










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Respiratory tract infections are among the most common and diverse group of infections that have continually been a major cause of morbidity and morbidity in clinical medicine [1]. Respiratory tract infections are known as any infectious disease of the upper or lower respiratory tract. Upper respiratory tract infections (URTIs) involve the common cold, tonsillitis, laryngitis, pharyngitis, rhinitis, and otitis media. Lower respiratory tract infections (LRTIs) include acute bronchitis, and pneumonia [2]. Bacteria such as Pseudomonas aeruginosa, Streptococcus pneumoniae, Moraxella catarrhalis, and Hemophilus influenzae are among the causative agents of respiratory tract infections [3]. URTIs also cause of most antibiotic use. Approximately 60% of all outpatient antibiotics use is for respiratory infections, particularly for acute bacterial sinusitis for adults and acute bacterial otitis for children [4].
Antimicrobial resistance is a rising public health distress and strictly related to use of antibiotics [5]. In Egypt, 63.6 % of prescriptions for antibiotics are dispensed in primary healthcare, and the major cause were for respiratory tract infections [6]. Most URTIs are viral, self-limiting infections that can be self-treated without the use for antibiotics [7]. Excessive usage of antibiotics has caused resistance of bacteria toward antibiotics, representing a significant public health problem, mainly in light of the declining supply of newer antibiotic drugs [8]. Reducing request for antibiotics for self-limiting settings is considered as effective approach of averting additional antibiotic resistance [9]. To address the problem of antimicrobial resistance in URTIs, the current study aimed to investigate common bacterial profile in upper respiratory tract infection and their antibiotics sensitivity pattern.
METHODS
EXPERIMENTAL DESIGN AND SUBJECTS
This is a retrospective investigation of upper respiratory tract infections in hospital- care settings in Tripoli city. A total of 1,110 patients who had URTIs, as manifested by clinical signs and symptoms and/or chest X-ray report suggestive of URTIs admitted to Abusetta Hospital in Tripoli city, were enrolled in this study over a period of 4 year from Jan 2011 to December 2014.
Prior to enrolment, a written informed consent was obtained from each patient. In addition, patients' demographic data such as age and gender were also documented at the time of specimen gathering. Specimens were collected directly into a sterile wide mouthed container and transported to the laboratory according to standard protocol [10]. All the subjects were assured regarding privacy of disease and data. This study was ethically approved by the ethics review committee of faculty of Medical technology, University of Tripoli, Libya.
ISOLATION OF BACTERIAL STRAINS
1,110 throat swab specimens from patients of different age groups were taken in specialized containers for the study. The specimen was inoculated under a septic technique on Petri plates enclosing blood agar, MacConkey agar and chocolate agar media, and incubated at 37°C for 24 h. All the bacteria were isolated and identified using morphological, microscopy and biochemical tests. Only positive culture sensitivity reports were selected.
ANTIBIOTIC SUSCEPTIBILITY TEST
Antibiotic sensitivity was performed by Kirby- Bauer disc diffusion method as previously described [11]. Paper disks were impregnated with antibiotics including Amikacin (AK) (30µg), Amoxicillin (AX) (10µg), Ampicillin (AM) (10µg), Cefotaxime (CF) (30µg), Ceftriaxone (CT) (30µg), Cefuroxime (CE) (30µg), Ciprofloxacin (CP) (5µg), Erythromycin (ER) (15µg), Gentamycin (GM) (10µg), etc., and incubated at 37°C for 24 hours. The diameter of the zones of inhibition was measured and analysis of result based on CLSI guideline was performed [12].
RESULTS
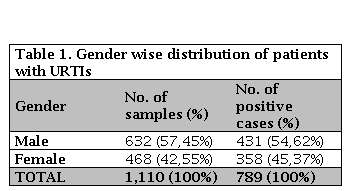
After assessing the data collected from the hospital and the tests done in the laboratory, a scenario of antibiotic resistance pattern of bacteria was evaluated. Out of the 1,110 clinical samples studied, 632 (57.45%) were from male and 468 (42.55%) were from female. Of them, 71.1% (n = 789) of the samples examined were positive for infectious bacteria (54.62% male and 45.37% female) (Table 1).
