥1% and <5%; and low risk - a calculated SCORE <1%.34
For the participants who eligible for the relative risk SCORE, major modifiable CVD risk factors (hypertension, dyslipidemia, smoking habits, obesity, impaired fasting glucose and sedentary behavior) were considered to evaluate their risk status according to the ESC and the European Society of Hypertension Guidelines.34
Hypertension was considered from the threshold of systolic BP>130 mmHg and/or diastolic BP>85 mmHg. The dyslipidemia risk factor was considered when TC>190 mg/dl or LDL-C>70 mg/dl for very-high-risk participants, LDL-C>100 mg/dl for high-risk participants, LDL-C>115 mg/dl for low- to moderate-risk participants, or HDL-C<40 mg/dl for men/<46 mg/dl for females, or TG>150 mg/dl).34 With regard to smoking habits, only current tobacco and nicotine product users were considered. Overweight participants presenting a body mass index (BMI) >25 kg/m2 and obese participants presenting BMI >30 kg/m2 were considered at risk.34 Fasting blood glucose was classified into normal blood glucose (<100 mg/dL), impaired glucose tolerance (100-125 mg/dL), and diabetes (>126 mg/dL).36 The ESC recommends that healthy adults of all ages perform at least 150 minutes a week of moderate intensity or 75 minutes a week of vigorous aerobic physical activity or an equivalent combination thereof.34 Less physical activity than recommended was considered to indicate sedentary behavior.
Data analysis
We used descriptive statistics to explore the characteristics of the study population. To analyze possible associations between variables, we used chi-squared and Kruskal-Wallis tests for categorical variables and t-tests and ANOVA for continuous variables. For the data analysis, we used SPSS v.24 and considered a p-value lower than 0.05 to be statistically significant.
Ethical statement
Ethics approval for conducting this study was received from the Ethics Committee of the Faculty of Medicine of Coimbra University in March 2017 (reference number: CE-011/2017). Consent to publish was obtained from the participants as indicated in the Consent for Participation Form, which was part of the ethics application forms submitted to the Coimbra University Institutional Review Board.
The customers provided their consent to register their name, date of birth, and telephone number to the pharmacist/pharmacy technician/trainee during the enrollment process, signing the digital consent form developed by the National Pharmacies Association (ANF - Associação Nacional das Farmácias) available on the computer system (Sifarma 2000).
RESULTS
To clarify the flow of participants throughout the study, a diagram is presented in Figure 1. The descriptive characteristics of the pharmacy users of both periods are shown in Table 2. The flow of customers varied during the day and the week and the peaks during the day were different in the winter and the spring. The percentage of male and female customers did not vary with the weekdays (p=0.849) or with the different periods of the day (morning/afternoon) (p=0.228). Entering the pharmacy to acquire medication was the most prevalent reason, and it was more frequently reported in the morning period (p=0.004) and by male customers (p<0.001). More female customers visited the pharmacy to acquire other health products (p<0.001), and this reason showed no difference between the morning and afternoon periods (p=0.527).
