










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 no.5 Madrid sep./oct. 2016
https://dx.doi.org/10.20960/nh.586
Interventions directed at eating habits and physical activity using the Transtheoretical Model: a systematic review
Intervenciones dirigidas a los hábitos alimenticios y la actividad física mediante el Modelo Transteórico: una revisión sistemática
Mariana Carvalho de Menezes1, Lydiane Bragunci Bedeschi1, Luana Caroline dos Santos2 and Aline Cristine Souza Lopes2
1Postgraduate Program in Nursing and 2Department of Nutrition. Research Group in Nutrition Interventions of University of Minas Gerais. Universidade Federal de Minas Gerais. Minas Gerais, Brazil
This work was supported by the Pró-Reitoria de Pesquisa of Universidade Federal de Minas Gerais which provided financial aid to the translation of this manuscript into English language.
ABSTRACT
Introduction: The multi-behavioral Transtheoretical Model (TTM) addresses multiple behaviors and it is a promising strategy to control multifactorial morbidities, such as chronic diseases. The results obtained using the TTM are positive, but are not consistently methodical.
Objectives: The aim of this study was to systematically review the effectiveness of the Transtheoretical Model in multi-behavioral interventions for changing eating habits and levels of physical activity.
Methods: A search on PubMed and SciELO databases was performed with inclusion criteria set for intervention studies before 2016 using the Transtheoretical Model for more than one behavior, including eating habits and/or engaging in physical activity.
Results and conclusion: Eighteen studies were identified; there was a predominance of randomized clinical trials, studies conducted in the United States, and the use of the Internet and/or telephone. The selected studies were aimed at changing eating behaviors; five of the studies did not address physical activity. The main results were reduction of fat consumption, an increase in the consumption of fruit and vegetables, and increases in physical activity, which are progressions in the stages of change and weight loss identified by the Transtheoretical Model. However, the studies showed methodological weaknesses, including high participant loss and the omission of information about randomization and blinding.
Key words: Theoretical models. Food habits. Exercise. Intervention studies. Review.
RESUMEN
Introducción: el Modelo Tranteórico multiconductual aborda distintas conductas y es una estrategia prometedora para el abordaje de patologías multifactoriales, sobre todo en las enfermedades crónicas. Los resultados iniciales de su empleo han sido favorables, pero no han sido probados con rigor.
Objetivos: el objetivo de este estudio fue realizar una revisión sistemática de la eficacia del Modelo Transteórico en el cambio de hábitos dietéticos y en el grado de actividad física con intervenciones en varias áreas de la conducta.
Métodos: se realizó una búsqueda en PubMed y SCieLO utilizando como criterios de búsqueda estudios de intervención realizados antes de 2016 y que incluyeran más de un hábito, incluyendo hábitos alimentarios y/o actividad física.
Resultados y conclusión: se identificaron 18 estudios, con un predominio de ensayos clínicos aleatorizados, estudios realizaos en Estados Unidos de Norteamérica, y uso de Internet y/o teléfono. Los estudios seleccionados tenían como meta el cambio en los hábitos dietéticos. En 5 de los estudios no se incluía la actividad física. El principal resultado de la intervención fue la disminución en el consumo de grasa y el aumento en la ingestión de frutas y verduras, así como un aumento en la actividad física. Estos cambios supusieron progresos en la pérdida de peso. Sin embargo, los trabajos eran metodológicamente débiles, incluyendo una alta tasa de abandonos, y falta de información sobre la aleatorización y cómo se realizó el estudio ciego.
Palabras clave: Modelos Teóricos. Hábitos alimenticios. Ejercicio. Estudios de intervención. Revisión.
Introduction
The Transtheoretical Model (TTM) is used in developing and monitoring the effectiveness of health interventions in research and health service contexts. This study focused on the multi-behavioral TTM because it addresses multiple behaviors, which makes it a promising strategy to control multifactorial morbidities, such as chronic diseases (1).
