










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.5 Madrid sep./oct. 2016
https://dx.doi.org/10.20960/nh.564
Cut-off values for classifying active children and adolescents using the Physical Activity Questionnaire: PAQ-C and PAQ-A
Valores de corte para clasificar niños y adolescentes activos utilizando el Cuestionario de Actividad Física: PAQ-C y PAQ-A
Javier Benítez-Porres1, José Ramón Alvero-Cruz2, Luis B. Sardinha3, Iván López-Fernández1 and Elvis A. Carnero1
1Biodynamic and Body Composition Laboratory and 2Exercise Physiology Laboratory. Universidad de Málaga. Málaga, Spain.
3Exercise and Health Laboratory. University of Lisbon. Lisbon, Portugal
This work was supported by the Spanish Ministry of Education, Culture and Sport under Grant AP2010-0583; Spanish Ministry of Economy and Competitiveness under Grant DEP2011-30565; and the University of Málaga (Campus of International Excellence Andalucía Tech).
ABSTRACT
Introduction: The Physical Activity Questionnaire for children and adolescents (PAQ-C & PAQ-A) has been widely used in research and field settings. However, there is a lack of information about its final score meaning.
Objective: To determine PAQ-C and PAQ-A score cut-off values using physical activity (PA) thresholds objectively measured as reference criteria.
Methods: 146 children (n = 83 boys, n = 63 girls) and 234 adolescents (n = 115 boys, n = 119 girls) participated in this study. Accelerometers (Actigraph GT3X) were used to assess objectively PA during one-week, afterwards PAQ was filled by the participants. As participants met or not the international PA recommendations for total, moderate-vigorous (MVPA) or light PA, three categorical variables of two levels were created. ROC curves procedure were carried out to obtain score cut-off points for identifying the positive category recommendation.
Results: ROC curves analysis estimated 2.75 and 2.73 score cut-off points to discriminate > 60 minutes of MVPA for PAQ-A and PAQ-C respectively (PAQ-A AUC = 0.68, p < 0.001 and PAQ-C; AUC = 0.55, p > 0.05). Also 60 minutes of MVPA was achieved with a total volume of 10,664 steps/day in children and 9,701 steps/day in adolescents.
Conclusions: Our results suggest that PAQ-A can be a useful tool to classify adolescents as active or inactive following international recommendations as criteria. However, we could not find a significant cut-off for PAQ-C score.
Key words: ROC curves. Adolescence. Childhood. Sensitivity. Specificity.
RESUMEN
Introducción: el Cuestionario de Actividad Física para Niños y Adolescentes (PAQ-C y PAQ-A) ha sido ampliamente utilizado en entornos de investigación y en el trabajo de campo. Sin embargo, existe una falta de información sobre el significado de su puntuación final.
Objetivo: determinar los valores de corte del PAQ-C y el PAQ-A y el número de pasos diarios asociados utilizando una medida objetiva de actividad física como criterio de referencia.
Metodología: 146 niños (n = 83 niños, n = 63 niñas) y 234 adolescentes (n = 115 niños, n = 119 niñas) participaron en el estudio. Se utilizó acelerometría triaxial (Actigraph GT3X) durante 7 días y los participantes completaron el PAQ-C y/o PAQ-A al entregar el acelerómetro. En base a las recomendaciones internacionales de AF se crearon tres criterios relativos a si los participantes cumplían o no con las mismas (AFMV > 60 min/día, AF vigorosa > 30 min/día, y AF total > 116 min/día; respectivamente). El análisis de las curvas ROC fue utilizado para identificar los valores de corte.
Resultados: el análisis de las curvas ROC estimó un valor de 2,75 y 2,73 para discriminar > 60 minutos de actividad física moderada-vigorosa para el PAQ-A y el PAQ-C, respectivamente (PAQ-A AUC = 0,68, p < 0,001 y PAQ-C; AUC = 0,55, p > 0,05). Dicha intensidad se logró con un volumen total de 10.664 pasos/día en niños y 9.701 pasos/día en adolescentes.
