










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The rising influence of social media in our private and professional lives is a new force that affects our understanding of medical professionalism, especially in the last decade. Interestingly, many social media tools are available for health care professionals (HCPs). Such social media, as a part of the Web 2.0, include blogs, wikis, podcasts, and social networking platforms such as Twitter, LinkedIn, YouTube, and Facebook, to name just a few [1, 2, 3, 4, 5, 6, 7, 8]. Some researchers suggested that these tools could significantly enhance professional networking and education, besides the beneficial role in organizational promotion, patient care, patient education, and public health programs [1, 4, 6, 7, 8, 9, 10]. Nonetheless, there are inherent potential risks to patients and HCPs regarding the distribution of inadequate quality information, damage to a professional image, breaches of patient privacy, violation of personal–professional boundaries, and licensing or legal issues [1, 3, 8, 10, 11, 12, 13, 14, 15, 16]. Interestingly, several guidelines have been issued by health care institutions and professional organizations to prevent these risks [1, 4, 7, 10, 16, 17].
DEFINITION OF SOCIAL MEDIA
The meaning of “social media” is broad and continually evolving. It is often remarked as Internet-based tools which guarantee individuals and communities to share information, to gather and communicate. Such platforms equally facilitate sharing of ideas, personal messages, images, and other content; and, in some cases, to collaborate with other users in real-time [1, 3, 4, 5, 6]. Social media are otherwise known as “social networking” or “Web 2.0” [1, 5].
Social media sites are providers of a variety of features that serve different purposes for the individual user [1, 18]. They may include a myriad of other media, which can be grouped by purpose, serving functions such as 1) Social networking (Facebook, MySpace, Google Plus, Twitter); 2) Professional networking (LinkedIn, ResearchGate); 3) Media sharing (YouTube, Flickr, Instagram, Tik Tok); 4) Content production (blogs [Tumblr, Blogger] and microblogs [Twitter]); 5) Knowledge/information aggregation (Wikipedia); 6) Virtual reality and gaming environments (Second Life) [1, 7, 8].
In the last decade, participation in social media by the general public has increased sharply over the past nine years [1, 6, 12]. The estimate of adults using social media has increased from 8% to 72% since 2005 in the U.S., [5, 11]. The utilization of social media is prevalent across all ages and professions and is pervasive around the world [3, 8].
PANDEMICS OF CORONAVIRUS DISEASE 2019
SARS-CoV-2 is remarked as a novel virus responsible for the pandemic of the severe acute respiratory syndrome, also known as Coronavirus Disease 2019 (COVID-19). First discovered in December 2019, SARS-CoV-2 has been the causative agent for a pneumonic illness initially detected in Wuhan City, Hubei province, China. Surprisingly, COVID-19 had spread throughout China and to 210 additional countries and territories as of April 13, 2020. Phylogenetic data implicate a zoonotic origin, and the rapid spread suggests ongoing person-to-person transmission. Several studies offer further insight into person-to-person transmission [19, 20, 21, 22]. However, there remain unknown details regarding the transmission between humans, including the level of exposure to a confirmed case at which transmission is more likely to occur. On March 15, 2020, Illinois, USA, reported the state's first laboratory-confirmed case (index case) of SARS-CoV-2 in a traveler who returned from Wuhan, China [19, 23]. New guideline to help protect the citizen from the transmission of the SARS-CoV-2 virus has been issued by the International Federation of the Red Cross (IFRC), UNICEF, and the World Health Organization (WHO) published on March 26, 2020. The direction provides practical checklists to keep schools protected from the pandemic. It also advises the State and Federal governments on how to adapt and implement emergency plans for educational facilities [19, 22]. The primary focus is Global public health security and efforts to preventing the spread of COVID-19 pandemic. The guideline equally focuses on serious attempts to detect, report, and support infection prevention and control measures in general. Global health governance assists clinicians with laboratory facilities, especially those with state-of-the-art tools, in addition to quick reporting, which are crucial components of this response [19, 23]. The overall response permits rapid information outflow and collaboration, especially between laboratory scientists and clinicians on the frontline. Healthcare workers are most at risk from outbreaks due to reemerging and novel pathogens. This risk has been observed in the current COVID-19 outbreak in China, whereas estimated 1716 health workers were infected by the virus, with six deaths as on 14th February 2020 [19, 24]. As it was observed in a single-center case series of SARS-CoV-2 from Wuhan published recently [19, 24]. The WHO released data dated April 13, 2020, showed a total estimated figure of COVID-19 infections at 1,920,181 cases, with 119,410 deaths and 443,735 recovered cases [25].