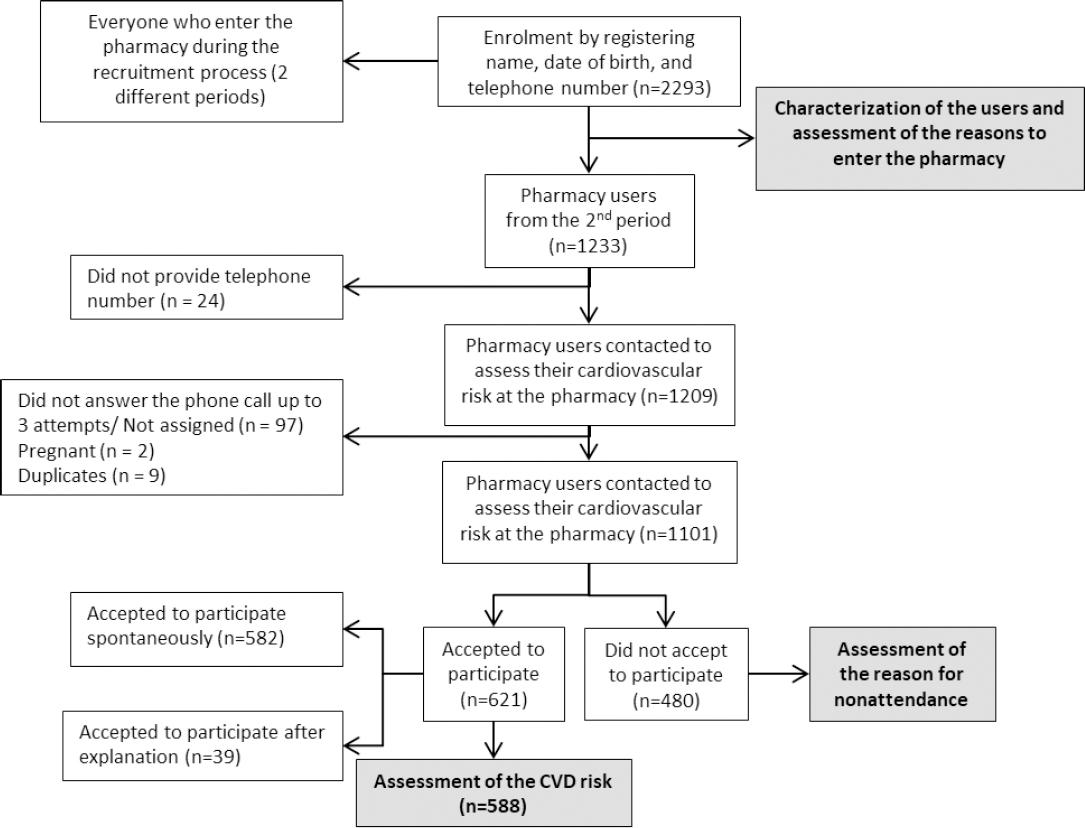
Table 2. Descriptive characteristics of the sample of the pharmacy users (n=2293)
| Characteristic | 1st period | 2nd period |
|---|---|---|
| Gender; n(%) | ||
| Male | 447 (42.2) | 516 (41.9) |
| Female | 613 (57.8) | 717 (58.1) |
| Mean age in years; mean (SD) | 55.26 (17.48) | 55.52 (17.07) |
| Minimum-Maximum | 18-101 | 18-94 |
| Regular customer; n(%) | 659 (62.2) | 811 (65.8) |
| Pharmacy staff member who attended the pharmacy customer; n(%) | ||
| Pharmacist | 679 (64.1) | 729 (59.1) |
| Pharmacy technicians | 363 (34.2) | 484 (39.3) |
| Non-clinical pharmacy staff | 18 (1.7) | 20 (1.6) |
| Reason that prompted the customer to come into the pharmacy; n(%) | ||
| Acquisition of medicines | 847 (79.9) | 753 (61.1) |
| Prescription-only medicines | 704 (66.4) | 745 (60.4) |
| Over-the-counter medicines | 213 (20.1) | 241 (19.6) |
| Acquisition of health products | 300 (28.3) | 403 (32.7) |
| Assessment of physiological and biochemical parameters | 25 (2.4) | 22 (1.8) |
| Information on medicine and health product | 10 (0.9) | 44 (3.6) |
| Other reason | 55 (5.2) | 150 (12.2) |
The assessment of physiological and biochemical parameters was a reason for visiting the pharmacy that was not influenced by gender but had more expression during the morning period (p=0.028). Asking for advice and information on medicine and health products was a reason for visiting the pharmacy that was not influenced by the period of the day (p=0.122) or the gender of the customer (p=0.661). Accompanying another customer and making a purchase for another person was more frequently reported by female customers (p=0.006) and in the afternoon period (p<0.001).
Of the customers who entered the pharmacy to acquire medicines, 36.2% (n=579) acquired at least one medicine from the CVD pharmacotherapy. More than half (64.1%, n=1470) of the customers were regular customers, the majority (65.6%, n=1504) were under 65 years of age, and the male customers were older (t=4.793, p<0.001), with a mean difference of 4.95 years.
