










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Atherosclerosis is crucial to cardiovascular disease (CVD) and is strongly related to dyslipidemia 1. Classically, dyslipidemia includes high total cholesterol, high low-density lipoprotein (LDL) cholesterol, low high-density lipoprotein (HDL) cholesterol, and high triglycerides. In effect, cholesterol plaques are distinctive features of the atherosclerotic lesions 2. Dyslipidemia is also a target of CVD risk scoring for stratification and prevention 1. The epidemic of CVD is now a global phenomenon, and remains the highest cause of death worldwide 3. Given the several health risks and public health burdens of CVD 1,3, its prevention or management is becoming a major challenge. Therefore, identifying dietary factors that may favorably affect serum lipids is of great importance.
Current management of CVD involves various lifestyle changes, dietary and exercise regimes 4 and the use of drugs or medical interventions 2. Nowadays, there is growing interest in the use of plant foods for the prevention and management of CVD and other related disorders, with a special emphasis on cocoa and its products 5.
Cocoa (Theobroma cacao L.) is one of the most ancient cultivated human crops. It is originated in Mexico and is central to the local diet 6. Nowadays, cocoa is grown mainly in Indonesia, Sri Lanka and West Africa 6. Cocoa is traditionally consumed as a beverage with or without milk. However, it is now used on a much larger scale as a basic ingredient for numerous chocolate products and confectionaries 7. Consumption of cocoa is related to higher-quality diets, including higher intakes of protein, antioxidants and a number of vitamins and mineral elements 8. Cocoa intake is also associated with several beneficial health effects, particularly reduced risks of obesity, diabetes, hypertension and CVD 8) (9.
Numerous cardioprotective effects of cocoa products have been reported, such as improved heart function, decreased oxidative susceptibility of LDL-cholesterol and reduced platelet activation, as shown by several comprehensive reviews 5) (8) (9. However, evidence for possible antihyperlipidemic activity of cocoa has been limited and mixed. Several studies have shown that cocoa products do not or variably affect lipid profile 10) (11) (12) (13) (14) (15, whereas other studies failed to support this 13) (14) (15) (16) (17) (18) (19. In this regard, there are no animal studies. Here, it is important to strictly define cocoa and its products. Cacao is the natural product, and cocoa or cocoa powder is the processed product, whereas chocolate is the food prepared from a combination of cocoa, sugar, fat, milk and other ingredients 8. Thus, chocolate and cocoa are two different terms and are not interchangeable, and many of the proposed health effects of cocoa may not be applicable to chocolate 20. In essence, cocoa itself is a reasonable product to study or to recommend from the point of view of health, as chocolate contains several non-cocoa constituents.
The basic concern regarding cocoa products and CVD has been related to their high caloric load mostly due to the high fat content, the bulk of which is composed on average of 33% saturated stearic acid, 25% palmitic acid, and 33% monounsaturated oleic acid 8) (20. The high fat content of cocoa may be viewed as a potential confounder affecting lipid assimilation and metabolism, the effect of which is not exactly known yet and may be unfavorable 20. In general, most of the nutritional and clinical studies linking cocoa with CVD have been mainly devoted to the effects of bioactive components such as polyphenols and flavonoids, and have often paid little or no attention to the cocoa fat as a possible mechanism for explaining such link. In fact, fats are the highest variable components of the diet both in quantitative and in qualitative terms, and they are the most relevant dietary factor affecting serum lipids, especially in cases with dyslipidemia 15. Nevertheless, controlled human or animal studies that link consumption of defatted cocoa and cholesterol with serum lipids and lipoproteins in particular are generally lacking. Therefore, we investigated whether the consumption of diets containing varying amounts of defatted cocoa with and without cholesterol had any effect on serum concentrations of total cholesterol, LDL-cholesterol, HDL-cholesterol and triglycerides in rats fed on such a dietary regimen for a period of ten weeks.