OBJECTIVE OF THE STUDY
This paper aims to explore the roles and responsibilities of physicians in the era of social media. The authors will take as an example the current pandemic of COVID-19.
The authors will critically examine how social media impact the way populations trust the recommendations of the governments and how they respect the measures on a day-to-day basis.
METHODS
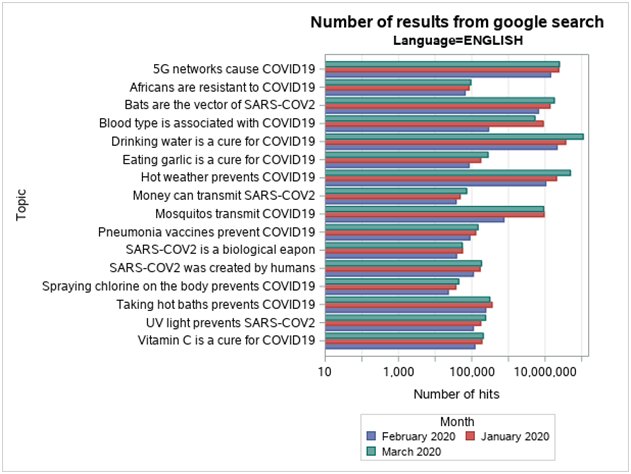
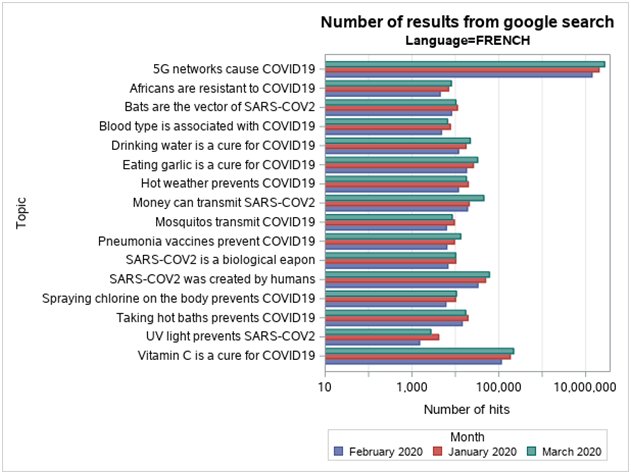
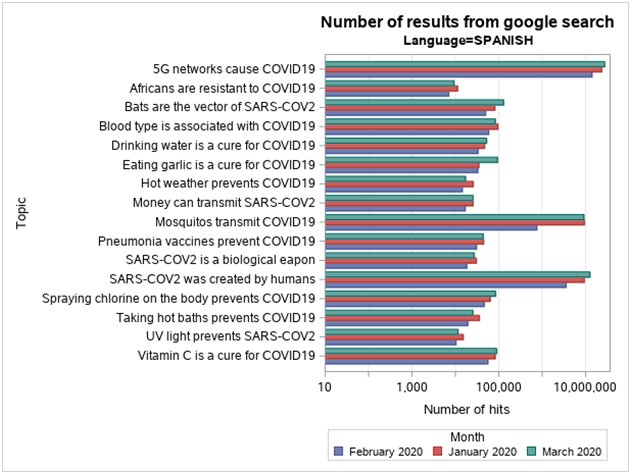
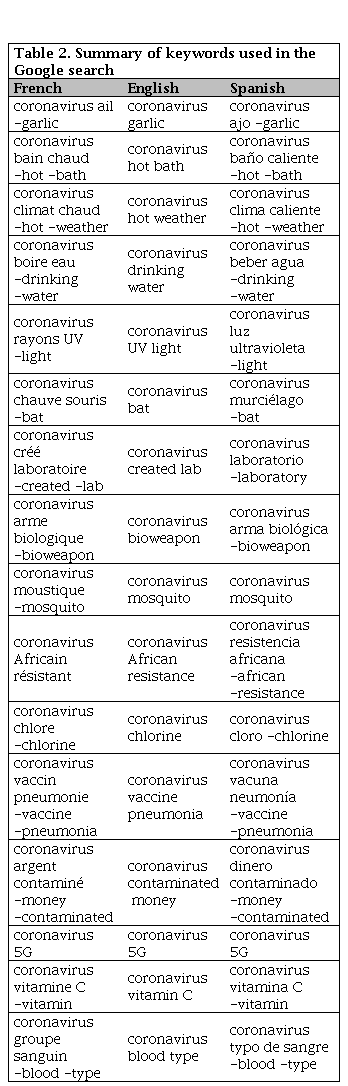
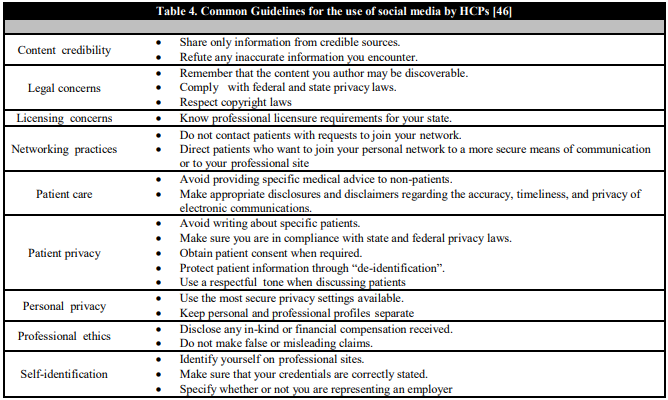
We identified relevant articles to date using a manual library search (PubMed), journal publications on the subject, and critically reviewed them. The google search was done in three languages serially, including French, English, and Spanish, for the following periods between January 1st to January 31st, February 1st to February 29th and March 1st to March 31st, 2020 respectively. Interestingly, the key highlights of fake news identified relating to COVID -19 pandemic are summarized according to Table 1a and 1b [26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44]. The various keywords used in the Google search in French, English, and Spanish, as outlined in Table 2. The numbers of results from Google search were, therefore, as represented in bar-charts with English, French, Spanish languages, according to Figure 1, Figure 2, Figure 3, respectively. Meanwhile, Table 3 shows concepts for Health Care Organizations' social media policies [45], and Table 4 represents standard guidelines for the use of social media by HCPs [46].



SOCIAL MEDIA AND THE CLINICIANS
Social media provide Clinicians with a direct platform to i) share information, ii) debate health care policy and practice issues, iii) promote health behaviors, iv) engage with the public, and v) educate and interact with patients, caregivers, students, or colleagues [1, 6, 11, 14, 15]. Social media sites have been used to facilitate i) health outcomes, ii) develop a professional network, iii) increase personal awareness of news and discoveries, iv) motivate patients, and v) provide health information to the community [1, 8, 11]. These platforms impact the Physicians by way of delivering online communities sites where they can a) read news articles, b) listen to experts, c) get informed on research and medical developments, d) consult colleagues regarding patient issues and e) network [1, 9]. There is an opportunity to i) share cases and ideas, ii) discuss practice management challenges, iii) make referrals, iv) disseminate their research, v) market their practices, or engage in health advocacy [1, 14]. Very few physicians communicate directly with patients to augment clinical care through social media platforms [1, 9]. From a survey of more than 4,000 physicians conducted by the social media site QuantiaMD, the authors found that estimated 90% of physicians use social media sites for personal activities [1, 9, 14].
