










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkArchivos Españoles de Urología (Ed. impresa)
versión impresa ISSN 0004-0614
Arch. Esp. Urol. vol.58 no.5 jun. 2005
International Section
UROTHELIAL CARCINOMA IN A CHILD.
Alejandro Rodriguez, David Burday, Wade Sexton, Nazeel Ahmad and Julio M. Pow-Sang.
Moffit Cancer Center at the University of South Florida. Tampa. Florida
Resumen.- OBJETIVO: El carcinoma urotelial de vejiga ocurre raramente en las primeras 2 décadas de la vida. Presentamos el caso de un niño de 12 años que presentó un carcinoma urotelial Ta grado II/III.
MÉTODOS: Describimos la presentación clínica y el proceso de diagnóstico, asi como el tratamiento y seguimiento. Finalmente, revisamos la literatura para analizar la etiología, tratamiento, y seguimiento del carcinoma urotelial en la población pediátrica.
RESULTADOS: Desde 1950, existen menos de 100 casos de carcinoma urotelial reportados en pacientes menores de 30 años, y mucho menos en niños y adolecentes. La mayoría de las pequeñas series describen estos tumors como de caracteristicas superficiales y de bajo grado (I-II). Este niño presentó una hematuria asintomática y una resonancia magnética descubrió una masa sólida y papilar que medía 2.7 cm. La cistoscopía y resección del tumor confirmó el diagnóstico. Una segunda resección 2 meses después confirmó que no existía tumor residual.
CONCLUSIONES: No existen normas establecidas acerca de la etiología, tratamiento, y seguimiento del carcinoma urotelial en pacientes pediátricos. Niños con hematuria macroscópica como síntoma principal deberían ser sometidos a una evaluación completa para descartar la presencia de un carcinoma urotelial.
Palabras clave: Carcinoma. Urotelial. Niño.
Summary.- OBJECTIVES: Urothelial carcinoma of the bladder occurs rarely in the first 2 decades of life. We report a case of a 12 year-old child that presented with a Ta grade II/III urothelial carcinoma of the bladder.
METHODS: We describe its clinical presentation and diagnostic procedures as well as treatment and followup. Finally, we review the literature to analyze the etiology, treatment, and surveillance of urothelial carcinoma in the pediatric population.
RESULTS: Since 1950, there are less than 100 cases of urothelial carcinoma reported in patients less than 30 years, and even less in children and adolescents. Most of the small series describe these tumors as being characteristically superficial and low grade (I-II). This child presented with silent macroscopic hematuria and an MRI revealed a solid and papillary mass measuring 2.7 cm. A cystoscopy and resection of the tumor confirmed the diagnosis. A re-resection at two months confirmed no residual tumor in the bladder.
CONCLUSIONS: There is no established criteria for the etiology, treatment, and surveillance of urothelial carcinoma in the pediatric population. Children with gross hematuria as the presenting complaint should undergo a complete evaluation to rule out the presence of urothelial carcinoma.
Keywords: Carcinoma. Urothelial. Child.
Address correspondence to:
Alejandro Rodriguez, M.D.
Moffitt Cancer Center and Research Institute
Genitourinary oncology Program
12902 Magnolia Drive
Tampa, Florida 33612-9497. USA
RodrigAr@moffitt.usf.edu
Accepted for publication: December 9th, 2004
INTRODUCTION
Urothelial carcinoma of the bladder occurs rarely in the first 2 decades of life. Since 1950, there are less than 100 cases reported in patients less than 30 years, and even less in children and adolescents. (1) Most of the small series describe these tumors as being characteristically superficial and low grade (I-II). (1-5) The etiology, invasive potential, treatment and surveillance of high-risk superficial transitional cell carcinoma of the bladder in children are not well established due to its even extreme rarity. We report a case of a 12 year-old boy with Ta grade II/III urothelial carcinoma of the bladder.
CASE REPORT
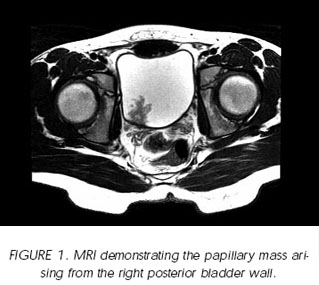
A 12 year-old boy presented with painless intermittent macroscopic hematuria. An IVP demonstrated normal kidneys and ureters, however an abdominal ultrasound detected an intravesical mass. An MRI revealed that the mass was solid and papillary, measuring 2.1 x 2.7 x 2.5 cm, arising from the right posterior wall of the bladder. (Figure 1) A cystoscopy and transurethral resection of the tumor was performed immediately. (Figure 2).