MATERIALS AND METHODS
DEFATTED COCOA POWDER PREPARATION
One batch (10 kg) of medium fat alkalized cocoa powder (Cadbury(r), Birmingham, England) was purchased from the local market in Amman, Jordan. The powder was defatted following the reference solvent extraction method 21. In this method, the powder was soaked with petroleum ether (boiling point 40-60 oC) in dark glass bottles (1:3, weight/volume), and was left at room temperature for 48 hours with occasional shaking. The mixture was allowed to stand and decanted to remove the solvent with its dissolved fat, and a fresh solvent was then added. This process was repeated three successive times. During the third time, a little amount of water was added to the mixture to facilitate separation and mixed slowly, and the fat-free cocoa powder was separated through a malti cloth. The defatted powder was air-dried and was blended in a stainless steel blender (Kenwood(r), Hampshire, England) for 20 minutes to obtain homogenous powder. The resultant powder was placed in sealed dark polythene bags and kept refrigerated at 4 °C until further use. The macronutrient content of the whole and defatted cocoa powder as determined by the Weende method 21 is presented in table I.

EXPERIMENTAL DIETS
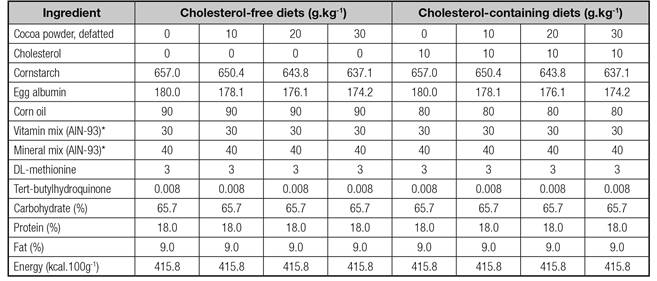
Eight isocaloric and isonitrogenous diets were prepared; four of them were cholesterol-free and differed in their content of defatted cocoa powder (0%, 1%, 2%, or 3%, w/w) while in the other four 1% cholesterol was added, at the expense of fat, to induce hyperlipidemia. The protein and carbohydrate contents of defatted cocoa powder were taken into consideration in the calculation of nutrient composition of the diets. Ingredient composition of the diets is described in table II. All diets contained the same amount of calories, protein, carbohydrate, fat, vitamins and mineral elements.
Dietary supplies of nutrients were in accordance with the dietary recommended allowances for rats from the American Institute of Nutrition 22. Macronutrient and energy contents of the diets are described in table II. Diets were freshly prepared once a week and placed desiccated in sealed dark polythene bags, and then kept refrigerated at 4 °C.
SAMPLE SIZE CALCULATION
The resource equation method was used to calculate the sample size 23. This method is particularly suited to factorial experiments, as in the present study, involving more than two groups and measuring many outcomes, and when no previous estimate of the standard deviation is available. In a completely randomized design, sample size is the total number of animals minus the number of treatment groups 23. In this study, two diets (cholesterol-free and cholesterol-containing), four levels of defatted cocoa powder (0%, 1%, 2%, or 3%, w/w), and six rats in each treatment group (as is common) were used. Thus, treatment groups were eight, and the calculated sample size was 42. For more precision, a sample size of 48 was adopted.
ANIMAL EXPERIMENTATION
Forty-eight male Sprague-Dawley rats were obtained from the Experimental Animal Unit of the Department of Nutrition and Food Technology of the University of Jordan, Amman, Jordan. The animals were acclimatized for eleven days before the experiment, during which they were fed on chow diet with free access to tap water. They were individually housed in plastic cages with stainless steel wire-mesh bottom (North Kent Plastic Cages Ltd., Dartford, England) under controlled temperature (22 ± 2 °C) and hygienic conditions with 12-hour light, 12-hour dark cycle. All the experiments involving animals were approved by the Institutional Animal Ethics Committee and carried out according to the recommended guidelines for animal care and use 24.
At the beginning of the experiment, animals weighed 239.6 ± 1.7 g and they were randomly assigned into the four cholesterol-free or four cholesterol-supplemented diets described above. During the experimental period, which lasted for ten weeks, experimental diets and tap water were given ad libitum. Body weight and food intake were monitored weekly. Food efficiency ratio as body weight gain (g) per 100 (g) food intakes was also calculated. On the termination day and after an overnight fast, animals were anesthetized using chloroform. Blood was collected by performing cardiac puncture and the serum was isolated and stored frozen at -20 °C until chemical analysis.
