










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Andaluza de Medicina del Deporte
versión On-line ISSN 2172-5063versión impresa ISSN 1888-7546
Rev Andal Med Deporte vol.6 no.1 Sevilla mar. 2013
Analysis of the drinks that contribute to the hydration of andalusian sportspeople
Análisis de bebidas que contribuyen a la hidratación de deportistas andaluces
A. Palacín-Arcea, M. Mariscal-Arcasa,c, C. Monteagudoa, M.C. Fernández de Alba-Sánchezb, J.R. Gómez-Puertob, C. Ruiz-Verdejab, J.D. Beas-Jiménezb and F. Olea-Serranoa
aResearch Group on Nutrition. Diet and Risk Assessment-AGR255. Nutrition and Food Science Department. University of Granada. Granada. Spain
bAndalusian Centre of Sport Medicine (CAMD). Junta de Andalucía. Spain
cFood Technology Department. Nutrition and Food Science. University of Murcia. Murcia. Spain
The study was supported by the Junta de Andalucía, Spain (Research Group AGR-255 "Nutrition. Diet and Risk Assessment"), a collaboration agreement with the Andalusian Centers of Sports Medicine (Junta de Andalucía) and the FPU program of the Spanish Ministry of Education and Science.
ABSTRACT
Objectives. To estimate the water balance in a healthy population of sportspeople from Southern Spain and determine the sources of their fluid intake, evaluating the contribution of different types of drink and comparing the results by sex and province of residence.
Methods. Three hundred eighty-six sportspeople (231 males, 152 females) were enrolled in the study. A questionnaire was administered to calculate nutrient intake through diet and physical activity, and anthropometric measures were taken according to ISAK standards. SPSS-15 was used for data analyses.
Results. Fruit juice, tap water, bottled water, processed fruit juice, carbonated drinks, and isotonic drinks comprised 96% of the total water intake. Simple sugar consumption represented 4.44% of daily calorie intake. Significant differences were found between sexes and between professionals and amateurs. The amount of drinks consumed varied as a function of the quality of the drinking water, which significantly differed among the eight Andalusian provinces.
Conclusion. This study population did not fully meet fluid intake recommendations, compliance with hydration recommendations varied as a function of the sex and the amateur or professional status of these sportspeople. The pattern of drinks consumption also differed according to their place of residence.
Palabras clave: Sportspeople. Hydration. Diet.
RESUMEN
Objetivos. Estimar el balance hídrico en deportistas sanos del sur de España. Determinar los principales aportes de agua y la contribución de los diferentes tipos de bebidas en la hidratación de los sujetos de estudio y comparar los resultados teniendo en cuenta el sexo y la provincia de residencia.
Métodos. Se reclutaron 386 individuos, (231 hombres y 152 mujeres), a través de los Centros Andaluces de Medicina del Deporte (CAMD) y el CAR de Sierra Nevada. Mediante la realización de un cuestionario se calculó la ingesta de nutrientes a través de la dieta y la actividad física. Así mismo se tomaron medidas antropométricas de acuerdo con las normas ISAK. Los datos fueron procesados usando SPSS-15.
Resultados. Los zumos naturales, el agua del grifo, el agua embotellada, los zumos envasados, las bebidas carbonatadas y las bebidas isotónicas contribuyen en un 96% a la ingesta total de agua. La media de consumo diario de azúcares simples fue del 4,44% de la energía diaria. Existen diferencias estadísticamente significativas entre sexos y entre profesionales y aficionados. Teniendo en cuenta la calidad del agua de consumo de las ocho provincias andaluzas encontramos diferencias en el patrón de ingesta de líquidos.
Conclusión. En este estudio la población no cumple las recomendaciones de ingesta de líquidos. Las recomendaciones de hidratación varían en función del sexo y de si son o no profesionales o aficionados. El patrón de ingesta de líquidos es diferente dependiendo del lugar de residencia de nuestros deportistas.
Key words: Deportistas. Hidratación. Dieta.
Introduction
Water is a non-caloric nutrient that is essential for life and has numerous functions as a solvent, transporter, body temperature regulator, and lubricant, among others. It makes up around 60-70% of the human organism by weight, and fluid intake is responsible for 60% of this amount, food intake for 30%, and cell metabolism for the remaining 10%1-4.
