










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkNutrición Hospitalaria
On-line version ISSN 1699-5198Print version ISSN 0212-1611
Nutr. Hosp. vol.33 n.2 Madrid Mar./Apr. 2016
https://dx.doi.org/10.20960/nh.115
TRABAJO ORIGINAL / Epidemiología y dietética
Double burden of malnutrition in rural and urban Guatemalan schoolchildren
Doble carga de malnutrición en escolares urbanos y rurales de Guatemala
José Joaquín Muros1, Mercedes Briones1, Guillermo Rodríguez2, Paula R. Bouzas3, Rafael Giménez1 and Carmen Cabrera-Vique1
1Department of Food Science. School of Pharmacy. University of Granada. Granada. Spain.
2Ibero-American University Foundation (FUNIBER). Ciudad de Guatemala. Guatemala.
3Department of Statistics and Operations Research. School of Pharmacy. University of Granada. Granada, Spain
ABSTRACT
Introduction: Guatemala has been experiencing a lifestyle transition. While chronic malnutrition remains prevalent obesity, has increased substantially.
Objective: The study aimed to provide current information on nutritional status trends in Guatemala.
Methods: A cross-sectional study was conducted in two different regions of Guatemala. A random sample of 392 children and adolescents (aged 5-18 years), stratified by geographical location (rural and urban), sex and age, was selected.
Results: Approximately 62% of the children and adolescents in the urban sample are overweight, whilst 13.8% are obese. Amongst urban participants the prevalence of overweight and obesity was higher in the 5-10 year age group. In the rural sample, the prevalence of overweight was 23.8% with 1.1% obesity. The highest prevalence of overweight and obesity was found in the 11-14 year age group. The urban group shows a higher prevalence of overweight and obesity compared to any of the age categories of the rural group (except in the 15-18 year age group where obesity in the rural group is slightly higer). A significantly higher prevalence of stunting was observed in the rural group than in the urban group, except in 15-18 year age group. Underweight was significantly higher in the 5-10 year age category of the rural group (25 vs. 1.2 %). The prevalence of thinness was also significantly higher in rural areas for all age groups except the 5-10 year age group.
Conclusion: A double burden of malnutrition and a high prevalence of underweight and overweight exist among children and adolescents in Guatemala.
Key words: Double-burden. Malnutrition. Children. Adolescents. Guatemala.
RESUMEN
Introducción: Guatemala ha estado experimentando una transición en sus estilos de vida. Mientras que la desnutrición crónica sigue siendo prevalente, se ha experimentado un aumento sustancial de los casos de obesidad.
Objetivo: proporcionar información actualizada sobre las nuevas tendencias en cuanto al estado nutricional en Guatemala.
Métodos: se diseñó un estudio transversal con una muestra de 392 niños y adolescentes (5-18 años) seleccionados de manera aleatoria. El muestreo fue estratificado según su ubicación geográfica (rural y urbana), sexo y edad.
Resultados: alrededor del 62% de la muestra urbana presentó problemas de sobrepeso y un 13,8 de obesidad. Entre los participantes urbanos, la prevalencia de sobrepeso/obesidad fue mayor en el grupo de 11-14 años. El grupo urbano presentó una mayor prevalencia de sobrepeso/obesidad que el grupo rural para todos los grupos de edad (excepto en el grupo de 15-18 años que presentó unos índices de obesidad ligeramente más elevados en el grupo rural). Se observó una mayor prevalencia de retraso en el crecimiento en el grupo rural, excepto para el grupo de edad de 15-18 años. La prevalencia de bajo peso fue significativamente mayor en el grupo rural (25% vs. 1,2%) así como la prevalencia del delgadez, excepto para el grupo de edad de 5-10 años.
Conclusión: la alta prevalencia de bajo peso y la de sobrepeso/obesidad coexisten en los niños y adolescentes en Guatemala.
Palabras clave: Doble carga. Malnutrición. Niños. Adolescentes. Guatemala.
Introduction
Guatemala is a low-middle income country with large inequalities in nutritional and socio-economic status (1). This country has gone through a nutritional and lifestyle transition. While chronic malnutrition remains prevalent (2) substantial increases in overweight and obesity have taken place in the recent years (3).
An abundance of literature has documented health inequalities between rural and urban children. Studies have shown that children living in urban areas are less likely to suffer stunting or underweight than those living in rural areas (4). However, changes in diet and lifestyle have contributed to change this trend recently. These changes have resulted in the coexistence of both overnutrition (overweight and obesity) with undernutrition (stunting or underweight), which is known as "double burden". This double burden has been observed at national and familiar levels (5).
