










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkBACKGROUND
Burns is regarded as a common cause of childhood injuries and serious public health concerns worldwide [1, 2]. Some authors submitted that childhood burns account for 2-6% of all injuries in the pediatric age group in developed countries [1, 3, 4]. Burns is remarked as the second most frequently occurring accidental fatality in children under five years and the highest unintentional death at home [1, 5, 6, 7].
In the developing countries and low socioeconomic settings like ours, childhood burns deserve special attention because such injuries constitute the leading factor responsible for disability-adjusted life-years (DALYs) in low- and middle-income countries. In 2004, about 11 million people worldwide suffered from burns, severe enough to require medical attention [8]. Besides, children are a vulnerable category with attendant morbidity and mortality. Burns is a significant reason for prolonged hospital admissions, deformity, disability, and death in sub-Saharan Africa [9].
Interestingly, they may equally impact in the long-term on the patient's economic physical, psychosocial status [1, 10, 11]. Meanwhile, children who sustain burn injuries may also develop posttraumatic stress disorder [1, 10, 11]. There is currently no published work on childhood burns in our settings. Therefore, this study aimed to highlight the pattern and treatment outcome of childhood burn injuries in northwestern Cameroon. Such reports are expected to provide preventive and improvement guidelines in our settings in the long run.
METHODS
The prospective cross-sectional descriptive study was conducted over a two year study period that spanned between December 2017 and December 2019 at the Department of Surgery of St Elizabeth Catholic General Hospital, Shisong. The facility is a tertiary health facility in the Northwestern region of Cameroon, with a catchment population of about 3 million people.
We did not include children over 15 years in the study. The parents/attending adults of the involved children signed informed consent before the commencement of the study. Following the clinical diagnosis and relevant investigations, the total body surface area (TBSA) burnt was then calculated utilizing the Lund and Browder's chart. A pretested proforma was utilized for data collection per sociodemographic, etiology of burns, pre-hospital intervention, and timing of the injury. The data also include the surface area of the wounds, as well as treatment outcome [12-16]. Data analysis was achieved utilizing EPI Info 7. Data presentation as per descriptive statistics including mean, median, frequency, percentages, etc., and chi-square test where applicable, and p- value is set at 0.005.
RESULTS
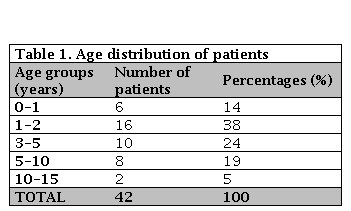
During the study period under review, there were a total of 42 patients, which consisted of 23 (54%) males and 19 (46%) females. The overall mean for the children ages was 4.84 years, with the median 2.40±3.05 years, interquartile range of 1-14 years. Most patients were from Kumbo and suburbs in 29 (70%) cases, and 13 (30%) came from other cities. The age range at risk was two years and below, constituting about 52.0% of the entire patients, as seen in Table 1.
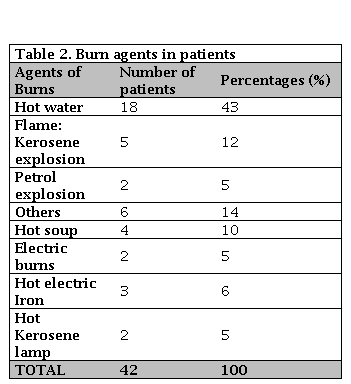
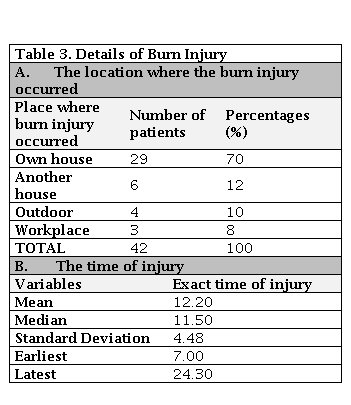
The most frequently encountered cause of burns was hot water (Scald -Burns), occurring in 18 (43%) of the patients. Four (22%) of the scald burns injuries were deliberate. In those instances, the parents dip the affected child into hot water as remedies for seizure disorders or convulsion. In the meantime, the second most frequently occurring burn injuries were flame burns, occurring in 13 (31%) of the cases; Kerosene or petrol explosion was responsible in seven cases, as seen in Table 2. The majority of burns were right at patient's homes estimated at 29 (70%) cases. Meanwhile, in 29 (70%) cases, the incident occurred outside the houses in an estimated 6 (12%) cases, as outlined in Table 3. A closer review of the timing of the events showed that the median time was 11.50, while the overall average timing was 12.20, as shown in Table 3.
