










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.1 Madrid ene./feb. 2016
https://dx.doi.org/10.20960/nh.7
TRABAJO ORIGINAL / Nutrición artificial
The influence of the initial state of nutrition on the lifespan of patients with amyotrophic lateral sclerosis (ALS) during home enteral nutrition
La influencia del estado inicial de la nutrición en la esperanza de vida de pacientes con esclerosis lateral amiotrófica (ALS) durante la nutrición enteral en casa
Janusz Sznajder, Marta Ślefarska-Wasilęwska and Stanisław Kłęk
Nutrimed Nutrition Clinic. Sosnowiec, Poland
ABSTRACT
Aim: Amyotrophic lateral sclerosis (ALS) is a chronic, neurodegenerative disease, which leads to development of malnutrition. The main purpose of this research was to analyze the impact of malnutrition on the course of the disease and long-term survival.
Material and methods: A retrospective analysis has been performed on 48 patients (22 F [45,83%] and 26 M [54,17%], the average age of patients: 66,2 [43-83]) in 2008-2014.The analysis of the initial state of nutrition was measured by body mass index (BMI), nutritional status according to NRS 2002, SGA and concentration of albumin in blood serum.
Patients were divided into two groups, depending on the state of nutrition: well-nourished and malnourished. The groups were created separately for each of these, which allowed an additional comparative analysis of techniques used for the assessment of nutritional status.
Results: Proper state of nutrition was interrelated with longer survival (SGA: 456 vs. 679 days, NRS: 312 vs. 659 vs. 835 days, BMI: respectively, 411, 541, 631 days, results were statistically significant for NRS and BMI). Concentration of albumin was not a prognostic factor, but longer survival was observed when level of albumin was increased during nutritional therapy.
Conclusions: The initial nutrition state and positive response to enteral feeding is associated with better survival among patients with ALS. For this reason, nutritional therapy should be introduced as soon as possible.
Key words: Amyotrophic lateral sclerosis. Malnutrition. Enteral feeding.
RESUMEN
Objetivo: la esclerosis lateral amiotrófica (ELA) es una enfermedad crónica, neurodegenerativa que genera malnutrición. El objetivo principal de este estudio es analizar el impacto de la malnutrición en el curso de la enfermedad y la sobrevida a largo plazo.
Materiales y métodos: se realizó un análisis retrospectivo de 48 pacientes (22 mujeres [45.83%] y 26 hombres [54.17%], con un promedio de edad de 66,2 [43-83]) del 2008 al 2014. El análisis del estado nutricional inicial se midió utilizando el índice de masa corporal (IMC), el estado nutricional de acuerdo al NRS 2002, la valoración global subjetiva (VGS) y la concentración sérica de albúmina. Los pacientes se dividieron en dos grupos, dependiendo del estado nutricional en el que se encontraban: bien nutridos o malnutridos. Los grupos se crearon por separado, lo que permitió un análisis comparativo adicional de las técnicas utilizadas para la evaluación del estado nutricional.
Resultados: un estado nutricional adecuado se relaciona con mayor sobreviva a largo plazo (456 vs. 679 días, NRS 312 vs. 659 vs. 835 días, IMC respectivamente: 41, 541, 631 días, resultados estadísticamente significativos para NRS e IMC). Las concentraciones de albúmina no fueron un factor pronóstico, pero se observó mayor sobrevida si las concentraciones de albúmina incrementaban durante el tratamiento nutricional.
Conclusiones: el estado nutricional inicial y la respuesta positiva a la alimentación enteral están asociados a mayor sobrevida en pacientes con ELA, razón por la cual, la terapia nutricional debe de iniciarse lo antes posible.