This double burden is currently taken place in Guatemala (6). While nutritional stunting is still highly prevalent (45.6%) (7), overweight is an emerging public health concern (32.6% and 32.5% in public and private school children, respectively) (8). This has been attributed to the nutritional transition that commonly follows rapid economic transition and urbanization (9), characterized by rapid secular trends of refined, energy-dense and fat foods (10), and a sedentary lifestyle (11).
The aim of our study was to provide current information on nutritional status trends in Guatemala schoolchildren. To such end two groups of subjects from two different geographical populations (rural and urban) were studied through anthropometric assessment. This data will help identify vulnerable groups and facilitate the development of focused nutrition strategies according to the region.
Material and methods
Subjects
A cross-sectional study was conducted in two different regions (rural and urban) of Guatemala. The rural zone was located in Departamento of Izabal and the urban zone was located in the capital city, where children and adolescents from school were evaluated. A random sample of 392 children and adolescents (aged 5-18), stratified by geographical location (rural and urban), sex and age (5-10 years, 11-14 years and 15-18 years), was selected (Table I). In the case of rural participants two groups were studied: boarders (participants enrolled as a boarder in a school) and non-boarders (participants who attend and had a meal but do not live at the school). Urban participants lived and ate at home.

The sample comprised apparently healthy Guatemalan boys and girls, aged 5-18 years, who were not physically handicapped and had no obvious genetic disorders.
All participants took part voluntarily and in accordance with the Declaration of Helsinki regarding ethical research. The bioethical committee for human research of the University of Granada approved the study. Informed consent was also obtained from parents or tutors.
Anthropometric assessments
Guidelines of the International Society for the Advancement of Kinanthropometry (ISAK) (12) were followed. The following instruments were used: GPM Stadiometer (± 1 mm accuracy), Tefal scale (± 50 g accuracy), Holtain skinfold compass (± 1 mm accuracy), Holtain caliper (± 1 mm accuracy) and Holtain flexible metallic metric belt (± 1 mm accuracy). The following measurements were taken: height, weight, skinfolds (triceps, biceps, subscapular, suprailiac, supraspinal, abdominal, thigh, and calf), perimeters (waist, hip, mid-upper arm, flexed and contracted biceps, thigh and calf) and diameters (bicondylar humerus, bistiloid and bicondylar femur). Body mass index (BMI) was calculated from height and weight. We compared the results gathered from the sum of the 8 skinfolds (triceps, biceps, subscapular, suprailiac, supraspinal, abdominal, thigh, and calf) with fat percentage which was calculated using the Slaughter equation (13). The anthropometric status of the participants was determined against the WHO growth reference for those aged 5-18 (14). Cut-off values were: -2 SD for stunting and thinness, 1 SD for overweight and 2 SD for obesity. It was not possible to obtain anthropometric parameters for the 15-18 years age group in urban or rural areas.
Statistical analyses
All anthropometric measurements provided quantitative variables whereas gender, geographical location (rural or urban), status (boarder or non-boarder) and age group (5-10 years, 11-14 years and 15-18 years) provided qualitative variables. Numerical variables were studied as marginal and conditioned to qualitative ones. The analysis was mainly a descriptive analysis by subset regarding the inference. Parametric and non-parametric hypothesis tests were applied to compare multiple variables (significance level α = 0.05). Statistical analysis was performed using Statgraphics Plus package version 5.1, Statistical Graphics Corp. Copyright 1994-1999 and SPSS IBM SPSS Statistics 22.0.
Results
Table I shows the number of participants in the three age strata stratified by sex and geographical location. A final sample of 392 children and adolescents participated in the study. Of the recruited participants, 51.8% were urban and 48.2% were rural. Girls represented 50% of the sample. In addition, 44.9% were children aged between 5 and 10, 31.9% were aged between 11 and 14 and 23.2% were aged between 15 and 18.
Table II shows the anthropometric characteristics of children and adolescents in rural areas stratified by age and status. No significant difference for any parameter was found between boarders and non-boarders of different age groups. However, significantly higher values (p < 0.05) were found between male boarders and non-boarders in average age, height, weight and BMI.