The main pillars of TTM encompass the stages of change (SC), decisional balance, self-efficacy, and processes of change. The SC represents the motivation and promptness of change (2), and progression is mediated by the other components. Decisional balance involves the individual's perception of the advantages and disadvantages of modifying the targeted behaviors and self-efficacy, which is defined as the confidence in the ability to adopt new behaviors. The processes of change comprise cognitive, experimental, and behavioral strategies that encourage the progression across stages (3).
The results obtained using the TTM are positive, but are not consistently methodical. The present work systematically reviewed the effectiveness of the TTM in multi-behavioral interventions for changing eating habits and levels of physical activity.
Methods
This review was conducted based on the recommendations of the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guide. The following steps were undertaken in this study: The hypothesis and aims of the study were defined, the criteria for inclusion and exclusion of articles was established, bibliographical research was conducted, the material was carefully read, the information to be obtained from the articles was defined, and the methods of analyzing and presenting the results were established.
The bibliographical research was performed with the purpose of answering the following question: Has the multi -behavioral change-eating habits and physical activity- using the TTM been effective? The databases of the United States National Library of Medicine (PubMed) and The Scientific Electronic Library Online (SciELO) were used. The keywords used (in Portuguese and in English) included (1) use of the Transtheoretical Model ("stages of change", "stage of change", "transtheoretical model", "transtheoretical model of change"); (2) addressing more than one multiple behavior interventions", "multiple behavior changes"); and (3) inclusion of the eating behaviors and/or physical activity in the intervention ("dietary therapy", "eating habits", "physical activity", "diet and exercise").
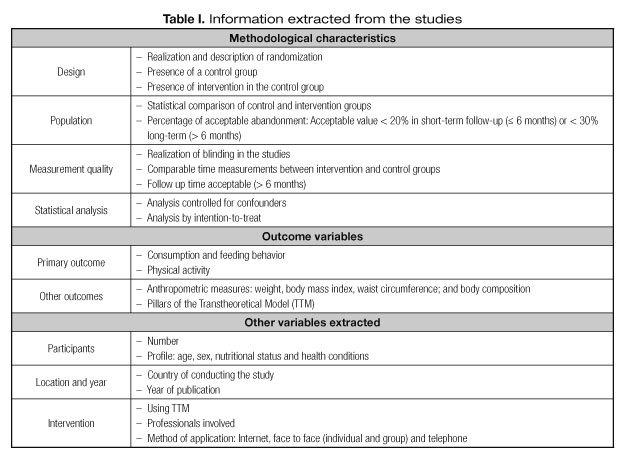
All articles published before 2016 were identified, followed by an analysis of their titles, and an analysis of abstracts and full texts. When the title and the abstract met the established criteria, the selected articles were read in full (Table I) (4). Moreover, the articles referenced in this work and additional available publications were recovered using the same inclusion criteria.
To verify agreement on the selection of articles to be analyzed in this review, two authors applied the proposed inclusion criteria in an independent and blinded manner. The kappa test was used to measure the concordance between the evaluators. In case of discordance, there was a discussion and a consensus was proposed and, when necessary, the other authors of this work were consulted. The articles associated with an unique study were analyzed separately, but referenced in the text according to the first publication.
Results
STUDY SELECTION
The database SciELO did not have any articles containing the multi-behavioral TTM; therefore, only articles found in the PubMed database were analyzed.
The independent evaluators reached an initial consensus over the selection of 78.8% of the articles (kappa test: 0.697). The discordance generated resulted mainly from the incomplete description of the methodology in the abstracts.
Figure 1 presents the flowchart used to select the articles. Eighteen studies met the eligibility criteria and were included in this review. The 18 studies evaluated generated 23 publications: Johnson et al. (5); Cook et al. (6), Prochaska et al. (7-9), Logue et al. (10), Jones et al. (11), Svetkey et al. (12) and Elmer et al. (13) (Premier Study), Block et al. (14) and Sternfeld et al. (15) (Alive! Study), Clark et al. (1), Greaney et al. (16) and Greene et al. (17) (SENIOR study), Riebe et al. (18,19), Steptoe et al. (20,21), Van Wier et al. (22,23) (ALIFE@Work study), Niederhauser et al. (24) (Building Strong and Ready Families Program), Mauriello et al. (25), Velicer et al. (26), Armitage et al. (27), Menezes et al. (28) (Table II).