Conclusiones: nuestros resultados sugieren que el PAQ-A puede ser una herramienta útil para clasificar a los adolescentes activos siguiendo las recomendaciones internacionales de actividad física como criterio. Sin embargo, no pudimos encontrar un punto de corte significativo para el PAQ-C.
Palabras clave: Curvas ROC. Adolescencia. Niñez. Sensibilidad. Especificidad.
Introduction
Physical activity (PA) is predictor of cardiovascular (1), skeletal (2), and mental health (3), in children and adolescents. Moreover, PA has been identified as a behavior that may contribute to the prevention of chronic diseases such as obesity, cardiovascular diseases, and metabolic syndrome (4,5). However, current youth, and especially girls, are often not enough active (6).
PA assessment by questionnaires an useful tool in field studies and continue to provide important information to assess activity patterns on large populations PA and they enable a convenient way to assess activity patterns (7). The Physical Activity Questionnaire for children and adolescents (PAQ-C & PAQ-A) are a cost-effective tools to assess PA patterns during childhood and adolescence (8) and they have been widely used in research and field settings. However, a limitation is that the outcome score is not readily interpretable (9). The PAQ asks for frequency spent in physical activities, which is a subjective rating of intensity, moreover their items are scored using ordinal scales (1-5 scale) and the outcome measure is computed as a simple mean of the individual items. As consequence, it is difficult to relate the PAQ score with the established international PA recommendations (10).
Meanwhile, objective measures are often used to validate less accurate measures, such as subjective instruments, but this does not directly improve the accuracy or precision of the self-report instrument. Equivalent estimates of PA could be generate in a more efficient and cost- effective way if we use handle self-report instruments. In this line, the utility in youth can be greatly enhanced by calibrating self-report output against objectively measured PA data. Therefore, although objective instruments are now widely used, there is a considerable need to improve the utility and accuracy of self-report measures.
Triaxial accelerometers provide an objective indicator of free-living PA that can be temporally linked to data from a self-report tool (11), so it is an appropriate method to establish cut-offs points as PA recommended. The most accurate method to measure energy expenditure of PA, such as doubly labelled water or indirect calorimetry are expensive (12) and impractical procedures to achieve this goal. Accelerometry-derived measures are usually expressed as daily min of light, moderate and vigorous physical activity to allow classification of PA according to whether health-related PA guidelines are met. Thus, it would be possible to carry out the meaningful interpretation of PA measurements into active and non-active, because this classification is linked with clinically relevant health outcomes.
In previous studies, various arbitrary PAQ-score cut-off points have been proposed to categorize youth according to their self-reported PA. Ogunleye et al. (13) divided youth as "active" or "low-active" based on an age-sex-specific median split of PAQ scores. Bailey et al. (14) grouped youth into "active," "average" and "inactive" based on age-sex specific PAQ-score quartiles (top, middle two, and bottom quartiles, respectively). Chen et al. (15) assigned PAQ scores ≤ 2 as "low activity," > 2 and ≤ 3 as "moderate activity," and > 3 as "high activity".
As shown, it is a weakness of the PAQ that there is a lack of uniformity and information about the meaning of final score which would differentiate youth active and non-active. Therefore, the aim of this study was to determine PAQ-C and PAQ-A score cut-off values using PA thresholds objectively measured as reference criteria based on international recommendations.
Material and methods
SAMPLE
An invitation to participate in the study was sent to all parents who had their children and adolescents in different schools of primary and secondary education (Málaga, Jaen and Galicia, Spain). Four-hundred and forty potentially eligible subjects responded, and gave their written informed consent after receiving detailed information about the aims and procedures of the study. Subjects with incomplete PA data (n = 18) or technical errors in the instrument (n = 42) were excluded. A final sample of 146 children (n = 83 boys, n = 63 girls) and 234 adolescents (n = 115 boys, n = 119 girls) participated in this study. There were no differences on age and body mass index (BMI) between the excluded participants and the final sample.
The research protocol was reviewed and approved by the Ethics Committee of the Sports Medicine School, at the Faculty of Medicine (Málaga, Spain). The study was developed following the ethical guidelines of the Declaration of Helsinki-Seoul, last modified in 2008.