As shown in table III, Guatemalan children and adolescents had negative mean of weight-for-age z-scores (WAZ), height-for-age z-scores (HAZ) and BMI-for-age z-scores (BAZ) irrespective of sex and geographical location with some exceptions. Positive scores for BAZ were obtained in male boarders aged between 5 and 10 and in female boarders aged between 11 and 14. BAZ was positive in boys in the age group 15-18 years in the non-boarder group. The urban group only showed negative mean for HAZ. Urban participants in every category had significantly higher WAZ, HAZ and BAZ than the rural participants (p < 0.05) except in HAZ 15-18 year-old participants. In general, the difference in z-scores between the genders did not reach statistical significance, except for HAZ in 11-14 year-old urban participants. Urban participants in every category had significantly higher WAZ, HAZ and BAZ than the boarder participants (p < 0.05) except in HAZ in 15 to 18 year-old participants. Urban participants in every category had significantly higher WAZ, HAZ and BAZ than non-boarder participants (p < 0.05) except in HAZ in the 5-10 years and 15-18 year age group. No significant differences were found between boarders and non-boarders except for higher HAZ in the age group of non-boarders.

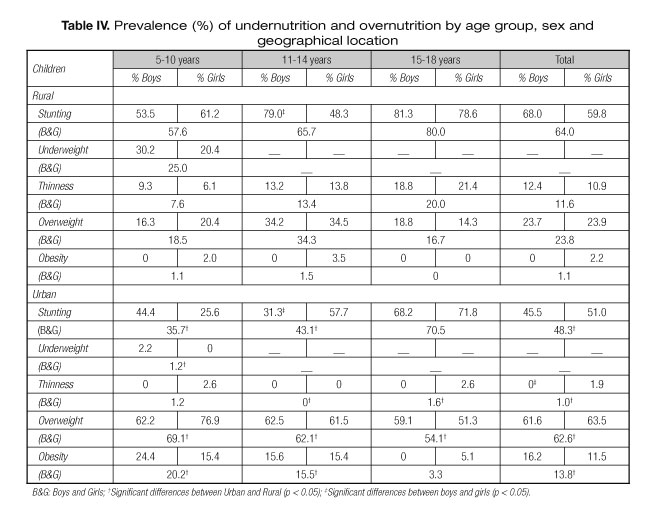
Table IV shows that approximatly 62% of the children and adolescents in our urban sample are overweight, whilst 13.8% are obese. Amongst urban participants the prevalence of overweight and obesity was higher in 5-10 year age group than in the other two groups irrespective of gender. In our rural sample, the prevalence of overweight was 23.8% with 1.1% obesity. The prevalence of overweight and obesity was highest in the 11-14 year age group, again irrespective of gender. The urban group have a higher prevalence of overweight and obesity than the rural group in every age category (except in the 15-18 year age group where obesity is slightly (non-significant) higer in the rural group). A significantly higher prevalence of stunting was observed in the rural group than in the urban group, except in the 15-18 year age group. There were no differences between genders except in the urban 11 to 14 year old group, where there was a higher prevalence in girls. Underweight was significantly higher in the rural group (25 vs. 1.2 %) in the 5-10 year age group. The prevalence of thinness was also significantly higher in rural areas for all age groups except the 5-10 year age group.
Discussion
To the best of our knowledge, this is the first study to report the prevalence and the coexistence of undernutrition and overweight in a sample of Guatemalan schoolchildren. The present study aims to give an overview of the current nutritional status of this population and to enable comparisons between those living in urban and rural areas of Guatemala. The dual burden of malnutrition in children and adolescents in Guatemala shows that undernutrition is more common in rural areas, whereas overnutrition appears to be mainly an urban phenomenon.
Guatemala has the third highest rate of chronic malnutrition (stunting) in the world (54.5%) (15). In some municipalities, particularly in the Western Highlands of the republic, this prevalence can reach 80%. Our study supports previous finding and identifies undernutrition in Guatemala as a severe public health problem that still persists. A recent important longitudinal study which observed Guatemalan children over a period of 40 years (16) suggested increased HAZ scores and a reduction of severe growth retardation. However, there was no long-term change in the prevalence of overweight and obesity. In our study higher age groups demonstrate more stunting than lower age groups. Other studies have shown that indigenous children suffer disproportionately, with rates of stunting almost twice that of non-indigenous children (17). Urbanization, however, has been long recognized as a modifying factor for growth and development in low-income societies (18). Our study showed a higher prevalence of stunting in rural areas (64%) than in urban areas (48.3%). However this rate of stunting is higher than the national percentage of 45.6 %, or the 53.9 and 40.3 % reported in 2008 for total and urban Chimaltenango Guatemalan first grade primary school children (19). Although stunting is a problem that affects the entire Guatemalan population, significant disparity between Guatemala's Ladino and indigenous population groups can be found (20).