METHODOLOGICAL CHARACTERISTICS OF THE STUDIES
From the 18 analyzed studies, 14 were conducted in the United States of America, two in the United Kingdom (20,27), one in Brazil (28) and one in Canada (11).
The sample size in the studies varied from 71 to 5,407 (avera-ge = 1,349) participants, and included male and female participants. The average age ranged from 25, 8 to 75 years, with the exception of two studies which samples were composed by preadolescents (26) and adolescents (25) (Table II).
The main inclusion criterion for the studies was the presence of an aggravating factor, such as overweight (9,10,18,20,22,27), high blood pressure (12), increased risk of cardiovascular diseases (20), and diabetes mellitus (11).
The predominant design was the randomized clinical trial (5-12,14,20,22,26,28), but studies of interventions without a control group (CG) (18,26), an experimental (1) and quasi-experimental (24) group were also identified. Only 8 studies clearly described the randomization method used (10,12,14,20,22,26-28).
From the 16 studies that had a CG, 31 % (n = 5) did not conduct an intervention. The treatment of the CG was generally defined as "usual care" (1,6,7,10-12,20,22, 8), and only five studies (7,10,12,27,28) described the intensity and type of care.
In the majority of the studies, the comparability of the control and intervention groups (IG) was tested on the baseline values (1,6-12,14,20,24,25,27,28) for demographical and socio-economic variables, among others, with the exception of two studies (5,22). In the study of Van Wier et al. (22,23), the groups were not statistically compared before the intervention, although all the analyses were adjusted by baseline values, which created an adjusted follow-up score.
Most of the trials had a follow-up period of six months or longer (4), varying between one (27) and 36 months (26). Some studies presented participant losses considered acceptable over the short- (≤ 6 months) (6,12,27) and long-term (> 6 months) (5,8,11,12,26); one study did not give the loss information. We found losses ranging between 11,1% (27) and 63% (24) in the short-term studies and between 17,3% (26) and 46% (5) in the long-term studies. In general, these losses were lower in the CG.
All studies evaluated the CG and IG (intervention group) at comparable time points, and additional analyses were performed only with the IG; in some studies, this was done for supporting the intervention (8,11).
Seven investigations (39%) did not mention whether the researchers or the participants were blind to status (1,5,7,11,20,22,24), and the reason given was the nature of the interventions (18,20) or the presence of research assistants, who were not blind to the group assignment, during assessments (25,26). The remaining studies explained how blind analyses were performed or the data collection was carried out using self-report questionnaires without the involvement of the researcher (6,8,10,12,14,27,28).
Regarding the statistical analysis of the data, the majority of the studies controlled by potential confounding factors in -intention-to-treat analyses (1,5,10-12,14,20,22,25,26). In addition, Prochaska et al. (7,8) used the Generalized Linear Model, a method that allows the evaluation of a changing pattern across time, in addition to performing modeling and evaluation of missing data.
For the evaluation of the main outcomes, the studies used Food Frequency Questionnaires (11,14,17,22), 24 hours Food Records (R24) (10,13,17,18,28) and general questionnaires concerning eating habits and behaviors (6-8,14,25,26,28) to evaluate food consumption. R24 were administered face-to-face, via telephone or computer, two (13) or three (10,17,18,28) times at each -evaluation time-point. However, only one study included the consumption of micronutrients (13), while the others limited the analysis to the consumption of calories, lipids, and food groups, including fruit and vegetables (FV).
Concerning the practice of physical activity (PA), the studies applied distinct questionnaires in which the participants reported the duration and/or frequency of the activity (14,16,19,20,22,24-26). A seven-day PA (physical activity) Recall to estimate the daily energy expenditure (10,13), an ergometric test to evaluate the cardiac frequency or maximum oxygen consumption (13,19), a measure of the functional mobility in the elderly (16), monitoring of PA with a pedometer (23) were among the measures used.