In contrast, only 65% use these sites for professional reasons [1, 9, 14]. Other reports found that nearly a third of physicians have been reported participating in social networks professionally [1, 8]. In the overall analysis, the use of social media by physicians is increasing, especially for both personal and professional reasons [1, 4, 9].
THE SOCIAL MEDIA “WATCHDOG” DYNAMICS
The great hero of being our brother's keeper and fulfilling the criteria for social media watchdog dynamics was demonstrated by one physician who was regarded as the "whistleblower" for the coronavirus. Dr Li Wenliang was generally know to be one of the first victims to have sucumbed to the novel coronavirus infection, COVID-19 [47]. Li, 34, was a consultan ophtalmologist at Wuhan Central Hospital, China. Subsequently, it became the reality of the COVID-19 threat to frontline health workers, i.e., the clinicians taking care of patients. On 30th December 2019, he warned a closed group of ex-medical school classmates on the WeChat social media site of “Seven cases of the severe acute respiratory syndrome (SARS) like illness with links to the Huanan Seafood Wholesale Market” at his hospital [25]. The above corresponded to the first alert received by the WHO from the Wuhan municipal health service on the outbreak of COVID-19 in China [28]. Incidentally, Dr. Li Wenliang was among eight people reprimanded by security officers for “spreading rumors” [47]. He subsequently contracted COVID-19 in a tragic turn of events. Following a short period of hospitalization and intensive care, he succumbed to death on Friday, the 7th of February, 2020 [47, 48]. This case is a reminder of the significant role Physicians could perform as watch-dogs, besides the impact of revealing risks of the emerging pandemic to clinicians worldwide.
Dr. Li Wenliang's name is on the list of HCPs that were at the forefront of the pandemic of SARS, Ebola, MERS, and now COVID-19 [47, 48]. We reiterate that it was the clinicians in Wuhan who sounded the alarm about the emergence of COVID-19, which was rapidly identified after these clinicians, sent samples to a reference laboratory for confirmation [47, 49].
THE CHALLENGES OF SOCIAL MEDIA
The main limitation of social media is the poor quality of information and a lack of reliability [1, 15]. The majorities of authors of medical information found on social media sites are often unknown or are identified by limited information [1, 13, 15]. Also, the medical information may be i) unreferenced, ii) incomplete, and iii) informal [12]. Interestingly evidence-based medicine de-emphasizes anecdotal reports. Social media tend to emphasize them, relying on individual patient stories for collective medical knowledge [1, 2]. These unethical practices make social media users be at risk of overt conflicts of interest that they may be incapable of interpreting [1, 13].
Several efforts are being put in place after all that may be useful in addressing this problem. The HCPs have a responsibility to safe-guiding patients from vulnerable websites, and to direct them to credible websites where the information is subject to quality control [1, 10]. The World Health Organization is leading an effort to establish a new domain suffix that would be used solely for validated health information with the Internet Corporation for Assigned Names and Numbers [1, 16]. The issuance of this domain suffix would be strictly regulated. Interestingly, it is expected that the content of websites with these addresses would be monitored to ensure compliance with strict quality criteria [1, 18]. The goal is that when providing results in response to health-related inquiries, these domain addresses would be prioritized by search engines [1, 16]. Other challenges of utilizing social media include 1) Damage to the professional image in the form of posting unprofessional content that can impact unfavorably on HCPs, students, and affiliated institutions [2]. 2) Breaches of patient privacy on social media with potential for negative repercussions; for instance, those resulting from the violation of patient confidentiality [1, 6]. Such infractions may have medicolegal implications on HCPs and health care entities in general [1, 45, 46]. 3) Violation of the Patient–HCP Boundary, which means that HCPs may be violating the patient-HCP boundary even if patients initiate online communication when they interact with their patients on social media [1, 10]. Some of the current efforts at addressing these challenges are summarized in Table 3 and Table 4 [45, 46].