Palabras clave: Esclerosis lateral amiotrófica. Desnutrición. Alimentación enteral lateral.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurological disease from the group of neurodegenerative disorders, under which the lower and upper motor nerves are damaged. The cause and etiology of the disease are unknown, only in 5-10% of the cases inheritance has been proven, thereby creating a familiar form of disease (1). An incidence of 7/100 000 level in the general population makes the disease a major social health problem (2). The peak of incidence is located at the age of 64 (3). The average survival time is 2-3 years for the type of the bulbar beginning and 3-5 years for the type of the limb beginning, but one half of patients dies within 30 months after diagnosis (4). At the moment there is no possibility of causal treatment of this disease, which is why in recent years the emphasis has been put on coordinated specialized care. Due to the fact that dysphagia and eating disorders are common symptoms of this disease, nutritional therapy is an essential part of multidisciplinary care. Unfortunately, the role of nutritional therapy is often neglected, and the dietary intervention begins too late and it is carried out carelessly. Many authors emphasize in their works the importance of malnutrition and its correlation with neurological deficits in the course of ALS (5,6). The aim of the study was to answer the question of whether the initial nutritional state has an impact on survival of patients with ALS, and whether nutritional therapy can be an effective therapeutic intervention.
Material and research methods
A retrospective analysis was performed on a group of 48 patients (22 F [45.83%], 26 M [54.17%], age average: 66.2 [43-85]), of patients nutritionally treated because of ALS under home enteral nutrition conditions in the period from 06.01.2008 to 06.01.2014. The average duration of treatment was 594 days (median 511 days, range: 179-1891). Among the 48 patients there were 22 deaths (45.83%) and 26 (54.17%) patients were artificially ventilated. All patients were fed intragastrically with industrial diets. In forty cases (83.4%) the access was a percutaneous endoscopic gastrostomy (PEG) in six (12.3%) a surgical gastrostomy, in two (4.1%) a nasogastric tube. Low-carbohydrate diets were dominating among the industrial diets (28 patients, out of which 6 of them received standard diet, 6 of them diabetic, 4 of them diets with soy protein and 12 of them fiber-rich diets), high-calorie diets were used in 20 patients. The average, daily supply of energy was 1580 kcal (range: 1200-2000). All patients had bulbar component of the disease (34 cases of bulbar form, 14 cases of mixed disease bulbar-limb). The exclusion criteria: nutritional therapy lasting less than 160 days.
The analysis of nutritional status has been performed using body mass index (BMI), Nutritional Risk Screening 2002 (NRS 2002), Subjective Global Assessment (SGA) and the concentration of albumin in blood serum. The primary endpoint of the study was to answer the question whether the nutritional status influence the results of ALS treatment. The secondary endpoint was to determine the effect of nutritional therapy on long-term survival. All tests were performed during admission and after six months of treatment. Groups of patients were divided by:
- SGA: group I - B + D grade (n = 30), group II - C grade (n = 18). No patient was properly nourished.
- NRS 2002: group I - 3 points (n = 6), II - 4 points (n = 30), III - 5 or more (n = 12).
- BMI: BMI < 17 kg/m2 (n = 12), II - 17.01-18.49 kg/m2 (n = 8), III - 18.5-25 kg/m2 (n = 28)
- Concentration of albumin: group I - below the normal range (< 35 g/L, n = 20) and group II - normal concentrations (> 35 g/L, n = 28).
Statistical analysis
The evaluation of interdependence of initial nutritional status and survival of patients was conducted. For this purpose chi-squared test (with the division of survival period into two groups, i.e. the survival period to 360 days and more) was used. The evaluation of the interdependence of initial nutritional status and survival of patients was done. For this purpose χ2 test (chi-squared test) was used, which is introduced in cases where there is a need to assess the independence of the two traits. This test can verify null hypothesis (H0) that two traits are independent of the alternative hypothesis (H1) telling that two traits are dependent.
The test of this hypothesis is statistics χ2 with right-sided critical area. Condition P (χ2 ≥ χα2) = α determines it, where χα2 is the critical value, which was read from the χ2 distribution table for a predetermined confidence level α. If χ2 ≥ χα2 we reject H0 stating that considered traits are dependent. In the opposite case, we find that at a certain confidence level α there are no grounds to reject the null hypothesis H0 talking about traits independence. The calculation has been made with the division of patients into two groups: one for whom the period of survival was 360 days and the other with a longer survival time.