Regarding other outcomes investigated, thirteen studies obtained anthropometric data (10,12,18,20,22,27,28) or used self-reported anthropometric information (5,6,9,11,22,24,25). Weight was the most frequently used measurement, and some studies also included Body Mass Index (BMI) (18,19,24,25,27,28), waist circumference (WC) (10,22,28), and body fat percentage (BF %) (19).
Some studies failed to report which questionnaire was used for evaluating the TTM pillar stages of change (6,14) and only a few described the validation of this tool (5,25,26,28). The remaining TTM pillars (processes of change, decisional balance and self-efficacy) were used to monitor the results in only a few interventions (1,6,14,19,22).
INTERVENTIONS AND THE TRANSTHEORETICAL MODEL
The application methods for the intervention included online platforms, e-mails, phone calls (1,5-11, 14,22,25,26) and group (12,18,28) and individual (9,20) face-to-face meetings.
The professionals engaged in the development and execution of the interventions included nutritionists (10,12,18,22,28), health educators (12,20), health coaches (9), psychologists (10,18,20,28), nurses (20,24), chaplains (24), and physical education teachers (22), or advisors (10,11); seven studies did not report who developed or performed the intervention (1,5,7,8, 25-27). The training of these professionals was mentioned in six of the studies (9,10,12,20,22,28).
The TTM was used as an aid to classify the SC of the participants and assess the intervention (22), as an intervention tool (10,12), or both (1,5-9,11,14,18,20,24-26,28). As an example, in the ALIFE@Work study (22) (performed with overweight workers) the advice related to PA was based on the stages of change, while the advice related to healthy eating habits was based on self-reports of food consumption.
Some interventions were exclusively based on the TTM (1,5,7,8,10,11,18,20,25-28), while others (6,12,14,22) used it in combination with other elements derived from behavioral and cognitive psychology or other theories (9,24).
INTERVENTION EVOLUTION: EATING HABITS AND PHYSICAL ACTIVITY
Almost all the studies addressed healthy eating habits (HEH), and thirteen studies included advice on the increasing PA (1,5,6,9,10,12,14,18,20,22,24-26). Interventions focusing on eating habits were particularly aimed at reducing the ingestion of fat and increasing the consumption of FV, which was explicitly addressed in 72% and 38% of the studies, respectively. Others monitored behaviors, including controlling the size of food portions (10), and reducing calories (5,22,28), sodium (13), alcohol (13, 22) and sugar (14, 22) (Table II).
Among the changes in eating habits, significant reductions were observed in the consumption of total fat (11,13,20,22), saturated fat (13,14,19) trans fat (14), calories (10,13,19,28), sodium (13) and cholesterol (12); there was an increase in the ingestion of FV (7,8,11,13,14,17,25,26), vitamins, minerals and fibers (13) (Table II).
Positive changes in behavior, such as increased intention, motivation and attitudes to achieve HEH (6), and increased substitution of food with high-fat content for low-fat content, were reported. Reduction in the frequency and quantity of high-fat products and changes in the way the food is prepared (7,8,28) were also observed (Table II).
Some studies documented negative changes in eating habits, such as reduced consumption of FV after 24 months (13) or no alterations after the intervention in the ingestion of sugar (14) and FV (23) (Table II).
The evolution of physical activity was evaluated primarily by the increase in frequency or duration (9,10,14,19,20,22,25,26), whereas the type and intensity of the activities were less explored.
The work of Johnson et al. (5) and Cook et al. (6), although including interventions for PA and HEH, did not include the analyses of the evolution in PA frequency and duration (5,6) or in consumption or eating habits (5) (Table II).
As a consequence of alterations in the eating habits and in the practice of physical activity, eight short- and long-term studies showed weight reduction among members of the IG (5,13,19,22,27,28) and CG (6,9, 27), as well as reductions in their WC (10,22), BF % and BMI (19,28) (Table II).
All the studies that evaluated the evolution of the SC reported positive results, and the patients progressed to the stages of action and maintenance (5-8,11,14,16,19,21,24-26) (Table II). Block et al. (14) was the only study that did not find an evolution in the ingestion of fat, despite the positive results for other eating habits.