SOCIAL MEDIA AND FAKE NEWS ASSOCIATED WITH COVID-19
The ease with which people share their personal experiences or anecdotal reports on social media enables misinformation about the current pandemic to spread at an alarming rate. It is, therefore, crucial for us as physicians to verify and inform the public which sources are reliable and contain accurate information. Indeed, misconceptions regarding the origins, the prevention methods, and the treatment of COVID-19 may have had detrimental consequences on the beliefs of the disease's existence, manifestations, and treatment in the general population.
As the news of a novel virus started spreading, so did conspiracy theories regarding its origins. One popular theory is that SARS-CoV-2 was artificially fabricated in a research laboratory in Wuhan to be used as a biological weapon. This rumor gained significant coverage throughout social media platforms, even without an identifiable credible source to verify these claims. Several posts that display this similar fake theory continue to be shared even though genetic data clearly show that SARS-CoV-2 is not derived from previously known viruses and therefore, could not be a result of laboratory manipulation [50]. Further analysis of its genome proves that it came from nature by an animal source. Conspiracies such as this one and misinformation, in general, have the potential of harming the general public; therefore, it is essential for physicians to take a position by spreading scientific evidence in place of this fake news.
The rumors about COVID-19 treatment and prevention methods have also been circulating, creating public confusion and potentially leading to harmful self-medication. Notable rumors include eating garlic, frequently sipping hot water and taking mega-doses of vitamin C to prevent getting infected by COVID-19 has been widely shared in various social media (Facebook, WhatsApp, etc.) [51]. “Even though there is no scientific evidence to back these claims up, people have been following these pieces of advice deemed as miracle cures. Although most of the proposed ‘treatments’ are harmless, a few can lead to significant health issues, especially if handled without the supervision of a health care professional” [51]. The example of chloroquine is remarkable in this instance; three cases of chloroquine overdoses were found in Nigeria after President Donald Trump described the drug as “one of the biggest game-changers in the history of medicine” [51]. A chlorine dioxide solution with potentially life-threatening effects has also been marketed online as a medical treatment, forcing the U.S. Food and Drug Administration to issue a warning against its use [52]. These examples demonstrate the importance of spreading accurate information over conjectures that lead to confusion, which prevents us from efficiently containing the spread of this virus. Besides, Table 1a and 1b of the appendix presents several of these myths along with scientific evidence against those claims.
CHLOROQUINE IN THE POST COVID-19 ERA
In 1934, chloroquine was first discovered by Hans Andersag [53, 54]. Following the discovery, it was on the WHO's List of Essential Medicines, the safest and most effective medicines needed in a health system [55]. It was available as a generic medication [56]. Furthermore, chloroquine was initially withdrawn from circulation due to bizarre side effects which include blurring of vision, nausea, vomiting, abdominal cramps, headache, diarrhea, pedal edema, shortness of breath, pale lips/nails/skin, muscle weakness, easy bruising/bleeding, hearing and mental problems [57, 58]; Unwanted/uncontrolled movements (including tongue and face twitching) [57], Deafness or tinnitus; Mental/mood changes (such as confusion, personality changes, unusual thoughts/behavior, depression, feeling being watched, hallucinating) [57, 58]; Skin itchiness, skin color changes, hair loss, and skin rashes [58, 59]; Chloroquine-induced itching is very common among black Africans (70%); [60] Unpleasant metallic taste [61]; Chloroquine retinopathy, and electrocardiographic changes [62]; others adverse reactions include pancytopenia, aplastic anemia, reversible agranulocytosis, low blood platelets, and neutropenia [63].
Many Nigerian households still use tablets containing chloroquine for treating malaria even though it was banned in 2005, given the side effects and high rate of malaria resistance to this drug. News of a February study in China about the use of chloroquine for the coronavirus had already sparked a lively debate in most parts of Africa, so people were stocking up the drug.