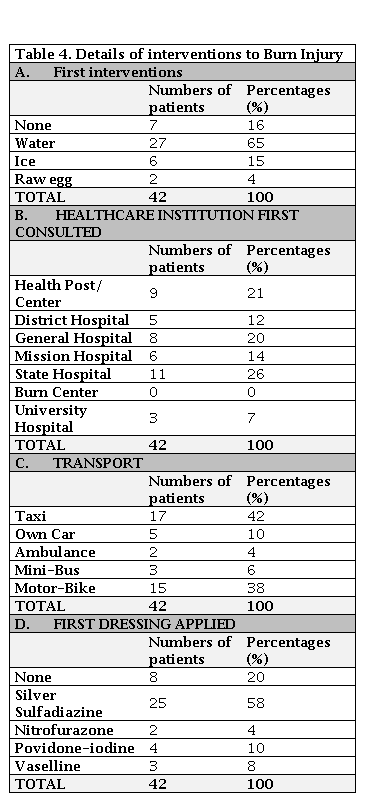
Sixty-five (65%) parents made the first intervention with water, 6 (15%) with ice, and 7 (16%) did not intervene (Table 4). After the incident, the details of initial healthcare institutions visited include 5 (12%) presented directly at the district hospital, 14 (33%) went to the university or a state hospital, and 9 (21%) visited the private healthcare center. In the Kumbo community, the most acceptable medium of transportation is by motorbike, which is reflected in Table 4 figures showing that 15 (38%) cases were transferred to the clinic by motorcycles. The family car was utilized in 5 (10%) cases, private taxi in 7 (18%) cases, and ambulance in 2 (4%) cases.
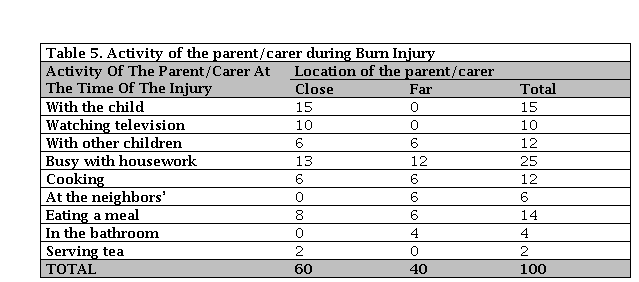
Furthermore, 25 (60%) parents were at close range, and 17 (40%) parents were far away from their children as per the time of the events. An estimated 59% of the families were categorized into low socioeconomic class. Crowded lifestyle was demonstrated in 89% of these families by the presence of only 1 or 2 rooms of living space. Most parents were occupied with various forms of housework when the incident occurred. Three (9%) were watching television, while 8 (20%) admitted to being engaged with the child as outlined in Table 5. Besides, an estimated 60% of the cases had the parents close to their children when the incidents occurred. Also, parents were rather busy with other activities in 35% of cases of burn injuries.
DISCUSION
In this series, our experience with burns injuries in children in northwestern Cameroon is similar to what obtains elsewhere. Globally, burns injuries remain a serious health concern in children [17]. We observe male children predominance in our study, which conforms to several published studies [1, 18]. Male children are relatively more active and explorative than their female counterparts yet with minimum ability to recognize hazards, which may be responsible for their more frequent involvement in burn injuries [1, 17, 18, 19, 20]. Consequentially, they demonstrate an increased risk of exposure to such accidents in general. The majority of burns occur in children within the age group 2-6 years. In a similar study by Al-Shehri, who submitted that the majority of childhood burns happen in the 0-5 year age group, which constitutes 78% of all childhood burns [1, 21]. Interestingly, Kai-Yang et al., observed that children aged < 3 years were more prone to burn injury than children aged > 3 years [1, 22].
Furthermore, the degree of burn injury has been reported to be high among younger children as children under age six years of having fragile skin compare to older children and adult”s [1, 22, 23]. The most frequently affected body parts include the limbs and the trunk, especially in children. Perineal burns are a rarity because the perineum in the pediatric age group is a protected location, as noted by Ameh [17, 24] in one literature report.
In this series as well as other reports scald burns is on the rise with an estimated 43% cases recorded here, as compared with the submission of Archibong et al., who reported other hot items like beverages, oil, and soup, in addition to water; altogether constitute 56.6% of the cases [17, 19]. Interestingly, studies by Adesunkanmi [17, 25] in the southwestern region and Uba et al. [17, 26] in the northern province of Nigeria corroborated our findings of scald burns as the most frequently occurring. Our results are in sharp contrast to other works of literature reports suggesting flame burns as the most commonly encountered. However, these conflicting reports studied adults and children combined [17, 27, 28]. There were no cases of child abuse in our series, as have been reported in some studies [17, 29, 30].
Also, surprising is that most burn injuries occurred at home within the presence of competent adults; who were pre-occupied with other activities at the time of accidents. Besides, they were distracted and paying less attention to the children. Datubo-Brown argued that most of these cases were preventable, provided the adults paid closer attention to identifying the potential hazards [17, 29].