A close balance is necessary between water intake (drink and food) and excretion (sweat, urine, feces, respiration)5. The WHO (1996) recommends an intake of 30 mL/Kg/day for a healthy person, who is only considered at risk if there is a water loss >10% body weight6. In any physical activity, the heat released in muscle contraction must be eliminated through perspiration, producing electrolyte and water losses, which are greater in more intense and prolonged exercise. Dehydration has a negative effect on the health and physical performance of sportspeople, reducing their capacity to exert high-intensity efforts7-11.
Loss of 2-5% bodyweight through dehydration is considered to reduce the capacity for aerobic effort by 20-30%12. Sweat loss during intense exercise ranges from around 0.5 to 2.0 L/h, depending on the ambient temperature, body size, and metabolic rhythm13,14.
The consumption of carbohydrate solutions may enhance sports performance by ensuring a sufficient amount of fuel for energy needs and by supplying fluids for rehydration15. An adequate carbohydrate intake is essential to maintain the energy levels of sportspeople. In general, carbohydrate solutions leave the stomach slower than water or weak sodium chloride solutions16-20. Sugar-rich solutions remain longer in the stomach than do water or weaker sugar solutions but deliver more glucose (in Kcal) per minute to the intestine21.
Some authors have argued that a sports drink should contain less than 2.5 g sugar per 100 mL of water in order to accelerate its passage through the stomach, but this small amount of carbohydrates would not make a sufficient contribution to energy reserves. Recent studies claimed that sportspeople need to consume at least 50 g sugar an hour in order to improve their performance, whereas most commercially available sports drinks contain only 6-8 g sugar per 100 mL22,23. Glucose is an essential component of a rehydrating drink because it not only provides a source of energy but also stimulates sodium absorption to replace the sodium lost by perspiration and promotes water absorption by the glucose-sodium co-transport mechanism24-26. Ideally, water and electrolytes should be replaced as fast as they are lost, thereby minimizing the risk of dehydration, increased body temperature, cardiovascular stress, and hyponatremia27.
Given the importance of good hydration to sportspeople, whose achievements can be impaired by a water balance deficit, we designed a study to gather data on their current situation to serve as a reference for sports activity by present and future sportspeople. The study objectives were: to estimate the water balance in a healthy population of sports-people from the Andalusia region (Southern Spain); to determine the sources of their fluid intake, evaluating the contribution of different types of drink; and to compare results by sex and by province of residence.
Method
Subjects
The eligible population was composed of sportspeople affiliated to one of the eight Andalusian Sports Medicine Centers in Andalusia or the High Altitude Training Center in Granada, Southern Spain. This study was approved by the ethics committee of our university. The inclusion criteria were: age between 18 and 55 yrs, because of the distinct water needs of individuals below and above this range28; and the absence of disease.
A total of 386 volunteers were recruited at the above centers and invited to an initial interview with the person responsible for healthcare at each center, who had received training for this purpose and followed an agreed protocol. After their informed consent had been obtained, the volunteers completed a personal data form, food frequency questionnaire (FFQ), 3 × 24-h food intake recall, questionnaire on life habits, and 24-h recall of physical activity. They then underwent an anthropometric study (see details below).
Participants were identified by an alphanumeric code to preserve their anonymity. The socio-demographic data included province, sex, marital status, educational level, profession, place of work, sports practiced, sports level, and period of the season. The FFQ used has been widely used and validated29,30; it includes foods consumed by Mediterranean populations and gathers information on intake at breakfast, mid-morning snack, lunch, afternoon snack, and evening meal. The questionnaire records: the consumption or not of each food item; the number of times items were consumed per day, week, or month during the previous year; and the amount consumed each time in g, mL, or domestic measures (plates, glasses, spoons, etc.). The 3 × 24-h recall was an open-format questionnaire that gathered information on the food intake during the three previous days (including 1 non-working day and 2 working days); data obtained were analyzed using Dial Diet 1.19. 2008 software (Alce Ingeniería, Madrid, Spain).
The physical activity recall was an open-format questionnaire on the type of exercise or sports modality, level of competition (national, regional, other), exercise intensity, mean duration of each exercise session, place and climatic conditions, period of the season (pre-competition, competition, recovery/transition period), and other sports activities31.