MEASURES
Body composition
Participant's heights were measured with socks and shoes removed using a stadiometer (SECA Leicester, Birmingham, UK). A Tanita UM-050 digital weighing scale (Tanita UK Ltd, Yiewsley, Middle-sex, UK) was used to measure body mass. Body mass index (BMI; weight/height; kg/m2) was then calculated.
Anthropometric measurements, including skinfolds, height and body mass, were performed by a level 3 certified anthropometrist according to standards for anthropometric assessment of International Society for the Advancement of Kinanthropometry. Fat mass percent (FMP) was calculated using Slaughter's equation (16).
Physical Activity Questionnaire
PA was assessed using the PAQ-C and PAQ-A (17). The PAQ have acceptable reliability and convergent validity (18,19) and the administration and scoring are described below. In brief, the self-administered, 7-day recall questionnaire comprises nine or eight items (PAQ-C includes an additional item on recess), respectively, and collects information on participation in different types of activities and sports (activity checklist), effort during physical education classes, and activity during lunch, after school, evening and at the weekend during the past 7 days. Each item is scored between 1 (low PA) and 5 (very high PA) and the average score denotes the PAQ score. A high score indicates higher levels of PA. The ninth (PAQ-A) and tenth (PAQ-C) item are not used in calculation of the activity score, asks children and adolescents if they were sick or otherwise prevented from engaging in regular PA. Once a value from 1 to 5 for each of the 8-9 items used in the PA composite score is obtained, the mean of these 8-9 items is taken, which results in the final PAQ activity summary score.
Cultural adaptation of the Spanish PAQ was performed following the basic steps of standardized questionnaires cultural adaptation process (20). The original Spanish translation was made by the research team members. Subsequently, two bilingual researchers outside the group performed the reverse translation. The differences between the original version and the translations were reviewed and discussed by the research group and external researchers.
Triaxial accelerometry
The Actigraph GT3X monitor device (Actigraph, Pensacola, FL, USA), was used to assess PA objectively. The accelerometer is lightweight (27 g), compact (3.8 × 3.7 × 1.8 cm) and has a rechargeable lithium polymer battery. It uses a solid-state tri-axial accelerometer to collect motion data on three axes: vertical (Y), horizontal right-left (X) and horizontal front-back axis (Z). The GT3X measures accelerations in the range of 0.05 g to 2 g, which is digitized by a 12-bit analog-to-digital converter at a rate of 30 Hz. Once digitized, the data are filtered using a band-limited frequency of 0.25 to 2.5 Hz. The Actigraph accelerometer has been shown to be a reliable and valid tool for the assessment of different types of physical activities (21).
Researchers distributed pre-initialized accelerometers face-to-face at schools. Participants wore the accelerometers on the right side of the hip, secured with an adjustable elastic belt, underneath clothing, near to the center of gravity. Participants received a demonstration from a trained researcher on how to wear the accelerometer. They were asked to only remove the device when sleeping and engaging in water-based activities. Additionally, children received a brochure about accelerometer use including the instructions. Accelerometers were set to register 1-second epoch cycles, and were programmed to start recording at 12 midnight of the day following they receive the monitor and to record activity for the following 7 days.
The version 6.11.1 of Actilife Software (Actigraph, Pensacola, FL, USA) was used to process the accelerometer data. Periods of ≥ 60 minutes of zero values, allowing for 2 minutes of non-zero interruptions, were defined as accelerometer "non-wear" time and were removed from the analyses. The first day of recording was not included in the analysis. Only participants with ≥ 4 complete days, including one weekend day, were included (22). A day was considered valid if it contained ≥ 10 hours of wear time for weekdays and ≥ 8 hours for weekend days considering different sleep patterns at weekends (23).
We selected the cut points for children from Evenson et al. (24) to determine the time spent on different intensity levels of PA for children: ≤ 100 cpm for sedentary behavior, < 2,296 cpm for light, < 4,012 cpm for moderate, and ≥ 4,012 cpm for vigorous PA. These cut-offs values were subsequently validated for adolescents (25).
A recording of more than 15,000 counts per minute was considered as a potential malfunction of the accelerometer and the value was excluded from the analyses, based on the recommendations from Esliger et al. (26).