Thinness defined as BMI-for-age z-scores, < -2 SD has been adopted to indicate recent nutritional deprivation. In Latin American school-aged children, the prevalence of underweight and thinness is generally lower and less than 10 %. Our study found a range of 11.6% (rural areas) to 1% (urban areas). Underweight and thinness indicates insufficient dietary intake and can inevitably result in adverse health outcomes. Immediate health consequences to school-aged children of being excessively thin include delayed pubertal maturation and reduced muscular strength and work capacity (21).
Childhood obesity is a public health concern which increasingly affects low/middle income countries, with increases of 65% over the past two in low/middle income countries and 48% in high-income countries. Currently 81% (35 million) of affected children live in low/middle income countries (22). While nutritional stunting is still highly prevalent overweight is now becoming a public health concern. Sixty-seven percent of Guatemalans aged 15 and above are overweight, 29% of which are obese (23). We found similar results in urban children and adolescents with a prevalence of 65.6% and 13.8% for overweight and obesity respectively. However, the prevalence in rural participants is lower (23.8% overweight and 1.1% obese). A low percentage of undernutrition (predominantly stunting) and a high percentage of overweight and obesity have been found in urban areas in other Latin American populations (24-26). Overweight and obesity also have a negative impact on health, which includes indicators of metabolic syndrome as well as psychological disturbance (27). The alarming consequence of obesity, among other things, is a greater risk factor for the onset of type 2 diabetes in children (28).
It has been highlighted that cities experience the greatest increase of overweight and obesity because they are much more advanced along the nutritional transition than the countryside (29-30). In urban contexts the range of food choices is greater and prices are generally lower. In addition, urban employments often demand less physical exertion than rural ones, and a greater proportion of women work away from home and are too busy to shop for, prepare and cook healthy meals at home (31).
The simultaneous prevalence of overnutrition (i.e. overweight or obesity) and undernutrition (i.e. stunting) within the same group of children has been previously reported in low/middle income countries (32-35). Both undernutrition and overnutrition during the school age years have detrimental impacts on overall development and on health.
Limitations of the present research are the inclusion of only two geographical regions and relatively small numbers in some subgroups. Due to the cross-sectional nature of the study, we are also unable to reliably assess the causal processes of the double burden of malnutrition. In addition, it was not possible to obtain anthropometric parameters for the 15-18 year age group in urban or rural areas. Finally, the WHO growth reference for those aged 5-18 years does not show values for WAZ in 11-18 year groups.
Conclusions
In conclusion, a double burden of malnutrition exists in children and adolescents in Guatemala. A high prevalence of underweight and overweight exists in school-aged children. Health authorities must develop nutritional and physical activity programs in order to reverse this double burden in Guatemala and other related countries.
References
1. Lee J, Houser RF, Must A, de Fulladolsa PP, Bermudez OI. Socioeconomic disparities and the familial coexistence of child stunting and maternal overweight in Guatemala. Econ Hum Biol 2012;10:232-41. [ Links ]
2. The US Global Health Initiative. Guatemala Strategy 2010. Available at: http://www.ghi.gov/documents/organization/158909.pdf. [ Links ]
3. World Health Organization. Global Database on Body Mass Index 2007. Available at: http://www.who.int/nutgrowthdb/database/en/. [ Links ]
4. Fotso JC. Urban-rural differentials in child malnutrition: Trends and socioeconomic correlates in sub-Saharan Africa. Health Place 2007;13:205-23. [ Links ]
5. Food and Agriculture Organization of the United Nations. The double burden of malnutrition. Case studies from six developing countries. Rome: Food and Agriculture Organization of the United Nations; 2006. p. 97. [ Links ]
6. Halford JC, Boyland EJ, Hughes GM, Stacey L, McKean S, Dovey TM. Beyond-brand effect of television food advertisements on food choice in children: the effects of weight status. Public Health Nutr 2008;11:897-904. [ Links ]
7. Ministerio de Educación Pública. Tercer Censo Nacional de Talla en Escolares de Primer Grado de Primaria de la República de Guatemala. Mineduc; 2009. [ Links ]