BACTERIAL ISOLATES
The dominated species of pathogenic bacteria presented with URTIs patients attended Abusetta hospital in Tripoli has been presented in (Figure 1).
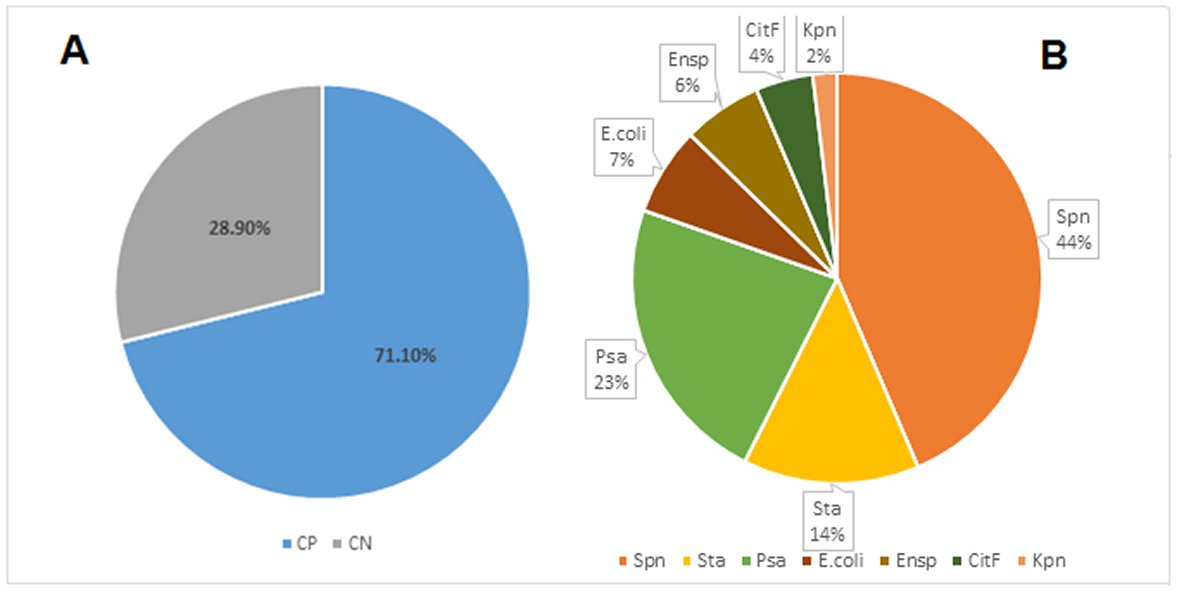
Figure 1. Detection and identification of bacterial pathogens isolated from 1,110 patients with URTIs. Fig 1A shows the rates of culture positive and culture negative specimens. Fig 1B shows the proportion of different bacterial strains among culture positive specimens.CP: Culture Positive; CN: Culture Negative; Spn: Streptococcus pneumonia; Sta: Staphylococcus aureus; Psa: Pseudomona aeruginosa; E. coli: Escherichia Coli, Ensp: Enterobacter sp; CitF: Citrobacter freundil; Kpn: Klebsiella pneumaniae.
From the various inoculated samples, 71.1% (n = 789) of the samples examined were positive for infectious bacteria. The dominated species of pathogenic bacteria were identified as Streptococcus pneumonia, followed by Pseudomonas aeruginos, Staphylococcus aureus, Escherichia Coli, Enterobacter spp, and Citrobacter. Among the identified bacterial species, the highest number 43.3% (n = 342) of isolates of streptococcus pneumonia were obtained, whereas lowest number were 2.2 % (n = 18) obtained of Klebsiella, while Pseudomona aeruginosa, Staphylococcus aurous, Escherichia Coli, Enterobacter spp, Citrobacter, contributed 13.8% (n = 109), 6.9% (n = 55), 6.2% (n = 49), 4.5% (n = 36), of total isolates, respectively.