More than half 56.4% (n=621) of the contacted customers accepted the invitation to the study, and 53.4% (n=588) actually attended the CV risk assessment. Table 3 shows the results of the reasons for nonattendance. There was no difference in acceptability between male and female pharmacy customers, and the pharmacy customers who were more likely to accept the risk evaluation were those who entered the pharmacy for the acquisition of medicines (p=0.004), elderly customers (p<0.001) and regular customers (p<0.001).
Table 3. Reasons for nonattendance to the appointment (n=1101)
| Reason | n (%) |
|---|---|
| Accepted to participate | 621 (56.4%) |
| Spontaneously accepted to participate | 582 (93.7%) |
| Accepted to participate after explanation | 39 (6.3%) |
| Did not accept to participate | 480 (43.6%) |
| Lack of time | 96 (20.0%) |
| Not used to participate in this type of services | 46 (9.6%) |
| Bedridden or in an institution/Cognitive impairment/ Deceased | 50 (46/1/3) (10.4%) |
| Do not need follow up at the pharmacy/Followed up by the physician | 205 (42.7%) |
| Not the usual pharmacy/ Migrant /have no transport | 83 (17.3%) |
Of the 588 participants, 56.6% (n=333) were already on CV pharmacotherapy (antihypertensives, antidyslipidemic medications, antidiabetic medications, antithrombotic agents, etc.) and were being followed by their physician; as such, they were not included in this screening study. The remaining 43.4% (n=255) of participants were CV pharmacotherapy naïve, and the descriptive characteristics and access to health care are shown in Table 4. CV pharmacotherapy-naïve participants were more likely to be younger, with a mean age of 46.8 years (SD 11.3), female, higher educated and employed. The median duration of the individual screening encounters was 18.2 (SD 6.3) minutes. The modifiable CVD risk factors are shown in Table 5. We found that 94.9% (n=242) of the screened participants presented at least one major modifiable CVD risk factor. In fact, 17.3% (n=44) presented one, 22.4% (n=57) presented two, 29.8% (n=76) presented three, 16.9% (n=43) presented four, 7.5% (n=19) presented five, and 1.2% (n=3) presented six CVD risk factors.
Table 4. Descriptive characteristics and health care access of the sample of the participants (n=255)
| Characteristic | n | % | p value* | ||
|---|---|---|---|---|---|
| Non-SCORE group (n=135) | SCORE group (n=120) | ||||
| Gender | 0.527 | 0.023 | |||
| Male | 76 | 29.8 | |||
| Female | 179 | 70.2 | |||
| Age | 0.244 | 0.001 | |||
| 18-49 years | 156 | 61.2 | |||
| 50-64 years | 71 | 27.8 | |||
| 65-79 years | 26 | 10.2 | |||
| >80 years | 2 | 0.8 | |||
| Regular customer (yes) | 182 | 71.4 | 0.180 | 0.395 | |
| Level of education | 0.360 | 0.367 | |||
| Illiterate 0 years | 2 | 0.8 | |||
| 1-4 years | 51 | 20.0 | |||
| 5-6 years | 28 | 11.0 | |||
| 7-9 years | 45 | 17.7 | |||
| 10-12 years | 65 | 25.5 | |||
| University or Master's degree | 63 | 24.7 | |||
| PhD | 1 | 0.4 | |||
| Professional situation | 0.894 | 0.005 | |||
| Employed | 167 | 65.5 | |||
| Unemployed | 32 | 12.6 | |||