A COST INCREASE OF CHLOROQUINE AFTER MEDIA ASSUMPTION
In a chaotic press conference on Thursday, March 12, 2020, President Donald Trump of the USA even touted chloroquine as a coronavirus treatment, saying the medication was “approved for the prescription” [64, 65]. However, the drug is approved by the FDA exclusively for use as an antimalarial. Stephen Hahn, the commissioner of the Food and Drug Administration, appeared to contradict the president almost immediately, saying any analysis of the drug's efficacy as a coronavirus treatment should be conducted “in a setting of a clinical trial” [64, 65].
Following this announcement, the price of Chloroquine phosphate sky-rocketed in the market as it showed some promise treating patients with the novel coronavirus and the respiratory disease it causes. A pharmaceutical drug representative said the initial price increases came after the drug manufacturing companies “made significant investments in ramping up capacity,” and equally a response to the “increasing demands and rapidly declining drug-stock volume in the market” [64, 65].
PURCHASING CHLOROQUINE IN BLACK MARKET AND OVER THE COUNTER
In most of the low-income countries of sub-Saharan Africa, medicine sellers can be found in drug shops, general stores, kiosks, market stalls. Also, these medicine sellers operate as itinerant hawkers, with considerable variation in-retailer type across settings. Like any business, they maintain their existence in response to consumer demand, in this case, for accessible, convenient, reliable, and affordable antimalarial and painkiller supplies. Medicine sellers are generally closer to home than formal facilities [66, 67, 68, 69]. For example, in coastal Kenya, 87% of rural households live within one km of a shop, but only 32% within two km of a government dispensary or private clinic [66, 70].
Moreover, their service is faster, and their weekly opening hours maybe twice as long as those in health facilities [66, 71]. As drug stock-outs are common in public facilities, medicine sellers form an important alternative supply, and their staff is often perceived as more friendly and approachable [66]. Finally, cost is an important motivation [66, 72]. In some settings, patients pay less at medicine sellers than at formal facilities [66, 73, 74] reflecting the lack of fees for consultation or diagnostic tests, illicit charges at some facilities, and the fact that sub-optimal drug doses can be purchased [66, 69] Credit may also be easily obtained at retail outlets [66, 75]. Even where inexpensive or free drugs are available at facilities, people may patronize medicine sellers to avoid the travel and time costs involved in accessing regular care [66, 72].
However, there are concerns about the dispensing of the correct drugs and information that medicine sellers provide. In many instances, the type or dose of medicine is inappropriate for the presenting complaint [66, 76, 77]. The above scenarios are commonly referred to as the “Black-market” band-wagon effect. In a baseline survey in Kenya, only 4% of children given store-bought chloroquine received an appropriate dose, and only 2% received this dose over the recommended three-day period [66, 78, 79, 80, 81].
ASIAN STUDY WITH REMDESIVIR AND CHLOROQUINE
To date, there is no official statement on any specific treatment against the new virus by the WHO. Therefore, identifying active antiviral agents to combat the disease is urgently needed. Thus, an efficient approach to drug discovery is to test whether the existing antiviral drugs are effective in treating related viral infections. The COVID-19 belongs to the group of Betacoronaviruses. The other known varieties include i) SARS-CoV and ii) Middle East respiratory syndrome CoV (MERS-CoV). Several drugs have been used in patients with SARS or MERS, such as ribavirin, interferon, lopinavir-ritonavir, corticosteroids, However, the efficacy of some drugs remains controversial [82, 83, 84] In this Asian study, the antiviral efficiency of five FDA-approved drugs including i) ribavirin, ii) penciclovir, iii) nitazoxanide, iv) nafamostat, v) chloroquine, and two well-known broad-spectrum antiviral drugs vi) remdesivir (GS-5734) and vii) favipiravir (T-705) against a clinical isolate of COVID-19 in vitro was well evaluated. The standard assays were carried out to measure the effects of these compounds on the cytotoxicity, virus yield, and infection rates of COVID-19 [82, 83, 84].