ANTIBIOTIC SUSCEPTIBILITY TEST
Kirby- Bauer disc diffusion method was used to test the susceptibility of isolated pathogenic bacteria against different antibiotics such as amoxicillin, amoxyclav, amikacin, ciprofloxacin, clarithromycin, cefuroxime, doxycycline etc, ranging from (05 – 30 µg), and principles for suggesting whether the isolate is susceptible or resistant toward specific antibiotic have been given in Table 2. It was observed that the Streptococcus pneumoniae was highly resistant to gentamycin (51 % resistant strains) and ciprofloxacin (41 % resistant strains), whereas it was least resistant to cefotoxin (0.3 % resistant strains) and doxycycline (0.5 % resistant strains).
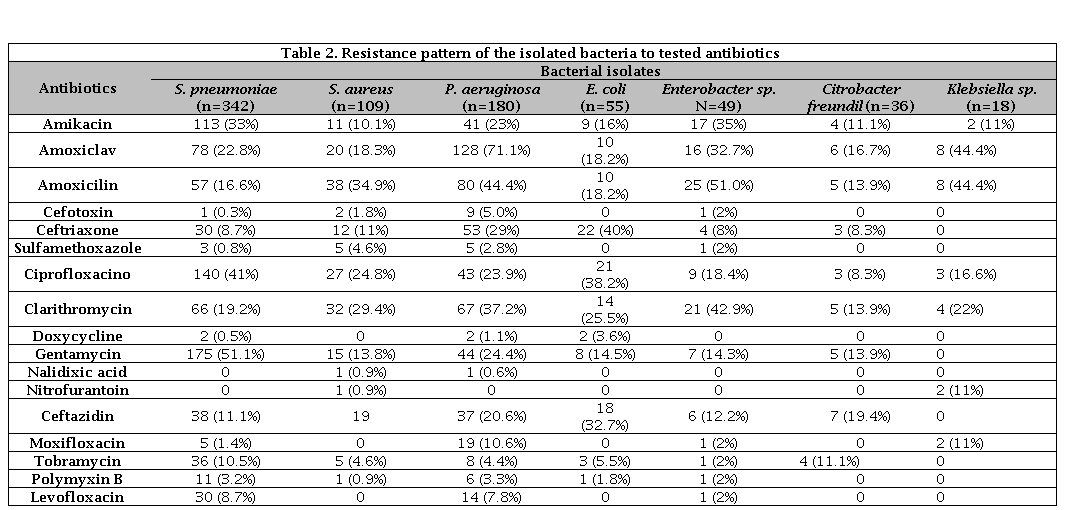
Pseudomona aeruginosa was resistant to β-lactam antibiotics such as amoxyclav, amoxicillin, ceftriaxone as well as macrolide antibiotics such as clarithromycin with percent resistance of 71, 44, 29 and 37 %, respectively (Table 2). P. aeruginosa was also moderately resistant to fluroquinolone antibiotics such as ciprofloxacin, and aminoglycosides antibiotics such as gentamicin and amikacin with percent resistance of 24, 24 and 23 %, respectively.
Our result also revealed that, Staphylococcus aureus was observed to be 35 % resistant against amoxicillin, 29 % against clarithromycin and 25 % against ciprofloxacin (Table 2). E. coli was observed to be highly resistant against ceftriaxone and ciprofloxacin compared to other antibiotics; it was having 40 and 38 % resistance against ceftriaxone and ciprofloxacin, respectively (Table 2). All other isolates were resistant to at least one antibiotic.
DISCUSSION
Isolates of S. pneumoniae, P. aeruginosa, S. aureus, Enterobacter spp, and Citrobacter represent clinically important pathogens. These pathogens have also been associated with URTIs in other studies [13, 14, 15]. Isolation of Streptococcus spp was within the range reported in most studies. A similar study reported a prevalence of 12.3% of this pathogen in Libya, although the pathogen was found to be in higher percentage in our study [16]. It was also reported with a prevalence of 22 % in Iceland, 14% in Brazil, Cameroon and 8% in Netherlands [17, 18 ,19, 20].