PROCEDURE
Each participant received an information sheet and consent form for parents, and were asked to return the forms to their school. Children and adolescents with signed consent forms were subsequently assessed (initial measurements) and received an accelerometer and later eigth-days later completed PAQ-C and/or PAQ-A questionnaire. As much time as necessary time was taken to fully explain the questionnaire and examples were provided. After the trial period, the material and questionnaires were collected by the researcher, and the data was stored in a database for further analysis.
STATISTICAL ANALYSIS
The characteristics of participants were described as mean and standard deviation (SD). A descriptive statistical analysis was performed for all quantitative variables and an analysis of the normal distribution was carried out using the Kolmogorov-Smirnov test. The relationship between the PAQ and minutes of PA from accelerometers was performed using Spearman's rank correlation coefficients (rho).
Based on international recommendations (10) three factors of two levels were developed as participants met or not the PA recommendations and discriminate between "active" and "non-active" youth (MVPA > 60 min/day, vigorous PA > 30min/day, and light PA > 116 min/day; respectively). Receiver operating characteristic (ROC) curves (27) were carried out to identify PAQ-C and PAQ-A score cut-off point for each factor. Accuracy of classification for each set of cut-points was evaluated by calculating weighted statistics, sensitivity, specificity, and area under the receiver operating characteristic curve (AUC). An area of 1 represents perfect classification, whereas an area of 0.5 represents an absence of classification accuracy. ROC-AUC values of > 0.90 are considered excellent, 0.80-0.89 good, 0.70-0.79 fair, and < 0.70 poor (28).
The analyses were performed using SPSS 22.0 (Chicago, Illinois) and MedCalc 14.12.0 (Mariakerke, Belgium) for ROC curves. The level of significance was set at p < 0.05.
Results
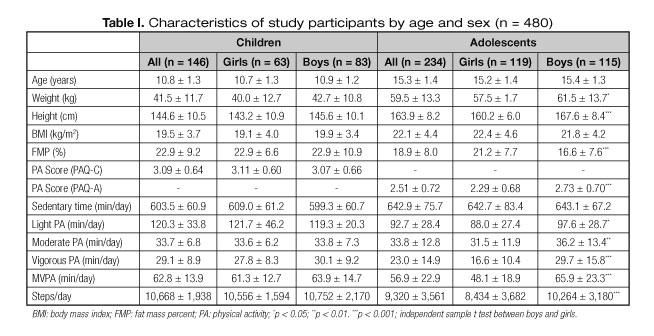
Characteristics of the participants (children and adolescents) for both sex combined and separately are presented in table I. All values are reported as mean and standard deviations (SD). Significant differences between boys and girls were found in adolescents for weight, height, FMP, PAQ-A score, all PA intensities and number of steps, with higher values for boys, except for FMP. No differences between sexes were found in children. 53.4% of children met the 60 minutes of MVPA recommended; while 41.9% of adolescents met this recommendation. PAQ score was positively associated with vigorous PA, MVPA and number of steps (rho = 0.19, rho = 0.17, rho = 0.16, respectively; all p < 0.05) for children. In adolescents, PAQ score was positively associated with all intensities (light, moderate, vigorous and MVPA) and number of steps supplied by the accelerometer (rho = 0.33, rho = 0.21, rho = 0.39, rho = 0.36 rho = 0.41, respectively; p < 0.001).
PHYSICAL ACTIVITY QUESTIONNAIRE FOR CHILDREN (PAQ-C)
Details for AUC, as well as PAQ-C scores and number of steps equivalent to the coordinates with the greatest sum of sensitivity and specificity are shown in tables II and III.

AUC of PAQ-C score for MVPA > 60 min/day, vigorous PA > 30 min/day, and light PA > 116 min/day were no significant (p > 0.05) and only weak (AUC < 0.7) discriminators between "active" and "non-active" individuals. However, AUC of number of steps for all intensities were significant (p < 0.001) and good (AUC > 0.8 for 60 minutes of MVPA) discriminators. ROC analysis showed PAQ-C score cut-off points > 2.75 to discriminate active children. 60 minutes of MVPA in children appears to be achieved, on average, within a total volume of 10,664 steps/day; 30 minutes of vigorous PA within a total volume of 11,038 steps/day; and 116 minutes of light PA within a total volume of 10,190 steps/day. The sensitivity associated with the different factors were moderate for PAQ-C score and steps/day. However, the specificity associated were low for PAQ-C score (42.7%, 41.2% and 43.9%, respectively) and high for steps/day (86.8%, 87.1% and 65.2%, respectively). This shows the low capacity of the PAQ-C to identify inactive children. An example ROC curves is illustrated in figure 1.