The anthropometric characteristics gathered were weight, height, BMI, sitting height, arm span, fold profile, body composition, perimeters, diameters, and bioimpedance, all according to the ISAK rules32 and using a Holtain Tanner/Whitehouse Skinfold Caliper (Holtain Ltd, Crymych, UK); Rosscraft tape measure (Rosscraft Division of Batchelor's Datamedia Limited, Canada); Seca 220 scales and stadiometer (Seca Mexico, México, D.F.), and PROMIS body-composition apparatus (Professional Medical Information System, S.L. Puerto de Santa María, Spain).
The recommended fluid intake was considered to be 1 L of fluid per 1,000 Kcal consumed33. Sweat losses were calculated as 500 mL/m2/h of intense activity, as proposed by Rowland (2011)34. The recommended intake of simple sugars was defined as no more than 10% of daily energy intake, as proposed by the WHO and FAO (Geneva/Rome, March 3 2003).
SPSS-15 (SPSS Inc. Chicago, IL, USA) was used for the statistical analyses. The Student's t-test for independent samples, ANOVA test, linear regression, and stepwise regression were used (see Results and tables). P < 0.05 was considered significant in all analyses.
Results
A total of 386 individuals were enrolled in the study, 231 males (60.31%) and 152 females 39.68% (n = 152), a significant gender difference (c2=16.29; p = 0.001). The age ranged from 18 to 54 yrs, with a mean of 27.39 yrs (Standard Deviation [SD] = 0.48). All participants were healthy active sportspeople.
Table 1 shows the mean anthropometric characteristics of the study population by sex (Student's t-test for independent variables); 54% of all participants practiced sport professionally and 46% were amateurs. Among the males, 48.9% were professionals and 51.1% amateurs; among the females, 61.8% were professionals and 38.2% amateurs, a significant difference between the sexes (p = 0.013). The mean hours of intense exercise/day were 3.02 for the males versus 2.43 for the females (p < 0.05), while the mean body surface area was 1.93 m2 in the males versus 1.68 m2 in the females (p < 0.05). Mean sweat loss during exercise was 783.15 mL/h in the males versus 647.15 mL/h in the females (p < 0.01). The mean water requirement without considering sweat loss was 2885.16 mL for males and 2430.07 mL for females (p < 0.05). When sweat loss was taken into consideration, the water requirement was 3294.13 mL for males and 2728.23 mL for females (p < 0.05).

According to the stepwise regression analysis, the water intake was supplied (in order of importance) by dairy products or derivatives (71%), drinks (16.4%), fruit, vegetables, and fish or derivatives, together representing > 90% of total intake (table 2). The drinks were (in order of importance) fresh fruit juice, tap water, bottled water, processed fruit juice, carbonated drinks, and isotonic drinks, together comprising 96% of the total. Consumption of the first three items represented 83.1% of total drink intake; isotonic drinks contributed 3% of the daily total (table 2).

The mean daily consumption of simple sugar by the participants was 25.18 g/day, which provides approximately 100.71 Kcal/day, i.e., 4.44% of daily calorie intake (SD = 7.72 p < 0.001). Drinks supplied 22.14 g/day of this sugar. The drinks with the highest percentages of sugar were fruit juice (bottle/pack) (50.8%), carbonated drinks (16.4%), and energy drinks (15.7%), according to the FFQ questionnaire and 3 × 24h recall results (table 2).
Table 3 exhibits the results as a function of the professional or amateur status of the sportspeople, analyzed by using Student's t-test for independent samples. Significant differences (p < 0.05) were found between professionals and amateurs in Kcal/day, recommended fluid in-take, water supply via drinks, and balance between fluid consumption and loss.
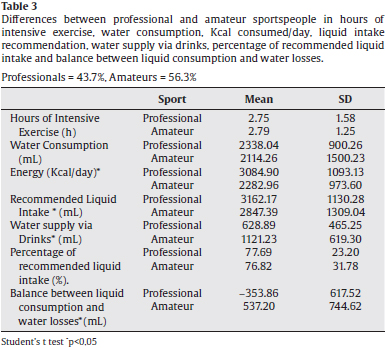
Table 4 shows the results of linear regression analysis with BMI as dependent variable and age, hours of intense exercise, water consumption, water provided by drinks, water intake recommendation, percentage of recommended water intake, and balance between drink consumption and water loss as independent variables. A fit of R = 0.687 was obtained, and significant differences were found as a function of BMI in hours of intense exercise, drink consumption, water losses, water supplied by drinks, and hours of intense exercise (p < 0.05).