| Retired | 41 | 16.1 | |||
| Student | 11 | 4.3 | |||
| Domestic | 4 | 1.6 | |||
| Attributed primary care physician | 0.356 | 0.102 | |||
| Yes | 240 | 94.1 | |||
| No or do not know | 15 | 5.9 | |||
| Hospitalization last year (yes) | 31 | 12.2 | 0.363 | 0.026 | |
| Resorted to the emergency services (yes) | 75 | 29.4 | 0.698 | 0.967 | |
| Difficulty buying the medicines (yes) | 28 | 11.0 | 0.768 | 0.125 | |
| Mean | Median | Min./Max. | |||
| Medical tests in the last year | 1.1 | 1.0 | 1/36 | 0.759 | 0.268 |
| Pharmacy visits (last 3 months) | 3.9 | 3.0 | 0/36 | 0.250 | 0.007 |
| Physician visits last year | 3.9 | 3.5 | 0/24 | 0.716 | 0.508 |
Table 5. Modifiable CVD risk factors (n=255)
| Characteristic | n | % | p value* | |
|---|---|---|---|---|
| Non-SCORE group (n=135) | SCORE group (n=120) | |||
| Smoking status | 0.001 | 0.575 | ||
| Non-smoker | 196 | 76.9 | ||
| Ex-smoker (<5years) | 12 | 4.7 | ||
| Smoker | 47 | 18.4 | ||
| Diet (vegetables/fruit) | 0.359 | 0.472 | ||
| Never | 0 | 0.0 | ||
| Sometimes | 52 | 20.4 | ||
| Every day | 203 | 79.6 | ||
| ≥ 5 servings/ day | 66 | 25.9 | ||
| Sedentary behavior | 0.001 | 0.398 | ||
| No | 108 | 42.3 | ||
| Yes | 147 | 57.7 | ||
| Alcohol consumption | 0.845 | 0.354 | ||
| No | 118 | 46.2 | ||
| Yes | 131 | 51.4 | ||
| >30g/day Male or 20g/day Female | 6 | 2.4 | ||
| Anxiety/ Depression | 0.095 | 0.264 | ||
| No | 119 | 46.7 | ||
| Moderate | 115 | 45.1 | ||
| Extreme | 21 | 8.2 | ||
| Living alone | 27 | 10.6 | 0.513 | 0.095 |
| Dyslipidemia | 0.001 | 0.384 | ||
| Yes | 60.4 | 0.038 (LDL-C) | ||
| Total cholesterol >190 mg/dl | 97 | 38.0 | ||
| LDL-C (Very high-risk:>70 mg/dl; High-risk:>100 mg/dl; Low to moderate risk:>115 mg/dl) | 67 | 26.3 | ||
| HDL-C <40 mg/dl for M/ <46 mg/dl for F | 44 | 17.3 | ||
| Triglycerides >150 mg/dl) | 59 | 23.1 | ||
| Obesity | 0.001 | 0.369 | ||
| Overweight BMI≥25 kg/m2 | 137 | 53.7 | ||
| Obesity BMI≥30 kg/m2 | 43 | 16.9 | ||
| Waist circ.>94 cm M/>80 cm F | 163 | 63.9 | ||
| Waist circ.>102 cm M/>88 cm F | 102 | 40.0 | ||
| Hypertension | 0.001 | 0.010 | ||
| Yes | 106 | 41.6 | ||
| High normal | 49 | 19.2 | ||
| Grade 1 hypertension | 34 | 13.3 | ||
| Grade 2 hypertension | 13 | 5.1 | ||
| Grade 3 hypertension | 1 | 0.4 | ||
| Isolated systolic hypertension | 9 | 3.5 | ||
| Fasting glucose levels | 0.029 | 0.066 | ||
| 102-125 mg/dL | 55 | 21.6 | ||
| ≥ 126mg/dL | 1 | 0.4 | ||
*Chi-square and Kruskal-Wallis for categorical variables and t-test and ANOVA for continuous variables
The results of the SCORE CVD risk evaluation are presented in the diagram in Figure 2. Of the 52.9% (n=135) participants eligible for the relative risk SCORE charts, 92.6% (n=125) presented major modifiable CVD risk factors, and 7.2% (n=9) had no assigned physician. The mean number of risk factors in this group was 2.7; 11.2% (n=14) showed abnormal fasting glucose levels, 28.8% (n=36) were hypertensive, 34.4% (n=43) were smokers, 51.2% (n=64) presented with dyslipidemia, 41.6% (n=52) had an abnormal waist circumference, 16.8% (n=21) were obese, and 64.0% (n=80) were sedentary.