PHYSICAL ACTIVITY QUESTIONNAIRE FOR ADOLESCENTS (PAQ-A)
Details coordinates with the greatest sum of sensitivity and specificity are shown for AUC, as well as PAQ-A scores and number of steps equivalent to the in tables IV and V.

AUC of PAQ-A score for all factors were significant (p < 0.01) but only weak (AUC < 0.7) discriminators between "active" and "non-active" youth. AUC of number of steps for all intensities were significant too (p < 0.001) and excellent (AUC > 0.9 for 60 minutes of MVPA) discriminators. ROC analysis showed PAQ-A score cut-off points > 2.73 to discriminate active adolescents. Regarding steps analysis, 60 minutes of MVPA in adolescents appears to be achieved, on average, within a total volume of 9,701 steps/day; 30 minutes of vigorous PA within a total volume of 9,806 steps/day; and 116 minutes of light PA within a total volume of 12,511 steps/day. The sensitivity associated with the different factors were low for PAQ-A score and high for steps/day (except for 116 minutes of light PA). The capacity of the PAQ-A to identify inactive adolescent (specificity) was moderate (77.9%, 75.1% and 68.8%, respectively) and moderate-high for steps/day (93.1%, 77.1% and 68.8%, respectively). An example ROC curves is illustrated in figure 2.

The capacity of number of steps to determine "active" or "inactive" youth was greater than the capacity of the questionnaire score, as observed by the higher positive likelihood rations and lower likelihood negative ratios for all factors. The same applies to positive and negative predictive values, as well as with sensitivity and specificity values (except for sensitivity of PAQ-A for 116 minutes of light PA).
Discussion and conclusions
The present study evaluated the capacity of PAQ-C and PAQ-A to differentiate active and non-active youth based on international PA guidelines. The main finding of this study was that PAQ-A questionnaire could be utilized to discriminate active adolescents (60 minutes of MVPA) using a cut-off point of 2.75. A value for children could not be found for PAQ-C score. Additionally, significant steps/day cut values were found both for children (10,664 steps/day) and adolescents (9,701 steps/day).
To our knowledge, this is the first study to define PAQ-C and PAQ-A cut-points values by accelerometry based on PA recommendations. Details to assess the PAQ-A score as cardiorespiratory fitness parameter have been published for English children. Our results are similar to obtained in the study of Voss et al. (29), in which a cut-off points of 2.9 for boys and 2.7 for girls were established, using cardiorespiratory fitness as the criterion-referenced standard. However, the ROC analysis reported differences between the two questionnaires and these results should be interpreted cautiously.
The sensitivity and the specificity analysis revealed that the PAQ-C cut-points were no able to distinguish the true negatives, but not the true positives. Furthermore, the AUC value indicates that the PAQ-C is unable to discriminate inactive children. In case of PAQ-A cut-off points, which proved sufficiently specificity to discriminate the true negatives but moderately the true positives, manifest an AUC value near to 0.7 (p < 0.001). A diagnostic test that yields an AUC of < 0.7, as observed here, may be deemed unacceptable for clinical use, given the potentially severe repercussions of misclassifying presence or absence of disease. However, the PAQ is not a clinical diagnostic test and comparatively low AUC are often published in a public health context. A plausible explanation for our results could be related with the construct validity of PAQ in Spanish children and adolescents. While the PAQ-A shown reasonable validity for this age range (rho = 0.39; p < 0.001) (30); the PAQ-C shown a questionable validity (rho = 0.28, p < 0.05) for assessing total PA and MVPA in Spanish children (31). Our correlation results between both instruments also concur with the line of evidence that suggests PA questionnaires for adolescents correlated better with accelerometer results than PA questionnaires for children (7).