Discussion
The multi-behavioral TTM is a promising strategy for the promotion of healthy lifestyles, and positive results for multiple behaviors in various scenarios have been reported (1,7,29,30). However, methodological differences among the studies persist, which hinders the demonstration of their effectiveness and their use in theoretical and practical applications.
The positive points of the analyzed studies include the use of randomized clinical trials, which is an appropriate methodology to assess the effects of an intervention; large sample sizes; long-term follow-up; and suitability of the statistical analyses. Consequently, the majority of the studies found a significant evolution in the stages of action and maintenance in the participants, in addition to changes in the behaviors associated with HEH and PA, with significant differences among the intervention and control groups.
Nevertheless, the studies also had methodological weaknesses, such as participant loss and omission of information concerning randomization and blinding. Most of the studies reported the intervention delivered to the CG participants, although the intensity of the intervention was not reported. Logue et al. (10) verified that, at baseline, 83% of the CG participants reported being advised by a physician to lose weight and 48% had previous experience with commercial programs for weight loss. In some studies, individuals of the CG evolved positively in their eating habits, levels of physical activity, and body weight, possibly due to CG group characteristics similar to those found in Logue et al. (6,10).
The positive changes observed for the CG could also result from recruiting highly motivated volunteers or the financial support given to the participants (6,10). The selection processes used may have attracted individuals more likely to undergo lifestyle changes, who, therefore, were not representative of the general population (12).
Similar methodological weaknesses were also identified in a review that aimed to evaluate the effectiveness of TTM-based interventions on sustainable weight reduction. Besides pointing out the insufficient information related to randomization and blinding, the authors indicate others limitations such as wide use of self-reported measures and lack of post-intervention assessments that could allow verifying long-term weight loss sustainability (31).
It should be highlighted that the use of multi-behavioral TTM is justified considering the complexity of the behaviors associated with people's lifestyles. It is estimated that 15% of the population account for 60% of health care costs due to multiple health-risk behaviors (1). Considering the relevance of maximized cost--effectiveness interventions, multi-behavioral TTM is promising for promoting coaction or paired actions, in which the change on one behavior can have a potential to change another behavior (29,30). The interventions evaluated in this review were included because they were multi-behavioral. However, sometimes the studies did not conduct simultaneous interventions for multiple health risks because some individuals were already at the action and/or maintenance stages for a certain behavior or individuals' choice of a particular type of intervention. Nonetheless, although at advanced stages of change, these individuals could have relapses, which support the multi-behavioral approach.
The interventions used had a heterogeneous set of methods, with different combinations of intensities, follow-up periods, technologies, theoretical models, uses of the TTM, target behaviors, target populations, and variables analyzed. Such heterogeneity makes it difficult to compare or reproduce the studies, in addition to limit the applicability of the discoveries to clinical practice (31).
The use of technological tools was a predominant method of intervention application. This is likely a consequence the complex logistics of face-to-face interventions, which require a large number of professional staff, substantial amounts of time, elevated cost, and other difficulties associated with reaching a large number of participants (6-8,22). On the other hand, the use of technologies may present some difficulties, like assessing the intensity of the intervention, actual participation of the individuals (14), creation of bonds between the educators and the participants, and the sensitization and motivation achieved though virtual communication.
In addition, when evaluated by e-mail, the engagement of the participants was low. In one study, only 30% answered to the evaluation questionnaires sent six and twelve months after the study began (7). The participation in such technological interventions also imposes certain requirements, such as knowing how to read and write and having access to a computer, Internet (1,5-11,14,22), or telephone (1,10,11,22). It also requires that the participants have the basic informatics skills to use interactive platforms, dynamic simulations, and access links (6,14,25,26).
Concerning the use of the TTM, although it comprises four pillars, most of the studies explored solely the stages of change, despite the fact that the authors of the studies highlighted the importance of the other TTM mediators. The importance of evaluating all the pillars is evidenced in the work of Greaney et al. and Greene et al. (The -SENIOR study) (16,17), in which the participants that received advice on diet and were at the maintenance stage had higher self-efficacy and use of the processes of change (17), whereas those who received intervention for the promotion of physical activity (PA) had a higher score in starting or maintaining activity (16).