The pathology report described a papillary urothelial carcinoma consisting of papillae covered by an atypical urothelium. The cells covering the papillae varied from an almost normal appearance to atypical urothelium. The atypical cells had moderate eosinophilic cytoplasm, focally irregular nuclei and prominent nucleoli. Few scattered mitotic figures were identified. The final grade of this superficial urothelial carcinoma of the bladder was considered as grade I-II/III by three pathologists. (Figure 3)

Since this tumor was different from most of the low-grade papillary tumors reported in the first two decades of life in case reports and small series due to its larger size (2.7 cm), we performed a cystoscopy and re-resection at 2 months that confirmed that the bladder was free of tumor. It is important to mention that there were no environmental risks associated with this pathology in this patient.
DISCUSSION
This child presented with macroscopic hematuria, in accordance with approximately 80 percent of the historical controls. (1-5) Ultrasound discovered a bladder lesion that had the possibility of being a retained clot, however the MRI of the bladder demonstrated clearly that this was a papillary solid lesion arising from the bladder. We agree with reports that suggest that ultrasound is effective in identifying bladder tumors and it should be considered in pediatric patients with any degree of hematuria not associated with urinary infection or trauma. (1) However, MRI could also be used as a diagnostic tool for these pediatric patients, specially, when cystoscopy at this age will mean requiring general anaesthesia. The IVP did not demonstrate any particular finding, and for this reason we think that in future cases an ultrasound and an MRI could be the best non-invasive diagnostic tools in children. This would effectively avoid contrast material that may produce allergic reactions or even nephrotoxicity in this age group of patients.
Urothelial carcinoma in children may differ from that in adults in its biological behavior and most likely in its etiology. The concept of field change of the bladder epithelium is unlikely in the pediatric patient with no known history of exposure to carcinogens. Because the lesion in this patient was a large 2.7 cm tumor with a grade II/III and cytologic features atypical for most patients in this particular age group, we elected to repeat the cystoscopy and resect the tumor bed to ensure that the patient was not clinically understaged.
With respect to disease surveillance, cystocopy is certainly the most invasive modality, necessitating general anesthesia in most pediatric patients. Some argue against interval cystoscopy because of the risk of urethral damage in this age group and the necessity for anesthesia. (1) We could select using ultrasound, urinalysis and cytology for our surveillance protocol, especially after the re-resection confirmed no remaining tumor. However, as cystoscopy is the best diagnostic tool for detecting any recurrence, and due to the fact that there is no defined protocol for follow-up in this age group of patients we plan to follow him with a modified adult protocol incorporating cystoscopy.
Urothelial carcinoma is rare in children. Most of the reported cases are grade I tumors, and available data suggest an excellent prognosis with low recurrence and progression rates. There is no established criteria for the etiology, treatment, and surveillance of urothelial carcinoma in the pediatric population. Children with gross hematuria as the presenting complaint should undergo a complete evaluation to rule out the presence of urothelial carcinoma.
REFERENCES AND RECOMENDED READING (*of special interest, **of outstanding interest)
**1. HOENIG, D.M.; McRAE, S.; CHEN, S.C. y cols.: "Transitional cell carcinoma of the bladder in the Pediatric Patient". J. Urol., 156: 203, 1996. [ Links ]
2. BENSON, R.C. Jr.; TOMERA, K.M.; KELALIS, P.P.: "Transitional cell carcinoma of the bladder in children and adolescents". J. Urol., 130: 54, 1983. [ Links ]
3. JAVADPOUR, N.; MOSTOFI, F.K.: "Primary epithelial tumors of the bladder in the first two decades of life". J. Urol., 101: 706, 1969. [ Links ]
4. KHASIDY, L.R.; KHASHU, B.; MALLET, E.C. y cols.: "Transitional cell carcinoma of the bladder in children". Urology, 35: 142, 1990. [ Links ]
*5. KEETCH, D.W.; MANLEY, C.B.; CATALONA, W.J. y cols.: "Transitional cell carcinoma of bladder in children and adolescents". Urology, 42: 447, 1993. [ Links ]