Knowing the χ2 statistics there is a possibility to determine φ-Yule coefficient, which assesses the strength of the relationship between the two traits.
φ = √(χ2/n)
This coefficient is equal to zero when tested traits are independent and their maximum value is 1 denoting a full correlation between the measured traits.
Results
All planned analyses were performed for each patient. The results including the division on diagnostic tests can be found below.
Long-term survival and SGA (Fig. 1)
Group I: the average survival time was 679 days (range 179-1891), median survival was 702 days.
Group II: the average survival time was 456 (range 159 -1084), median survival was 273 days.
Results are shown in figure 1.

The value of the test χ2 (chi-squared): 1.1.
Long-term survival and NRS (Fig. 2)
Group I: average survival time was 835 days (range 702-1075), median survival was 728 days.
Group II: average survival time was 659 days (range 159-1891), median survival was 511 days.
Group III: average survival time was 312 days (range 179-580), median survival was 242 days.
Results are shown in figure 2.
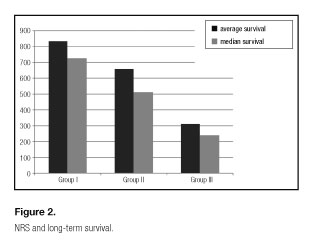
The value of the χ2 (chi-square) test: 7.18.
Long-term survival and BMI (Fig. 3)
Group I: average time of survival was 411 days (range 159-1048), median survival was 242 days.
Group II: average survival time was 541 days (range 179-1069), median survival was 459 days.
Group III: average time of survival was 631 days (range 189-1349), median survival was 607 days.
Results are shown in figure 3.
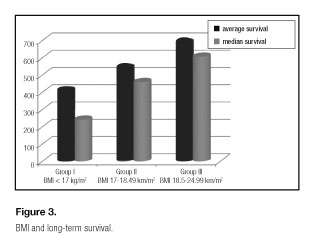
The value of the χ2 (chi-square) test: 4.54.
The determined χ2 test values indicate that there is a correlation between NRS, BMI and survival (χ2 test calculation values are higher than the critical value, and thus we reject the null hypothesis H0 about the independence of the studied traits).
Long-term survival and the initial concentration of albumin blood serum
Group I: average survival - 597 days, median survival - 392 days [183-1091].
Group II: average survival - 592 days, median survival 573 days [159-1349].
In the next stage another analysis was performed to assess the effectiveness of nutritional therapy. Both groups of patients were divided into sub-groups.
Group I: Low baseline concentration of albumin.
A (n = 14) - low initial concentration of albumin but noticeable growth during treatment (average increase: 8,52g/L [range 2.1-18.47]).
B (n = 6) - no increase or decrease of concentration during treatment.
Long-term survival:
A: on average - 717 days, median survival - 511 days.
B: on average - 317 days, median survival - 189 days (183-580).
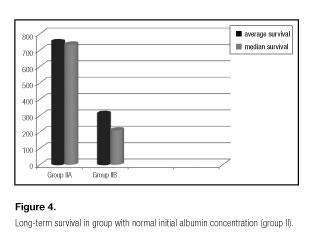
A similar analysis and division into subgroups were made in group II.
A (n = 18, improvement of albumin concentration an average of 8,52g/l [2.1-18.47 range]). Results: average survival - 749 days, median survival - 734 days.
B (n = 10, decrease of albumin concentration an average of 3.08 g/l [range 0.7-6.2 g/l]).
Results (Fig. 4): average survival - 310 days, median survival - 210 days.