Moreover, discrepancies and high variability in children's PA measured by accelerometers have been reported around the world, which may introduce a bias in this study (32). The output from accelerometers is a dimensionless unit commonly referred to as accelerometer counts. Researchers have attempted to calibrate these counts with energy expenditure in order to get a biological meaning to the output (33). This has resulted in the publication of count thresholds relating to various categories of energy expenditure, that allow researchers to summarize time spent in a given intensity of activity (34). The availability of multiple cut points or equations has led to much confusion in the accelerometer literature (35). We used the Evenson et al. (24) cut points, recommended in Trost et al. (25) comparative study to estimate time spent in sedentary, light-, moderate-, and vigorous-intensity activity in children and adolescents. Other cut points would have yielded different results. Nonetheless, the associations and differences with total PA will continue to be same since this variable must not be highly dependent of cut-off values.
Conversely, the discriminative power of steps/day was excellent, as evidenced by the high AUC values (near of 0.9 for PAQ-C and > 0.9 for PAQ-A). The AUC provides an estimate of the "goodness" of a diagnostic test, whereby a theoretical perfect test with 100% specificity and 100% sensitivity yields an AUC of 1, and a non-discriminating test an AUC of 0.5. Sensitivity and specificity obtained were 78.2% (95% CI 67.4 to 86.8), 86.8% (95% CI 76.4 to 93.8) for 60 minutes of MVPA in children; and 86.6% (95% CI 78.2 to 92.7), 93.1% (95% CI 87.3 - 96.8) for 60 minutes of MVPA in adolescents. The cut-off points associated were 10,664 steps/day for children and 9,701 steps/day for adolescents. These values are similar to those reviewed by Tudor-Locke (36). These aspects are of interest for public health since they corroborate the insights into PA needs and recommendations for children and adolescents that may be used to evaluate scholar population and implement intervention strategies by healthcare workers and physical education teachers. In addition, quantifying PA, with a low-cost way, will be helpful in order to focus school and community interventions on youth with unhealthy lifestyles.
The specific criteria used to categorize individuals as meeting or not meeting PA recommendations were selected based on WHO guidelines (10). Recent studies indicate the need to increase the recommendation of MVPA. Thus, Jiménez-Pavón et al. (37) recommend around 60 and 85 min/day of MVPA, including 20 min/day of vigorous PA. On the other hand, data from the European Youth Heart Study with objectively measured PA suggest 90 minutes of MVPA based on metabolic health and the metabolic syndrome (4). Similarly, the criteria applied in this study (MVPA > 60 min/day, vigorous PA > 30min/day, and light PA > 116 min/day) are in agreement with the proposed guidelines, but our approach support the hypothesis that 60 min or more of MVPA could be enough, if enough vigorous PA is accumulated during such period (at least 30 minutes).
Limitations
This study has several limitations that should be considered. First, subjectivity and limited recall ability are known limitations of self-reported PA, particularly in young people (38). Limitations of self-reports items include the tendency for people to report socially desirable responses. Moreover, although objective measures of PA, such as triaxial accelerometry or heart rate monitors are ideal, even these methods have their limitations, and this practice has been criticized due to the fact that accelerometers and self-report instruments measure different things (39). Other limitations could explain our results and the capacity of discrimination. For example, our sample size was relatively small but significant for the purpose of study. However, these results should be verified in larger samples.
Conclusions
In summary, our findings provide normative PAQ scores for adolescents. According with the ROC analysis, our results suggest that PAQ-A can be a useful tool to classify adolescents as active or inactive following international recommendations as criteria. It seems, that a 2.75 score can be used to detect adolescents performing enough PA. However, this does not apply to the PAQ-C, which might not be an adequate tool to classify children as active or inactive.
These cut-off points can be useful and a cost-economic way to evaluate scholar population and implement intervention strategies. However, as far as possible, we suggest, in accordance with recent studies (40), the use of a combination of objective and subjective assessment methods.