Table 5 shows the ANOVA results for BMI, BMI/fat weight ratio, and BMI/muscle weight ratio, considering four groups (males and females under 30 yrs old and males and females over 30 yrs old). Significant differences among the groups were observed in BMI (p = 0.048) and BMI/ fat weight ratio (p = 0.005).

Table 6 exhibits ANOVA results for the amount of drinks consumed as a function of the quality of the drinking water, which significantly varied (p < 0.001) among the eight Andalusian provinces as follows: soft water 50 mg/L (Córdoba and Málaga), slightly hard water 50-100 mg/L (Sevilla, Huelva, Jaén, Granada, and Cádiz), and moderately hard water 100-200 mg/L (Almeria), according to data published by OCU, the Spanish Organization of Consumers and Users (www.ocu.org).

Discussion
In this study, we estimated the fluid intake of Andalusian sportspeople aged 18-55 year. The fluid intake was 77.69% of the recommended level (WHO, 1996) in the professionals and 76.82% of this level in the amateurs, a non-significant difference. The Directorate - General for Health and Consumer Protection of the European Commission produced a report (February 2001) on the composition of foods and drinks designed to cover the energetic cost of major muscular efforts, especially in sportspeople. It indicates that sports drinks should supply carbohydrates as the main energy source and effectively maintain optimal hydration or rehydration35. In the present series, the drinks making the largest contribution to their hydration were natural fruit juice, bottled water, and processed juice, which comprised 88% of the total intake. Similar results were reported by Brazilian university sportspeople by Martins and Ferreira36. ALM de Francisco A, et al37 found that an increase in physical activity produced a rise in fluid intake, although they considered the consumption of juices and soft drinks together, unlike in the present study. The intake of isotonic drinks in our study population was very low (3%) and can be considered inadequate, given that they contain 6-7% carbohydrates and help to replace the electrolytes lost in intense exercise38.
A study in Mexico39 reported that drinks represented up to 22.3% of the total daily energy supply of adolescents and adults, whereas drinks contributed 4.44% of the daily energy intake in the present study population, significantly (p < 0.001) below the maximum of 10% recommended by the WHO and FAO (Geneva/Rome, March 3 2003).
BMI is a useful parameter to assess nutritional status in healthy individuals with a moderate physical activity routine; however, it may not be a reliable measure in sportspeople and has been reported to vary according to the characteristics of the individuals and of the sports they engage in40. For this reason, we analyzed the BMI divided by the muscle weight and the BMI divided by the fat weight. Differences in BMI and BMI: fat weight ratio (p ≤ 0.005) were found as a function of the sex of the sportspeople and their age (≤ 30 yrs vs. 30 yrs). The evaluation of anthropometric findings in studies on the nutritional status of sports-people requires comparisons with reference values established in populations of high-level practitioners of the same types of sports41.
Significant inter-provincial differences were observed in the consumption of drinks (p < 0.001). Individuals living in areas with soft or only moderately hard drinking water consumed a larger volume of drinks (carbonated drinks, energy drinks, bottled water, etc.) in comparison to those residing in areas characterized by hard tap water.
In conclusion, compliance with hydration recommendations varied as a function of the sex and the amateur or professional status of these sportspeople. The pattern of drinks consumption also differed according to their place of residence. This study population did not fully meet fluid intake recommendations, but their consumption of simple sugar was well below the WHO-recommended maximum (<10%). The BMI is not a reliable indicator of the weight status of sportspeople due to their higher proportion of muscle weight.
Acknowledgements
The authors are grateful to the High Performance Center of Sierra Nevada and the Sports Medicine Centers of Andalusia in Huelva, Málaga, Almería and Granada for their collaboration in this study and thank Richard Davies for his assistance with the English version. Study participants were recruited through the project "Nutritional and diet assessment methodologies applied to the Andalusian sportsperson in Andalusian Sports centers", Research project FMD2010SC0071 of the Junta de Andalucía.
Conflict of interest
The authors declare that they have no conflict of interest.