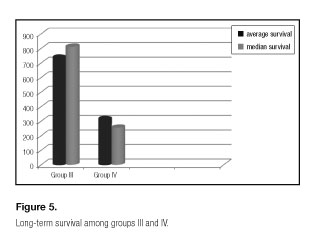
A separate analysis was performed in group III, comprised by IA and IIA subgroups, and in group IV, comprised by IB and IIB subgroups. Analysis of the combined sub-groups IA and IIA, which is the overall assessment of patients with normal concentration of albumin and patients who have succeeded to improve the index over the six months.
Group III consisted of 32 patients. In this group the average survival was 763 days with a median survival of 734 days.
In Group IV patients from IB and IIB groups, i.e. patients with low albumin concentration whose index did not improve in 6 months and patients with normal concentration of albumin which decreased after 6 months, were assessed. In this group, the average survival was 313 days, while the median survival amounted to 200 days.
During the χ2 (chi-squared) test for group III and IV empirical values of the hypothesis χ2e (7.02 and 8.34 respectively) were obtained. They were higher than the theoretical values. This shows that at a significance level of 0.05 (i.e. with 95 % probability) the hypothesis of independence of these traits is needed to be rejected and therefore we can say that there is a correlation between these traits. The coefficients φ-Yule, for these two groups are respectively 0.38 and 0.41 (Fig. 5).
Discussion
ALS is a chronic, incurable disease, during the course of which nutritional status disorders always appear. This is a result of increasing muscle dysfunction associated with chewing and swallowing. In addition, weight loss is associated with the progressive decline of skeletal muscles. Nutritional support should be an important part of treatment for these patients, although it is usually ignored and in most cases introduced too late or not introduced at all. In the literature there are many works emphasizing the important role of medical nutrition therapy in ALS as a component of multidisciplinary care with rehabilitation and ventilation. Bali points out that this can have a significant positive impact on the course of the disease (7).
Malnutrition was found in all patients of described groups. This is consistent with literature data. Lehericey evidenced the prevalence of malnutrition and dehydration on the course of ALS probably against the secondary disorders to degeneration of neurons responsible for the act of swallowing, emphasizing the psychological and ethical aspects of nutritional therapy (8).
In assessing the duration of treatment of patients with ALS in the nutrition clinic it is necessary to remember that the median survival, counted from the date of diagnosis, is 30 months (4), average survival from the date of diagnosis ranges from 2.5 to 3 years. The diagnosis of ALS does not imply that patients begin a treatment in a nutrition clinic. Most patients are admitted to the nutrition clinic when every other method of nutritional treatment has failed.
It has to be noticed that a patient of a clinic should already have the inserted access to the digestive tract -otherwise it causes a delay in the start of nutritional therapy.
In the literature, there are many publications that state that the early inserting of PEG has a positive impact on the nutritional status and disease. Prior-Sanchez assures that faster implementation of PEG in patients with ALS is associated with increased survival (9). Similarly, Eisen A holds that progress in the treatment of ALS is mainly due to the use of the BiPAP and temporal usage of PEG (10).The survival median in ALS -900 days- compared with the results of patients from the groups with the best survival rates, in the light of the fact that patients are taken to nutritional clinics late, may evidence that results could be improved thanks to a faster introduction to nutritional therapy. This is confirmed by data from the literature. ST Ngo confirms that higher initial BMI and its maintenance are associated with an improvement of results (11). Desport thinks that malnutrition is considered as an independent predictor of worsening survival, also he shows that the use of enteral nutrition can improve the condition of the respiratory tract of patients with ALS (12). Furthermore, Lopez Gomez observed positive effects of early placement of patients in the enteral feeding protocol -these patients lived longer in comparison with those in which such protocol was not applied. In the group described above, we can see that patients who began treatment in a better clinical condition and those who had nutritional therapy lived longer. This is shown by each of the indicators under analysis.
Conclusions
1. Patients with ALS who are admitted to treatment in nutrition clinics are a heterogeneous group in terms of their initial nutritional condition. Coefficients of variation reach values above 70%. For example, in both groups classified by the level of SGA coefficients of variation are 71% and 72% respectively, in 4 NRS level and I group BMI they amount up to 77%.