References
1. Andersen LB, Riddoch C, Kriemler S, Hills A. Physical activity and cardiovascular risk factors in children. Brit J Sport Med 2011;45(11):871-6. [ Links ]
2. Julián-Almarcegui C, Gómez-Cabello A, Huybrechts I, González-Aguero A, Kaufman JM, Casajus JA, et al. Combined effects of interaction between physical activity and nutrition on bone health in children and adolescents: a systematic review. Nutrition reviews 2015;73(3):127-39. [ Links ]
3. Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med 2011;45(11):886-95. [ Links ]
4. Andersen LB, Harro M, Sardinha LB, Froberg K, Ekelund U, Brage S, et al. Physical activity and clustered cardiovascular risk in children: a cross-sectional study (The European Youth Heart Study). Lancet 2006;368(9532):299-304. [ Links ]
5. Cordova A, Villa G, Sureda A, Rodríguez-Marroyo JA, Sánchez-Colladoe MP. Physical Activity and Cardiovascular Risk Factors in Spanish Children Aged 11-13 Years. Rev Esp Cardiol 2012;65(7):620-6. [ Links ]
6. Alonso-Fernández N, Jiménez-García R, Alonso-Fernández L, Hernández-Barrera V, Palacios-Cena D. Health factors related to physical activity among children and adolescents: Results from Spanish National Health Surveys 2006 and 2011/12. Journal for specialists in pediatric nursing: JSPN 2015;20(3):193-202. [ Links ]
7. Chinapaw MJM, Mokkink LB, Van Poppel MNM, van Mechelen W, Terwee CB. Physical Activity Questionnaires for Youth A Systematic Review of Measurement Properties. Sports Med 2010;40(7):539-63. [ Links ]
8. Janz KF, Lutuchy EM, Wenthe P, Levy SM. Measuring activity in children and adolescents using self-report: PAQ-C and PAQ-A. Med Sci Sport Exer 2008;40(4):767-72. [ Links ]
9. Biddle SJH, Gorely T, Pearson N, Bull FC. An assessment of self-reported physical activity instruments in young people for population surveillance: Project ALPHA. Int J Behav Nutr Phy 2011;8. [ Links ]
10. WHO. Global Recommendations on Physical Activity for Health. WHO Guidelines Approved by the Guidelines Review Committee. Switzerland; 2010. p. 58. [ Links ]
11. Vanhelst J, Hardy L, Gottrand F, Beghin L. Technical aspects and relevance of physical activity assessment in children and adolescents in free-living conditions. Arch Pediatrie 2012;19(11):1219-25. [ Links ]
12. Sirard JR, Pate RR. Physical activity assessment in children and adolescents. Sports Med. 2001;31(6):439-54. [ Links ]
13. Ogunleye AA, Voss C, Sandercock GR. Prevalence of high screen time in English youth: association with deprivation and physical activity. Journal of public health 2012;34(1):46-53. [ Links ]
14. Bailey DA, McKay HA, Mirwald RL, Crocker PR, Faulkner RA. A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: the university of Saskatchewan bone mineral accrual study. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research 1999;14(10):1672-9. [ Links ]
15. Chen SR, Lee YJ, Chiu HW, Jeng C. Impact of physical activity on heart rate variability in children with type 1 diabetes. Child's nervous system: ChNS: official journal of the International Society for Pediatric Neurosurgery 2008;24(6):741-7. [ Links ]
16. Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Vanloan MD, et al. Skinfold Equations for Estimation of Body Fatness in Children and Youth. Human Biology 1988;60(5):709-23. [ Links ]
17. Crocker PRE, Bailey DA, Faulkner RA, Kowalski KC, McGrath R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med Sci Sport Exer 1997;29(10):1344-9. [ Links ]
18. Kowalski KC, Crocker PRE, Faulkner RA. Validation of the physical activity questionnaire for older children. Pediatr Exerc Sci 1997;9(2):174-86. [ Links ]
19. Kowalski KC, Crocker PRE, Kowalski NP. Convergent validity of the physical activity questionnaire for adolescents. Pediatr Exerc Sci 1997;9(4):342-52. [ Links ]
20. Geisinger KF. Cross-cultural normative assessment: Translation and adaptation issues influencing the normative interpretation of assessment instruments. Psychological Assessment 1994;6(4):304-12. [ Links ]
21. Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport 2011;14(5):411-6. [ Links ]
22. Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40(1):181-8. [ Links ]
23. Yildirim M, Verloigne M, de Bourdeaudhuij I, Androutsos O, Manios Y, Felso R, et al. Study protocol of physical activity and sedentary behaviour measurement among schoolchildren by accelerometry-cross-sectional survey as part of the ENERGY-project. BMC public health 2011;11:182. [ Links ]
24. Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sport Sci 2008;26(14):1557-65. [ Links ]
25. Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc 2011;43(7):1360-8. [ Links ]
26. Esliger DW, Copeland JL, Barnes JD, Tremblay MS. Standardizing and Optimizing the Use of Accelerometer Data for Free-Living Physical Activity Monitoring. J Phys Act Health 2005;2(3):366-83. [ Links ]
27. Zweig MH, Campbell G. Receiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicine. Clinical chemistry 1993;39(4):561-77. [ Links ]
28. Metz CE. Basic principles of ROC analysis. Seminars in nuclear medicine 1978;8(4):283-98. [ Links ]
29. Voss C, Ogunleye AA, Sandercock GRH. Physical Activity Questionnaire for children and adolescents: English norms and cut-off points. Pediatr Int 2013;55(4):498-507. [ Links ]
30. Martínez-Gómez D, Martínez de Haro V, Pozo T, Welk GJ, Villagra A, Calle ME, et al. (Reliability and validity of the PAQ-A questionnaire to assess physical activity in Spanish adolescents). Revista espanola de salud publica 2009;83(3):427-39. [ Links ]
31. Benítez-Porres J, López-Fernández I, Raya JF, Álvarez Carnero S, Alvero-Cruz JR, Álvarez Carnero E. Reliability and validity of the paq-c questionnaire to assess physical activity in children. J School Health 2016;86:677-85. [ Links ]
32. Guinhouya BC, Samouda H, de Beaufort C. Level of physical activity among children and adolescents in Europe: a review of physical activity assessed objectively by accelerometry. Public health 2013;127(4):301-11. [ Links ]
33. Freedson P, Pober D, Janz KF. Calibration of accelerometer output for children. Med Sci Sport Exer 2005;37(11):S523-S30. [ Links ]
34. Rowlands AV. Accelerometer assessment of physical activity in children: An update. Pediatr Exerc Sci 2007;19(3):252-66. [ Links ]
35. Welk GJ, McClain J, Ainsworth BE. Protocols for Evaluating Equivalency of Accelerometry-Based Activity Monitors. Med Sci Sport Exer 2012;44:S39-S49. [ Links ]
36. Tudor-Locke C, Craig CL, Beets MW, Belton S, Cardon GM, Duncan S, et al. How Many Steps/Day are Enough? for Children and Adolescents. Int J Behav Nutr Phy 2011;8. [ Links ]
37. Jiménez-Pavón D, Konstabel K, Bergman P, Ahrens W, Pohlabeln H, Hadjigeorgiou C, et al. Physical activity and clustered cardiovascular disease risk factors in young children: a cross-sectional study (the IDEFICS study). BMC medicine 2013;11:172. [ Links ]
38. Warren JM, Ekelund U, Besson H, Mezzani A, Geladas N, Vanhees L, et al. Assessment of physical activity - a review of methodologies with reference to epidemiological research: a report of the exercise physiology section of the European Association of Cardiovascular Prevention and Rehabilitation. European journal of cardiovascular prevention and rehabilitation: official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology 2010;17(2):127-39. [ Links ]
39. Ham SA, Reis JP, Strath SJ, Dubose KD, Ainsworth BE. Discrepancies between methods of identifying objectively determined physical activity. Med Sci Sport Exer 2007;39(1):52-8. [ Links ]
40. Steene-Johannessen J, Anderssen SA, van der Ploeg HP, Hendriksen IJ, Donnelly AE, Brage S, et al. Are Self-Report Measures Able to Define Individuals as Physically Active or Inactive? Med Sci Sports Exerc 2015. [ Links ]
![]() Correspondence:
Correspondence:
Javier Benítez Porres.
Department of Didactics of Languages, Arts and Sport.
Faculty of Educational Sciences.
University of Málaga.
Bulevar Louis Pasteur, 25.
Campus de Teatinos.
29010 Málaga. Spain
e-mail: benitez@uma.es
Received: 07/12/2015
Accepted: 26/02/2016