Earlier studies have highlighted the significance of establishing the suitable treatment for this infection to decrease probabilities of complications such as rheumatic fever, scarlet fever and endocarditis [21, 22, 23]. The high prevalence of Streptococcus spp has also been reported of 49% in Australia, 10.8% in China, and 3.5% in Italy [24, 25, 26]. Most of the bacteria isolated during the study period including S. pneumonia, P. aeruginosa, S. aureus, and Enterobacter spp fall in either nosocomial or community-acquired classes of infection, telling that proper preventive actions could limit bacterial involvement in URTIs.
Since increasing antibiotic resistance to frequently prescribed antibiotics makes bacterial infections an interdisciplinary universal threat to public health worldwide, the study also aimed to investigate antibiotic resistance patterns for the isolated bacteria. As we have mentioned in result section, our in vitro antibiotic resistance study was concerning that most of the isolates except S. pneumoniae, S. aureus, and Citrobacter freundil showed alarming levels of resistance against the commonly used first line antibiotics. Even two of 7 multidrug resistant isolates (P. aeruginosa and E. coli) exhibited resistance not only against the commonly used antibiotics but also against other antibiotics.
Antibiotic sensitivity studies exhibited Streptococcus spp to be highly resistant to gentamycin and ciprofloxacin; however, it was least resistant to cefotoxin and doxycycline. Similar studies have also reported resistance of Streptococcus spp to gentamycin and ciprofloxacin [27, 28]. In previous studies, cefotoxin was considered as the best antibiotic against Streptococcus pneumoniae [29]. However, a disappointing antibiotic sensitivity pattern of Streptococcus spp was observed for commonly prescribed antimicrobial including amoxyclav, amoxicillin, and clarithromycin with resistance rate of 22.8%, 16.6%, and 19.2%, respectively. The resistance pattern of Streptococcus spp has been reported in other studies [30]. Furthermore, the rate bacterial resistance to penicillin has also been reported in previous studies [31, 32]. Inappropriate widespread use of these antibiotics has been suggested as an explanation to this resistance.
The main cause favoring the appearance of antibiotic resistance is their widespread use. Pseudomona aeruginosa exhibited low rate of susceptibility to amoxyclav (71.4%) amoxicillin (44.4%), and ciprofloxacin (24%) which are frequently dispended over-the-counter in pharmacies, contrasts with the noticeable levels of sensitivities of the isolates to doxycycline and cefotoxin which are less-commonly used, thus suggesting an association between antibiotic use and the level of drug resistance reported in this study as previously suggested in another study [33].
Despite the improvements in healing and defensive measures, the emerging resistance toward antibiotics is a growing concern among clinicians and other health professionals worldwide. The uncritical and irrational use of antibiotics have donated to the emergence of resistance, which may turn out to be a principal cause of morbidity and mortality in the developing countries.
A precious antibiotic treatment is in demand to overcome this critical concern, but the shortage of evidence regarding the principle causes of antibiotic sensitivity patterns in countries like Libya have made it difficult. The information about antibiotic resistance profile reported here in this study is expected to promote awareness among physicians, community pharmacist, as well as among policy makers of community and private sectors in the country.
CONCLUSION
In summary, URTIs incidence, as well as pathogen exposure rates, were high is Abusetta hospital. S. pneumoniae and P. aeruginosa were the predominant bacterial causative agents, with amoxyclav and amoxicillin being resistance to most identified pathogenic bacteria in our population sample. There is calls for a crucial need to impose evidence‑based guidelines and the delivery of educational program to promote better antibiotic dispensing practices that can be worth in improving current resistant pattern in Libya. Although the number of isolates used may be small to draw significant assumptions on the susceptibility patterns, they, however, deliver baseline data for future investigations, particularly considering the thing that no such data have been reported in this vicinity notwithstanding the very high rate of antibiotic misuse. These findings are, therefore, of clinical and epidemiological importance.