References
1. Martínez Álvarez JR, Villarino Marín AL, Polanco Allué I, Iglesias Rosado C, Gil Gregorio P, Ramos Cordero P, et al. Spanish guidelines for hydration. Nutr clín diet hosp. 2008;28. [ Links ]
2. Laaksonen DE, Nuutinen J, Lahtinen T, Rissanen A, Niskanen LK. Changes in abdominal subcutaneous fat water content with rapid weight loss and long- term weight maintenance in abdominally obese men and women. International Journal of Obesity. 2003;27:677-83. [ Links ]
3. Sawka Michael N, Mountain Scott J. Fluid and electrolyte supplementation for exercise heat stress. American Journal of Clinical Nutrition. 2000;72 (2):564S-72S. [ Links ]
4. Murray B. El reemplazo de fluidos: posición del colegio americano de medicina del deporte. Sports Science Exchange. 1996;9(4):1-10. [ Links ]
5. Iglesias Rosado C, Villarino Marín AL, Martínez JA, Cabrerizo L, Gargallo M, Lorenzo H, et al. Importancia del agua en la hidratación de la población española: documento FESNAD 2010. Nutr Hosp. 2011;26(1):27-36. [ Links ]
6. Palacios Gil-Antuñano N, Montalvo Zenarruzabeitia Z, Ribas Camacho AM. Alimentación, nutrición e hidratación en el deporte. 2009. [ Links ]
7. Judelson DA, Maresh CM, Anderson JM, Armstrong LE, Casa DJ, Kraemer WJ, et al. Hydration and muscular performan Does fluid balance affect strength, power and high-intensity endurance? Sports Med. 2007;37(10): 907-21. [ Links ]
8. Claremont AD, Costill DL, Fink W, VanHandel P. Heat tolerance following diuretic-induced dehydration. Medicine and Science in Sports and Exercise. 1976;8:239-43. [ Links ]
9. Boguslaw W, Brian WT, Oded Bar-Or. Voluntary fluid intake, hydration status, and aerobic performance of adolescent athletes in the heat. Applied Physiology Nutrition and Metabolism. 2010;35,834-41. [ Links ]
10. Cheuvront SN, Carter R, Sawka MN. Fluid balance and endurance exercise performance. Curr Sports Med Rep. 2003;2(4):202-8. [ Links ]
11. Paquot N. Sports nutrition. Rev Med Liege. 2001;56(4):200-3. [ Links ]
12. Da Silva AI, Fernandes LC, Fernández R. Time motion analysis of football (soccer) referees during official matches in relation to the type of fluid consumed. Braz J Med Biol Res. 2011;44(8):801-9. [ Links ]
13. Casa Douglas J, Ganio Matthew S, López RM, McDermott Brendon P, Armstrong Lawrence E, Maresh Carl M. Intravenous versus Oral Rehydration: Physiological, Performance, and Legal Considerations. Current Sports Medicine Reports. 2008. [ Links ]
14. Wilmore JH, Costill DL, Kenney L. Physiology of sport and exercise. 4th ed. Champaign IL: Human Kinetics Publishers; 2007. [ Links ]
15. Spanish Federation of Sport Medicine (SFSM). Consensus on drinks for the sportsman. Composition of guidelines of replacement of liquids. Consensus document of the Spanish Federation of Sports Medicine. Archivos de Medicina del Deporte. 2008;25(4):245-58. [ Links ]
16. Miller KC, Mack GW, Knight KL. Gastric emptying after pickle-juice ingestion in rested, euhydrated humans. J Athl Train. 2010;45(6):601-8. [ Links ]
17. Marshall HC, Ferguson RA, Nimmo MA. Human resting extracellular heat shock protein 72 concentration decreases during the initial adaptation to exercise in a hot, humid environment. Cell Stress Chaperones. 2006;11(2): 129-34. [ Links ]
18. Moran TH, Knipp S, Schwartz GJ. Gastric and duodenal features of meals mediate controls of liquid gastric emptying during fill in rhesus monkeys. AJP - Regu Physiol. 1999. [ Links ]
19. Costill DL, Saltin B. Factors limiting gastric emptying during rest and exercise. Journal of Applied Physiology. 1974;37:679-83. [ Links ]
20. Coyle EF, Costill DL, Fink WJ, Hoopes DG. Gastric emptying rates for selected athletic drinks. Res Q. 1978;49:119-24. [ Links ]
21. Casa DJ, Armstrong LE, Hillman SK, Montain SJ, Reiff RV, Rich Brent SE, et al. National Athletic Trainers Association Position Statement: Fluid Replacement for Athletes. Journal of Athletic Training. 2000;35(2):212-24. [ Links ]