The report confirmed that Remdesivir proved to be a highly promising antiviral drug against several RNA viruses. This antiviral role was covering SARS/MERS-CoV5 infections in cultured cells, mice, and non-human primate (NHP) models. Also, the drug is being developed for the treatment of Ebola virus infection [82, 85]. Remdesivir is an adenosine analog, which incorporates into nascent viral RNA chains and results in premature termination [82, 86]. Further study showed that remdesivir functioned at a stage post virus entry, which is in agreement with its putative antiviral mechanism as a nucleotide analog.
Interestingly, a similar study performed on human subjects proved that chloroquine blocks virus infection by increasing endosomal pH required for virus/cell fusion, as well as to interfere with the glycosylation of cellular receptors of SARS-CoV [82, 87]. Besides, chloroquine has an immune-modulating activity, which may synergistically enhance its antiviral effect in vivo, consequently serving its antiviral activity. Chloroquine is well distributed in the whole body fluid, including lung, after oral administration. Moreover, chloroquine and derivative hydroxychloroquine are cheap and safe drugs already in use for over 70 years. Therefore, it is clinically applicable to COVID-19 [82, 87, 88].
The Asian researchers reported that the combination of remdesivir and chloroquine is highly effective in the control of COVID-19 infection in vitro. Hence, the report suggests further clinical randomized controlled trials be performed to further elucidate their effects and outcomes in human patients suffering from the novel coronavirus disease [82, 87, 88, 89].
PROFESSOR DIDIER RAOULT’S STUDY ON CHLOROQUINE
The charismatic Professor Didier Raoult, Director of the Research Unit in Infectious and Tropical Emergent Diseases (URMITE) in Marseille, stated that he had found a simple cure for COVID-19 infection. The humble chloroquine, the cheap unpatented substance used to treat malaria and autoimmune diseases lupus and rheumatism, is becoming an enigma in the face of social media publicity that greeted the new discovery [90]. Although initial research findings did not support antiviral therapies, these earlier reports didn't prevent Raoult from deciding that chloroquine can cure coronavirus infections; also, notwithstanding the serious side effects of the medication [91]. As part of the evidence-based protocol, to establish the efficacy of his latest therapy for Coronavirus disease, Professor Raoult treated twenty-four patients at his institution with the derivative hydroxychloroquine alone or in combination with the drug azithromycin. Surprisingly, the trial was non-controlled, non- randomized, ethically approved after the study already began. There were sixteen control patients that were treated in different clinics [91]. After some clinical adjustments of his trial therapy, a preprint was published simultaneously with a paper in a peer-reviewed journal where one of the co-authors is the editor.
Next, a Lawyer with whom Professor Raoult collaborated posted the miracle cure in Fox News. Incidentally, Fox News is the TV channel US President Donald Trump watches all day to get all his information. Trump then tweeted it that “HYDROXYCHLOROQUINE & AZITHROMYCIN, taken together, have a real chance to be one of the biggest game-changers in the history of medicine. The FDA has moved mountains – Thank You! Hopefully, they will BOTH (H works better with A, International Journal of Antimicrobial Agents)” [63, 64]
Furthermore, the event that followed Professor Raoult's announcement could best be described as chaotic. Several individuals worldwide stormed pharmacies and pet shops for chloroquine. Some unfortunate persons even killed themselves from chloroquine overdose-poisoning [91]. It is crucial to add here how YouTube has played an enormous role in this media publicity of inadequately tested drugs. Surprisingly, YouTube is still aiding and abetting the pro-Raoult group, while the anti-Raoult is continually fighting over the video content and contest. Even on Facebook, physicians are split into two, especially French physicians. We must reiterate the indirect harmful effect of Professor Raoult's declaration. This antecedent suggests that there is a strong possibility of this report being included in a properly designed study later, thus complicating such discovery [91].