Given the heterogeneous methodology observed, we suggest that CG members do not receive treatment or are exposed to interventions comparable in intensity to those received by IG members in future studies; therefore, the only distinction between the groups is the intervention content. Future studies of interventions should be detailed regarding the nature and magnitude of TTM dimensions that are used and carried out with methods applicable to the population in general. Potential limitations of this review include those linked to bibliographical research, such as the possible omission of studies related to the theme (32). On the other hand, to minimize this bias, several strategies were employed; these included using a large number of keywords, determining the search strategies in advance, defining inclusion and exclusion criteria, having two independent researchers select the articles, reviewing any additional references in the selected articles, and contacting the authors of the articles when necessary.
The obtained results reveal a growing interest in the international use of interventions based on the TTM for multiple health-related behaviors, especially using technological tools (computer and telephone), which has not yet been seen in Brazil. They provide evidence of the need for national studies and publications.
References
1. Clark PG, Nigg CR, Greene G, et al. The Study of Exercise and Nutrition in Older Rhode Islanders (SENIOR): translating theory into research. Health Educ Res 2002;17(5):552-61. [ Links ]
2. Sutton K, Logue E, Jarjoura D, et al. Assessing dietary and exercise stage of change to optimize weight loss interventions. Obes Res 2003;11(5):641-52. [ Links ]
3. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot 1997;12(1):38-48. [ Links ]
4. Van Sluijs EM, Van Poppel MN, Van Mechelen W. Stage-based lifestyle interventions in primary care: are they effective? Am J Prev Med 2004;26(4):330-43. [ Links ]
5. Johnson SS, Paiva AL, Cummins CO, et al. Transtheoretical model-based multiple behavior intervention for weight management: effectiveness on a population basis. Prev Med 2008;46(3):238-46. [ Links ]
6. Cook RF, Billings DW, Hersch RK, et al. A field test of a web-based workplace health promotion program to improve dietary practices, reduce stress and increase physical activity: randomized controlled trial. J Med Internet Res 2007;9(2):e17. [ Links ]
7. Prochaska JO, Velicer WF, Rossi JS, et al. Multiple risk expert systems interventions: impact of simultaneous stage-matched expert system interventions for smoking, high-fat diet, and sun exposure in a population of parents. Health Psychol 2004;23(5):503-16. [ Links ]
8. Prochaska JO, Velicer WF, Redding C, et al. Stage-based expert systems to guide a population of primary care patients to quit smoking, eat healthier, prevent skin cancer, and receive regular mammograms. Prev Med 2005;41(2):406-16. [ Links ]
9. Prochaska JO, Butterworth S, Redding CA, et al. Initial efficacy of MI, TTM tailoring and HRI's with multiple behaviors for employee health promotion. Preventive Medicine 2008;46:226-31. [ Links ]
10. Logue E, Sutton K, Jarjoura D, et al. Transtheoretical model-chronic disease care for obesity in primary care: a randomized trial. Obes Res 2005;13(5):917-27. [ Links ]
11. Jones H, Edwards L, Vallis TM, et al. Changes in diabetes self-care behaviors make a difference in glycemic control. Diabetes Care 2003;26(3):732-7. [ Links ]
12. Svetkey LP, Harsha DW, Vollmer WM, et al. Premier: a clinical trial of comprehensive lifestyle modification for blood pressure control:rationale, design and baseline characteristics. Ann Epidemiol 2003;13(6):462-71. [ Links ]
13. Elmer PJ, Obarzanek E, Vollmer WM, et al; PREMIER Collaborative Research Group. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control: 18-month results of a randomized trial. Ann Intern Med 2006;144(7):485-95. [ Links ]