22. Von Duvillard SP, Braun WA, Markofski M, Beneke R, Leithäuser R. Fluids and hydration in prolonged endurance performance. Nutrition. 2004;20 (7-8):651-6. [ Links ]
23. American College of Sports Medicine; American Dietetic Association; Dietitians of Canada. Joint Position Statement: nutrition and athletic performance. Med Sci Sports Exerc. 2000;32(12):2130-45. [ Links ]
24. Cheuvront SN, Haymes EM. Thermoregulation and marathon running: biological and environmental influences. Sports Med. 2001;31(10):743-62. [ Links ]
25. Nelson Paul B. Hyponatremia in a Marathoner. Physician and Sportsmedicine. 1988. [ Links ]
26. Pugh LG, Corbett JL, Johnson RH. Rectal temperatures, weight losses, and sweat rates in marathon running. J Appl Physiol. 1967;23(3):347-52. [ Links ]
27. Scientific Committee on Food. Report of the Scientific Committee on Food on composition and specification of food intended to meet the expenditure of intense muscular effort, especially for sportsmen. Health & Consumer Protection Directorate-General. European Commission. 2001. [ Links ]
28. European Commission. EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for water. EFSA Journal. 2010;8(3):1459. [ Links ]
29. Mariscal-Arcas M, Romaguera D, Rivas A, Feriche B, Pons A, Tur JA, et al. Diet quality of young people in southern Spain evaluated by a Mediterranean adaptation of the Diet Quality Index-International (DQI-I). British Journal of Nutrition. 2007;98(6):1267-73. [ Links ]
30. Rivas A, Cerrillo I, Granada A, Mariscal-Arcas M, Olea-Serrano F. Pesticide exposure of two age groups of women and its relationship with their diet. Science of the Total Environment. 2007;382(1):14-21. [ Links ]
31. Hernández B, Gortmaker SL, Laird NM, Colditz GA, Parra-Cabrera S, Peterson KE. Validez y reproducibilidad de un cuestionario de actividad e inactividad física para escolares de la ciudad de México. Salud pública Méx. 2000. [ Links ]
32. Group of kinanthropometry of Spanish Federation of Sports Medicine (SFSM). Body composition assessment in sports medicine. Statement of Spanish. Archivos de Medicina del Deporte. 2009;26:166-79. [ Links ]
33. National Research Council (U. S.). Subcommittee on the Tenth Edition of the RDAs. Subcommittee on the Tenth Edition of the RDAs, Food and Nutrition Board, Commission on Life Sciences, National Research Council. 10a ed. Washington: National Academy Press. 1989. [ Links ]
34. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-88. [ Links ]
35. Report of the Scientific Committee on Food oncomposition and specification of food intendedto meet the expenditure of intense musculareffort, especially for sportsmen. Available from: http://europa.eu.int/comm/food/fs/sc/scf/out64_en.pdf. [ Links ]
36. Martins JCB, Ferreira FG. Nivel de conocimiento de deportistas universitarios de la UFV sobre el tema hidratación. Fitness & Performance Journal. 2005. [ Links ]
37. De Francisco ALM, Martínez Castelao A. Estudio Bahía 2008: barómetro de la hidratación de la población española. Revista Nefrologia. 2010;30(2):220-6. [ Links ]
38. Cuasapaz López WA, Catagua Coral LP. La hidratación en los deportistas seleccionados de la disciplina de fútbol en los colegios de la ciudad de San Gabriel. Universidad Técnica del Norte. Facultad de Educación, Ciencia y Tecnología. Ibarra, 2010. [ Links ]
39. Barquera S, Hernández Barrera L, Tolentino ML, Espinosa J, Nq SW, Rivera JA, et al. Energy intake from beverages is increasing among Mexican adolescents and adults. J Nutr. 2008;138:2454-61. [ Links ]
40. Garrido Chamorro RP, Félix Garnés RA, González Lorenzo M. Índice de masa corporal y porcentaje de grasa: un parámetro poco útil para valorar a deportistas. Buenos Aires: Revista Digital; 2004. [ Links ]
41. Kweitel S. BMI: Little useful tool to determine ideal weight of a sportsman. Rev int med cienc act fís deporte. 2007. [ Links ]
![]() Correspondence:
Correspondence:
F. Olea-Serrano
Nutrition and Food Science Department. University of Granada
Campus de Cartuja s/n
18071 Granada. Spain
E-mail: folea@ugr.es
Received: May 5, 2012
Accepted: September 9, 2012