2. Patients with a better initial nutritional status, which is reflected in each of the indicators analyzed -SGA, NRS, BMI- live longer.
3. Basic values of albumin levels are not associated with average lifespan (χ2 = 0.95 level aφ = 0.14). The longest survival prognosticate patients with normal albumin levels, which manage to keep it as it is and patients with basic values of albumin below normal levels, where there is an increase in its concentration in the course of nutritional therapy. Patients with low basic level of albumin survive longer if they are able to modify it during the initial phase of nutritional therapy (highest value χ2 = 8.34 aφ = 0.41 were obtained for the III and IV group).
In short, the initial nutritional status and positive response to enteral feeding is associated with better survival among patients with ALS.
References
1. Anderson PM. Genetic Aspects of Amyotrophic Lateral Sclerosis//Motor Neurone Disease. In: Shaw PJ, Strong MJ, editors. Motor Neuron Disorders. Vol. 28. Philadelphia: Butterworth Heinemann; 2003. p. 207-8. [ Links ]
2. Worms PM. The epidemiology of motor neuron diseases: a review of recent studies. J Neurol Sci 2001; 191:9,6. [ Links ]
3. Abhinav K, Stanton B, Johnston C, et al. Amyotrophic lateral sclerosis in South-East England: a population-based study. The South-East England register for amyotrophic lateral sclerosis (SEALS Registry). Neuroepidemiology 2007;29:44-8. [ Links ]
4. Haverkamp LJ, Appel V, Appel SH. Natural history of amyotrophic lateral sclerosis in a database population. Validation of a scoring system and a model for survival prediction. Brain 1995;118(Pt):707-19. [ Links ]
5. Kubiszewska J, Kwieciński H. Stwardnienie boczne zanikowe. Borgis - Postępy Nauk Medycznych 6/2010, s. 440-8. [ Links ]
6. Vallat JM, Sauterreau D, Couratier P. Nutritional status is a prognostic factor for survival in ALS patients. Neurology 1999;53(5):1059-63. [ Links ]
7. Limousin N, Blasco H, Corcia P, Gordon PH , De Toffol B, Anders C, et al. Malnutrition at the time of diagnosis is associated with a shorter disease duration in ALS. J Neurol Sci 2010;297(1-2):36-9. DOI: 10.1016/j.jns.2010.06.028. [ Links ]
8. Bali T1, Miller TM. Management of amyotrophic lateral sclerosis. Mo Med 2013;110(5):417-21. [ Links ]
9. Lehericey G, Le Forestier N, Meininger V, Pradat PF. Nutritional management in ALS: a medical and ethical stake. Presse Med 2012;41(6 Pt 1):560-74. [ Links ]
10. Prior-Sanchez I, Herrera-Martinez AD, Tenorio Jimenez C, Molina Puerta MJ, Calanas Continente AJ, Manzano Garcia G, et al. Percutaneus endoscopic gastrostomy in amyotrophic lateral sclerosis. Nutr Hosp 2014;3096:1289-94. [ Links ]
11. Eisen A. Amyotrophic lateral sclerosis: a 40-year personal perspective. Clin Neurosci 2009;16(4):505-12. [ Links ]
12. Ngo ST, Steyn FJ, Mc Combe PA. Body mass index and dietary intervention: implications for prognosis of amyotrophic lateral sclerosis. J Neurol Sci 2014;340(1-2):5-12. [ Links ]
13. Desport JC, Preux PM, Truong CT, Courat L, Vallat JM, Couratier P. Nutritional assessment and survival in ALS patients. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;192:91-6. [ Links ]
![]() Correspondence:
Correspondence:
Marta Ślefarska-Wasilęwska.
Nutrimed Nutrition Clinic.
14 Źeromskiego Street 41-205 Sosnowiec, Poland
e-mail: marta8415@interia.pl
Received: 26/09/2015
Accepted: 27/10/2015