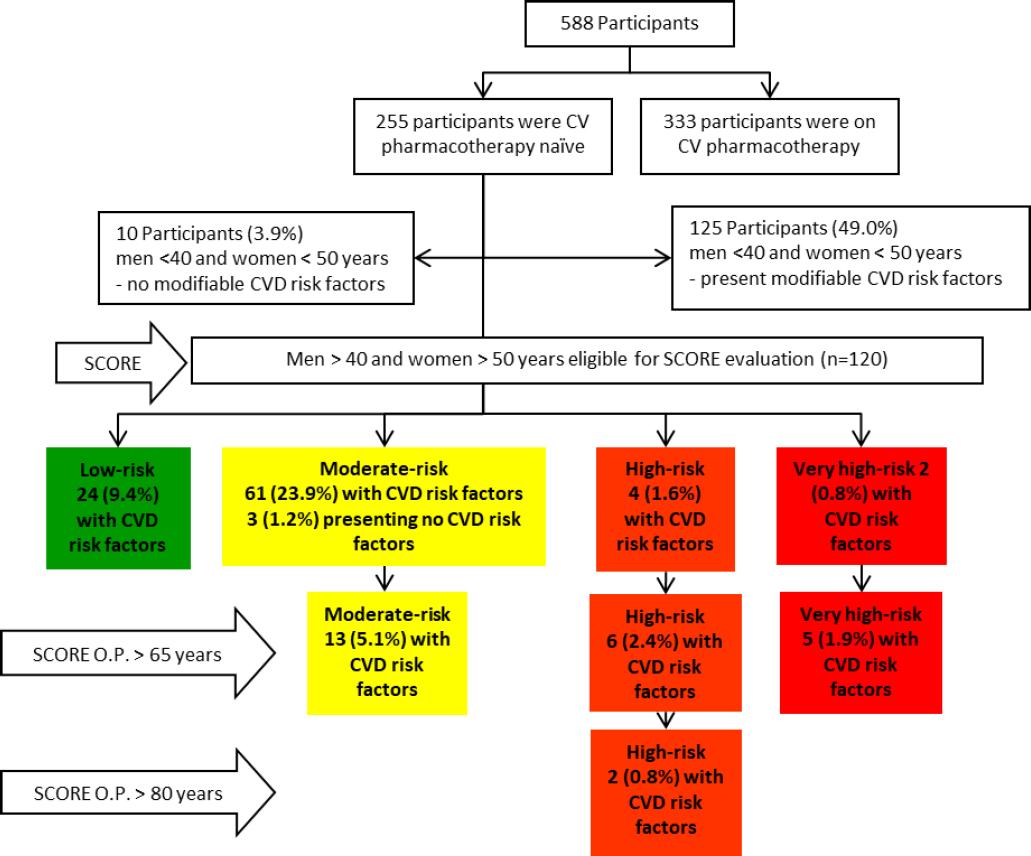
Applying the relative risk SCORE chart, 52 participants obtained a SCORE=0, 45 participants a SCORE=1, 23 participants a SCORE=2, 4 participants a SCORE=3, and 1 male participant, with no assigned physician, reached a SCORE=6, a high-risk status.
Of the 120 participants who were eligible for the SCORE assessment, the majority (64.2%, n=77) were found to be at moderate risk for CVD.
With regard to the non-modifiable CVD risk factors, 16.5% (n=42) were female ≥65 and male ≥55 years, 29.8% (n=76) were male, and 14.5% (n=37) reported a family history of premature CVD events. The participants who reported a family history of premature CVD events were taking no CV pharmacotherapy despite 94.6% (n=35) of them presenting at least one CVD risk factor, with a mean of 2.1 CVD risk factors.