Surprisingly, applications of harmful substances as the first aids in childhood burns are still prevalent in our environment. For instance, the use of raw eggs and traditional medicine may encourage wound infection, as seen in a few of the cases [17, 31, 32, 33, 34]. The late presentation worsens this incidence of disease in most cases. Besides, some parents tend to apply granulated edible salt or even the engine oil, which in the long run, provokes further inflammation [17]. Therefore, it is often suggested that the home-based first aid should be to cool the burn area under running tap water.
Transportation of the affected victims with burns to the hospital utilizing the ambulance or any other vehicle is highly acceptable, most notably for significant burn injury. However, there is a need for requiring inter-cities transfer requiring some attention [33, 34]. In this respect, consideration should be directed to patients with significant burns who may require traveling outside their region, this group of patients and their caregivers may experience additional economical, physical and psychological stress [31, 32]. It is advised that minor burns must be treated near homes.
Moreover, literature reports suggested that overcrowding conditions and heating with open wood fire and stoves may contribute to the cause of burns [33, 35]. Similarly, in this study, we observed that the crowded living condition of most families is a contributory factor and exposure of the child to burns as well as related distractions [33, 35]. At this juncture, we advocate for nationwide studies to inform and create awareness in families on childhood negligence and burn prevention strategies [33, 35].
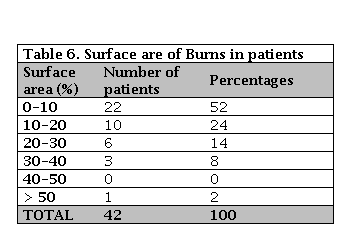
From our series, we did not record any child with inhalational injuries; therefore, the bulk of the cases were minor burn injuries with an overall TBSA of approximately 1-12% (p=0.002), also concurred with other reports [33, 35]. Our primary treatment modalities include dressing, analgesics, and antibiotics were required in many of the cases [17, 33]. “Some of our patients needed further intravenous fluid replacement and blood transfusion. Surgery was indicated in five (12%) patients [17, 33].
Similarly, Fomukong NH et al., in 2019 at the Douala General Hospital, Cameroon, studied 125 cases of pediatric burns with a median age of 4 years. Scald burns were the predominant mechanism of injury in 56 (45.5%) of patients from their report. Most patients studied had a partial-thickness burn, and most wounds involved total body surface area burns of approximately 1- 10%. The mortality rate of pediatric burns injuries obtained in their study was 29%. Flame burns (p=0.03) and BSA >25% (p=0.001) were statistically significant predictors of mortality in Douala General Hospital, Cameroon” [36].
However, Forbinake NA et al. in 2019, at the Burn Unit of the Douala General Hospital who studied 453 adult patients, equally found that flame burns constitute the most common (n=170, 37.3%) mostly due to cooking gas accidents (n=69, 15.2%). The majority of patients studied (n=203, 44.8%) had a total body surface area burns affecting about 1–9% of the entire body, and the most common type (n=225, 50.1%) were second-degree burns wounds; Most of the cases arrived at the hospital within an hour of the accident, and hospitalization averages 26.3 days [37].
Considering the preceding, the mortality rate of 4% in this series is in sharp contrast to the experience in Douala–Cameroon [34, 35] but comparable to results from other centers [16, 17, 18]. The difference in the overall outcome of the above studies in Douala –a cosmopolitan community in Cameroon compared to our series might be related to variation in the population sample and presence of burns unit at the General Hospital- Douala. Hence the center receives more patients from various locations in Cameroon.
Nonetheless, the management outcomes in our research were encouraging because we adopted some critical care protocols for burns in our institution [16, 17, 18]. These include experienced burn care nurses, regular evidence-based dressing protocols. Sloughectomy or wound debridement is done for burns wounds with sloughs initially [17]. Besides, the use of cradle for open dressing and patients nursed in a separate section of the surgical ward to prevent nosocomial infection as well as limiting houseflies from perching on the wounds [17]. We routinely commence our patients on prophylactic antibiotics because most of these wounds were considered contaminated or potentially infected. The most arduous protocol is adequate hydration of the patient and monitoring for fluid balance and where feasible early admission in burns care units, especially for significant burns injuries [17]. In addition to the above, we generally start physiotherapy promptly after appreciable wound healing. Early physiotherapy helps in preventing contractures and stiff joints [17].
CONCLUSION
Childhood burns are widely preventable. In this light, measurable success is not determined by treatment of burn injuries, but primarily by the prevention of injuries. There is significant variation in the etiology of burn injuries based on differing cultural and socioeconomic factors of each community. Considering the application of raw egg and others like local herbs, therefore pre-hospital interventions may be harmful in our settings. Early and prompt response may be desirable, with strong advocacy for aggressive and urgent public health enlightenment campaigns on the prevention of childhood.