8. World Health Organization. Guatemala Global School-Based Student Health Survey 2009. Available at: http://www.who.int/chp/gshs/2009_Guatemala_GSHS_Questionnaire.pdf. [ Links ]
9. Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev 2012;70:3-21. [ Links ]
10. Popkin BM, Gordon-Larsen P. The nutrition transition: worldwide obesity dynamics and their determinants. Int J Obes Relat Metab Disord 2004;28(3):S2-S9. [ Links ]
11. Garrett JL, Ruel MT. Stunted child-overweight mother pairs: Prevalence and association with economic development and urbanization. Food and Nut Bull 2005;26:209-20. [ Links ]
12. Marfell-Jones M, Olds T, Stewart A, Carter L. International standards for anthropometric assessment. ISAK. South Africa: Potchefstroom; 2006. [ Links ]
13. Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Van Loan MD, et al. Skinfolds equations for estimation of body fatness in children and youth. Hum Biol 1988;60:709-23. [ Links ]
14. Onis de M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 2007;85:660-7. [ Links ]
15. UNICEF. The State of the World's Children 2009: maternal and newborn health. New York: UNICEF; 2008. p. 131. [ Links ]
16. Stein AD, Wang M, Digirolamo A, Hoddinott J, Martorell R, Ramirez-Zea M, et al. Height for age increased while body mass index for age remained stable between 1968 and 2007 among Guatemalan children. J Nutr 2009;139:365-9. [ Links ]
17. WHO/PAHO. Malnutrition in Infants and Young Children in Latin America and the Caribbean: Achieving the Millennium Development Goals. 2008. [ Links ]
18. Gross R. Beyond food and nutrition: How can cities be made healthy? Asia Pac J Clin Nutr 2003;11(9):S763-6. [ Links ]
19. Colom IA, Espada R, Ordoñez-de-Molina A, Ortega ME, Álvarez E. Tercer Censo Nacional de Talla en Escolares del Primer Grado de Educación Primaria del Sector Oficial de la República de Guatemala. 2008. Available at: http://siinsan.gob.gt/portals/0/pdf/DesnutricionCronica_TercerCensoTallaEscolares2008.pdf. [ Links ]
20. Disabled World. Height chart of men and women in different countries. 2008. Available at: http://www.disabled-world.com/artman/publish/height-chart.shtml. [ Links ]
21. World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. WHO Technical Report Series no. 854. Geneva: WHO; 1995. [ Links ]
22. Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr 2010;92:1257-64. [ Links ]
23. World Bank. Nutrition at a Glance: Guatemala 2010. Available at: http://siteresources.worldbank.org/INTLACREGTOPNUT/Resources/Guatemala4-20-10.pdf. [ Links ]
24. Cesani MF, Garraza M, Bergel-Sanchís ML, Luis MA, Torres MF, Quintero FA, et al. A Comparative Study on Nutritional Status and Body Composition of Urban and Rural Schoolchildren from Brandsen District (Argentina). PLoS One 2013;8:e52792. [ Links ]
25. De Onis M, Blossner M. Prevalence and trends of overweight among preschool children in developing countries. Am J Clin Nutr 2000;72:1032-9. [ Links ]
26. Barría PMR, Amigo CH. Transición nutricional: una revisión del perfil latinoamericano. ALAN 2006;56:3-11. [ Links ]
27. Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the Third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med 2003;157:821-7. [ Links ]
28. American Diabetes Association. Type 2 diabetes in children and adolescents. Pediatrics 2000;105:671-80. [ Links ]
29. Shetty PS. Nutrition transition in India. PHN 2002;5:175-82. [ Links ]
30. Mendez MA, Popkin BM. Globalization, urbanization, and nutritional change in the developing world. JADE 2005;1:220-41. [ Links ]
31. Food and Agriculture Organization. The nutrition transition and obesity. FOCUS, The developing world's new burden: obesity. 2012. Available at: www.fao.org/FOCUS/E/obesity/obes2.htm. [ Links ]
32. Fernald LC, Neufeld LM. Overweight with concurrent stunting in very young children from rural Mexico: prevalence and associated factors. Eur J Clin Nutr 2007;61(5):623-32. [ Links ]
33. Kimani-Murage EW, Kahn K, Pettifor JM, Tollman SM, Dunger DB, Gomez-Olive XF, et al. The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children. BMC Public Health 2010;10:158. [ Links ]
34. Mamabolo RL, Alberts M, Steyn NP, Delemarre-Van de Waal HA, Levitt NS. Prevalence and determinants of stunting and overweight in 3-year-old black South African children residing in the Central Region of Limpopo Province, South Africa. Public Health Nutr 2005;8(5):501-8. [ Links ]
35. Wang Y, Monteiro C, Popkin BM. Trends of obesity and underweight in older children and adolescents in the United States, Brazil, China, and Russia. Am J Clin Nutr 2002;75(6):971-7. [ Links ]
![]() Correspondence:
Correspondence:
José Joaquín Muros Molina.
Departament of Food Science.
School of Pharmacy.
University of Granada.
18071 Granada, Spain
e-mail: jjmuros@ugr.es
Received: 02/10/2015
Accepted: 31/10/2015