In the SCORE group, we tested the associations between the four CVD risk SCORE categories (low, moderate, high, and very high risk) and the modifiable CVD risk factors (smoking, dyslipidemia, obesity, hypertension, sedentary behavior, etc.). In the non-SCORE group, we tested the associations between the number of CVD risk factors (zero to five) and modifiable CVD risk factors. The Kruskal-Wallis H test showed a significant difference in sex (chi-square(3)=9.520, p=0.023), age (chi-square(3)=35.914, p=0.001) and hypertension (chi-square(3)=11.331, p=0.010) between the different CVD risk SCORE categories. Significant differences were also found in professional situation (chi-square(3)=12.849, p=0.005), number of hospitalizations (chi-square(3)=9.285, p=0.026) and pharmacy visits (chi-square(3)=12.203, p=0.007). In the group where the SCORE charts were not applicable and we considered the number of CVD risk factors to convey the individual burden of CVD risk, the Kruskal-Wallis H test showed a significant difference in smoking habits (chi-square(5)=36.119, p=0.001), sedentary behavior (chi-square(5)=33.285, p=0.001), hypertension (chi-square(5)=23.003, p=0.001), dyslipidemia (chi-square(5)=33.175, p=0.001) and obesity (chi-square(5)=48.957, p=0.001) between the different CVD risk factor groups.
DISCUSSION
We have ascertained that pharmacies are a health care setting with a high number of users who visit pharmacies approximately four times more often than their physician and that visitors present a wide range of ages and reasons for visiting pharmacies; thus, many opportunities exist for public health initiatives to be provided in community pharmacies.37-39
Community pharmacy-based services are accepted by the users due to the perceived potential benefits (personal convenience; easy access; extended opening hours; pharmacy location; preference for the pharmacy environment; no need for an appointment), high levels of satisfaction, positive evaluation and strong positive attitude.33,38,40 Additionally, services valued by citizens include point-of-care testing.42 The obtained participation rate in this study indicates good acceptability of pharmacy customers towards CVD screening by the pharmacist. Our results are also consistent with other studies, where respondents who were frequent pharmacy customers and those who used medicines regularly were more willing to agree to participate.43 Another important facilitator of public health service acceptability is the trusting relationship between regular customers and the pharmacist which is valued mainly by older participants.29,44,45
The analysis of the reasons for nonattendance provides hints of the existing barriers, allowing pharmacists to promote pharmacy public health services by targeting relevant populations and maximizing uptake.40,41,46 The barriers to service utilization are the perception of both the general public and other health providers towards pharmacists' competencies, privacy and confidentiality, high dispensing workload, inadequate financial support, frequent staff changes, and the perception of pharmacists as medicine suppliers.46-48 Pharmacy CVD screening users agreed that a pharmacy was a good place for screening, and fewer agreed that screening should be only conducted by doctors compared with nonusers.49
We found that the most prevalent reason for nonattendance was not needing a follow-up at the pharmacy or already having routine follow-up visits to the physician, (42.7%, n=205), which was an anticipated reason for not needing a screening service in the pharmacy. The pharmacy has long opening hours, allowing the participants to choose when to undergo the CVD risk assessment. Even so, lack of time was one of the reasons for nonattendance. Another reason for nonattendance was the location not being the usual pharmacy, the customer being a migrant or lack of transport to access the pharmacy in 17.3% (n=83) of the contacted customers. The lack of public means of transportation in many locations in Portugal is a reality, but this reason would be circumvented if the CVD risk assessment service was provided in all pharmacies, which have wide geographic coverage. Including pharmacists in domiciliary hospitalization units leads to increased patient safety.50 Thus, if community pharmacists evaluate the risk of their users in institutions and homes, this further reason for nonattendance would be circumvented.
Public cognizance, awareness and previous use of pharmacy services facilitate the receptivity of the services.37 Not being accustomed to participating in this type of service was the reason noted by 9.6% (n=46) of the customers, and 6.3% (n=39) agreed to participate only after an explanation given by the pharmacist, confirming the former statement.