Subsequently, the Indian government banned chloroquine export, while national authorities, including the French government, issued a national health policy accepting chloroquine as the medicine to treat COVID-19 disease in some situations. Other Chinese researchers submitted that Raoult's report is the exact opposite of proper clinical research practice [91].
BCG VACCINE CONTROVERSY AND COVID-19
There was a controversial debate that arose following the statement by two French physicians on LCI TV channel on Wednesday, April 1st, 2020. Camille Locht, director of research at Inserm in Lille, and Jean-Paul Mira, head of the intensive medicine and resuscitation department at the Cochin hospital, were discussing the new study on BCG vaccination in the prevention of COVID-19 [92].
Following their inappropriate statements seen by several members of the African community as racist statements, parents warned not to vaccinate their children on Whatsapp, Youtube, which was squealed to a conspiracy theory report that the vaccines targeted to destroy or reduce the population of the Africans [92].
KEY PANEL MESSAGE
The rising influence of social media in our private and professional lives is a new force that affects our understanding of medical professionalism especially in the last decade
These new technological tools become very relevant to enhance i) professional networking and education, ii) organizational promotion, iii) patient care, iv) patient education and v) public health programs [4, 5, 6, 7 ,8, 9, 10].
These platforms present potential risks to patients and HCPs regarding the distribution of imperfect quality information, damage to a professional image, breaches of patient privacy, violation of personal–professional boundaries, and licensing or legal issues [3, 4, 5, 8, 10, 11, 12, 13, 14, 15, 16].
There is urgent advocacy for operation guidelines for preventing these associated risks expectedly issued by several health care institutions and professional organizations [4, 7, 10, 16, 17].
Physician must remain resolute in the face of the prevailing situations and should serve as “watchdog” for the preservation of the tenets of guiding principles of our “Noble Profession,” besides the impact of revealing risks of the emerging pandemic to clinicians worldwide.
RECOMMENDATIONS: PHYSICIAN ROLE AND RESPONSIBILITY IN THE CONTEXT OF A PANDEMIC
The primary priority is addressing the most significant concerns by clinicians worldwide, “what are the estimate figures of people infected since many cases may be mild or asymptomatic?” Recent modeling estimated the population at risk to be between 0.75 per 100,000 to 15.8 per 100,000 populations [93]. The accuracy of incidence estimates depends on the early deployment of sensitive and specific viral serological tests.
Early recognition of the disease in international and even local travelers is a significant aspect of surveillance for the importation of emerging pandemic. Multi-site collaborations such as the GeoSentinel Surveillance Network can act as sentinel systems to recognize new patterns of disease in travelers from specific areas [94].
The current COVID-19 pandemic underscores the critical importance of prioritizing diagnosis through clinician awareness and modern laboratory techniques such as NGS.
Dr. Li Wenliang's example is worthy of emulation and encouraging clinicians worldwide to be vigilant, bold, and quick in reporting unusual clinical presentations. The COVID-19 pandemic underscores the responsibilities and the vulnerabilities of frontline health care workers in tackling novel and highly transmissible pathogens.
We need to deploy the best of clinical skills, and backup of laboratory support, to rapidly detect and report any suspicion of emerging infections. Rapid, transparent communication is paramount when infectious diseases develop. This awareness is the only way to prevent significant outbreaks and will save many lives.
Advocacy for proper utilization of social media will be highly beneficial in the long-run.
CONCLUSIONS
Social media undeniably pose several potential risks to health care organizations. These risks undermine the safety and security of i) patient information, ii) patient consent, iii) employment practices, iv) physician credentialing and licensure, v) the violation of HCP–patient boundaries, and vi) other ethical issues. In an attempt to avoid these pitfalls, several health care organizations and professional societies issued guidelines in the form of sound and useful principles that HCPs should follow. Notwithstanding these pitfalls, when used wisely and prudently, social media sites and platforms offer the potential to promote individual and public health, as well as professional development and advancement.