14. Block G, Sternfeld B, Block CH, et al. Development of Alive! (A Lifestyle Intervention Via Email), and its effect on health-related quality of life, presenteeism, and other behavioral outcomes: randomized controlled trial. J Med Internet Res 2008;10(4):e43. [ Links ]
15. Sternfeld B, Block C, Quesenberry CP Jr, et al. Improving diet and physical activity with ALIVE: a worksite randomized trial. Am J Prev Med 2009;36(6):475-83. [ Links ]
16. Greaney ML, Riebe D, Ewing GC, et al. Long-term effects of a stage-based intervention for changing exercise intentions and behavior in older adults. Gerontologist 2008;48(3):358-67. [ Links ]
17. Greene GW, Fey-Yensan N, Padula C, et al. Change in fruit and vegetable intake over 24 months in older adults: results of the SENIOR project intervention. Gerontologist 2008;48(3):378-87. [ Links ]
18. Riebe D, Greene GW, Ruggiero L, et al. Evaluation of a healthy-lifestyle approach to weight management. Prev Med 2003;36(1):45-54. [ Links ]
19. Riebe D, Blissmer B, Greene G, et al. Long-term maintenance of exercise and healthy eating behaviors in overweight adults. Prev. Med 2005;40(6):769-78. [ Links ]
20. Steptoe A, Doherty S, Rink E, et al. Behavioural counselling in general practice for the promotion of healthy behaviour among adults at increased risk of coronary heart disease: randomised trial. BMJ 1999;319(7215):943-7. [ Links ]
21. Steptoe A, Kerry S, Rink E, et al. The impact of behavioral counseling on stage of change in fat intake, physical activity, and cigarette smoking in adults at increased risk of coronary heart disease. Am J Public Health 2001;91(2):265-9. [ Links ]
22. Van Wier MF, Ariëns GA, Dekkers JC, et al. ALIFE@Work: a randomised controlled trial of a distance counselling lifestyle programme for weight control among an overweight working population. BMC Public Health 2006;6:140. [ Links ]
23. Van Wier MF, Ariëns GA, Dekkers JC, et al. Phone and e-mail counselling are effective for weight management in an overweight working population: a randomized controlled trial. BMC Public Health 2009;9:6. [ Links ]
24. Niederhauser VP, Maddock J, LeDoux F, et al. Building Strong and Ready Army Families: A Multirisk Reduction Health Promotion Pilot Study. Military Medicine 2005;170(3):227. [ Links ]
25. Mauriello LM, Ciavatta MMH, Paiva AL, et al. Results of a multi-media multiple behavior obesity prevention program for adolescents. Preventive Medicine 2010; 51:451-6. [ Links ]
26. Velicer WF, Redding CA, Paiva, AL, et al. Multiple behavior interventions to prevent substance abuse and increase energy balance behaviors in middle school students. TBM 2013;3:82-93. [ Links ]
27. Armitage CJ, Norman P, Noor M, et al. Evidence that a very brief psychological intervention boosts weight loss in a weight loss program. Behavior Therapy 2014;45:700-7. [ Links ]
28. Menezes MC, Mingoti SA, Cardoso CS, et al. Intervention based on Transtheoretical Model promotes anthropometric and nutritional improvements- a randomized controlled trial. Eating Behaviors 2015;17:37-44. [ Links ]
29. Yin HQ, Prochaska JO, Rossi JS, et al. Treatment-enhanced paired action contributes substantially to change across multiple health behaviors: secondary analyses of five randomized trials. Transl Behav Med 2013;3(1):62-71. [ Links ]
30. Johnson SS, Paiva AL, Mauriello L, et al. Coaction in Multiple Behavior Change Interventions: Consistency Across Multiple Studies on Weight Management and Obesity Prevention. Health Psychol 2014;33(5):475-80. [ Links ]
31. Mastellos N, Gunn LH, Felix LM, et al. Transtheoretical model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database Syst Rev 2014;2:CD008066. [ Links ]
32. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Medic 2009;6(7):1-6. [ Links ]
![]() Correspondence:
Correspondence:
Mariana Carvalho de Menezes.
Escola de Enfermagem.
190 Alfredo Balena ave.
Santa Efigênia, Belo Horizonte.
30190-100. Brazil
e-mail: marysnut@gmail.com
Received: 17/12/2015
Accepted: 01/04/2016