The prevalence of CVD risk factors, such as dyslipidemia, hypertension, overweight and sedentary lifestyle, is very high, and obesity, smoking, and abnormal fasting glucose levels are concerning prevalent. In women <50 years, the absolute SCORE risk is zero even when presenting multiple risk factors. Thus, the relative risk chart is valuable for illustrating how a young person with a low absolute risk may be at a substantially high and reducible relative risk and that individual CVD risk factors must be addressed to manage these at-risk patients.
We found high-risk and very-high-risk SCORE statuses that corroborate the high mortality rates of CVD due to the high prevalence of risk factors. Our results were very similar to those found in a study conducted in Portuguese pharmacies where approximately 20% of the studied adults were at high risk and the main CV risk factors were hypertension (54.8%), hypercholesterolemia (63.1%), diabetes (13.4%), smoking (10.4%), obesity (29.0%) and a family history of premature CVD (33.0%).51 Our results demonstrate that community pharmacies can be a valuable and feasible venue for screening the population for patients at risk for CVD. Our results were also very similar to those found in the most recent study conducted in the Portuguese population where unhealthy diet (71.3%), overweight/obesity (62.1%), hypertension (43.1%), sedentarism (29.2%), smokers (25.4%), dyslipidemia (51.5%), and family history of premature CVD (11.8%) were found as risk factors. That study found that 68% of the participants presented two or more CVD risk factors.33 However, the referred study included diagnosed patients already on CV pharmacotherapy.
As expected, the Kruskal-Wallis H test showed a significant difference in sex, age, and hypertension between the different CVD risk SCORE categories, as these are the variables included in the SCORE algorithm and the major determinants of CV risk. The Kruskal-Wallis H test results also corroborate the assumption that the presence of an individual CVD risk factor predicts the clustering of CVD risk factors, rendering the screening process even more effective.
Thus, the data suggest that it would be feasible to provide CV risk screening in Portuguese community pharmacies.
Strengths and weaknesses
This cross-sectional study can be used to assess the burden of CVD and the health needs of the Portuguese population, and it disclosed findings that can be useful to planning and allocating CVD screening services in community pharmacies. However, a follow-up study to determine the health outcomes after the pharmacist's interventions on at-risk patients would have enriched the study. Future research is needed to describe clinical improvements in enrolled patients. Investigating the perceptions of primary care physicians regarding such a program and the response and collaboration regarding pharmacists referring patients is also important. Additionally, it would be important to gauge the acceptability by pharmacists in community pharmacies and to understand their willingness to provide CVD risk screening services.
Some data were self-reported and retrospective, with the risk of recall bias, as community pharmacists do not have access to the clinical information of the patients. We adopted a total population sampling approach; nevertheless, health check-ups are inequitably taken up, and non-attendees may present an even greater clinical need or risk factor burden.31 On the other hand, we might have captured patients who do not visit their physician or were not included in routine health examinations.
Some customers claimed "lack of time" as a reason for nonattendance, and this is a type of sampling bias. Thus, we may assume that some members of our population were inadequately represented in the sample. In summary, if we screened the non-attendees, the results of the study could have been different. To minimize nonresponse bias, the day before the encounter, the pharmacist made a second phone call to remind the participants.
The screening service was free of charge, positively influencing acceptability. Thus, the achievement of similar acceptability rates would depend on remuneration. The existing trusting relationship between regular customers and the pharmacist also had a positive influence on the acceptability rate but ended up mirroring a real-life context.
The study was conducted in a single pharmacy but would have been enriched by a multicenter study. Evaluating whether community pharmacists can include CVD screening services along with their regular daily practices would also be beneficial. However, the CV risk assessment strategy would be a combination of two basic services already supported by law, point-of-care testing and health screening, to be implemented as a standardized pharmacy-based CVD risk assessment service, which pharmacists have already included in their daily routine.
CONCLUSIONS
We determined the feasibility of pharmacist-delivered CVD risk screening in Portuguese community pharmacies. We assessed the characteristics of pharmacy customers, found high customer acceptability, asked for the reasons for nonattendance, and found a high prevalence of patients at risk for CVD. This is an opportunity for Portuguese community pharmacists to take a leading role in the early detection of CVD.