BIOCHEMICAL ANALYSIS
Concentrations of serum lipids and lipoproteins were determined by using commercial kits and in accordance to the manufacturer's instructions (Labkit, Spain and Syrbio, France). The lipid variables included total cholesterol, LDL-cholesterol, HDL-cholesterol, very low density lipoprotein (VLDL) cholesterol, and triglycerides. Analysis was performed at the Heteen Medical Laboratories, Zarqa, Jordan, using a pre-calibrated automated clinical chemistry analyzer (Humalyzer 2000, Human Gesellschaft für Biochemica und Diagnostica mbH, Wiesbaden, Germany). Atherogenic index ({total cholesterol minus HDL-cholesterol}/HDL-cholesterol), and ratios of total cholesterol/triglycerides and HDL-cholesterol/LDL-cholesterol were then computed 25,26.
STATISTICAL ANALYSIS
Data analysis was performed using statistical analysis software (SAS version 9, USA). Statistical significance was assessed by two-way ANOVA followed by the Duncan's multiple range tests, and the significance was set at p < 0.05. Data were expressed as means ± standard errors of the mean (SEM). Orthogonal polynomial comparisons were used to identify statistically significant trends. This test determines the nature of the response of the studied variables to increasing levels (0%, 1%, 2%, 3%) of defatted cocoa powder. Linear, quadratic and cubic trends were given as coefficient of determination (r2) at p < 0.05.
RESULTS
The macronutrient composition of whole and defatted cocoa powders used in this study is given in table I. Whole cocoa powder was found to contain high content of fat (20.4 g/100 g) and energy (458 kcal/100 g). On dry matter basis, defatting process reduced fat and energy contents of the cocoa by almost 95% and 23% respectively. This process also resulted in marked increase in carbohydrate, protein, ash and fiber contents of the cocoa.
Table III presents body weight, food intake and food efficiency ratio of rats fed defatted cocoa powder with and without cholesterol. Initial body weights were essentially similar (p ≥ 0.05) in all rats of the control and experimental groups. Compared to cholesterol-free control, cholesterol feeding did not significantly (p ≥ 0.05) influence body weight, weight gain, and food efficiency ratio, but it induced a significant (p < 0.05) increase in food intake. In neither control nor experimental groups did defatted cocoa feeding affect these variables.
Table III Body weight, food intake and food efficiency ratio of rats fed defatted cocoa powder for ten weeks

$Values are means ± SEM. *Values in rows with different superscripts are significantly different (p < 0.05). #Body weight gain (g)/100 g food intake.
Concentrations and indexes of serum lipids and lipoproteins of rats fed defatted cocoa powder with and without cholesterol are shown in table IV. In contrast to control, cholesterol feeding resulted in significant (p < 0.05) increase in serum HDL-cholesterol and total cholesterol/triglycerides ratio, and decrease in triglycerides, whereas LDL- cholesterol, HDL- cholesterol/LDL-cholesterol ratio and atherogenic index were unaffected. Noteworthy, serum total cholesterol and VLDL-cholesterol were modestly but insignificantly (p < 0.08) increased by cholesterol feeding.
In cholesterol-free groups, compared to control, 3% defatted cocoa feeding produced significant (p < 0.05) decrease in LDL-cholesterol and triglycerides, and increase in total cholesterol/triglycerides ratio (Table IV). Compared to 1% and 2% defatted cocoa, 3% defatted cocoa feeding induced also significant (p < 0.05) decrease in triglycerides and increase in total cholesterol/triglycerides ratio. In cholesterol-containing groups, compared to control, 3% defatted cocoa feeding caused significant (p < 0.05) increase in atherogenic index and VLDL-cholesterol, and decrease in HDL-cholesterol. Noticeably, the decrease in triglycerides and the increase in total cholesterol/triglycerides ratio induced by cholesterol were essentially maintained throughout the various levels of defatted cocoa feeding.
In cholesterol-containing groups, compared to defatted cocoa feeding in cholesterol-free groups, 3% defatted cocoa feeding induced significant (p < 0.05) decrease in triglycerides and increase in VLDL-cholesterol, atherogenic index and total cholesterol/triglycerides ratio (Table IV). Furthermore, 1% and 2% defatted cocoa feeding in cholesterol-containing groups resulted in significant (p < 0.05) increase in total cholesterol/triglycerides ratio and decrease in triglycerides compared to those in cholesterol-free groups. In all groups, none of the other lipid variables were notably affected by defatted cocoa feeding.
Table IV Serum lipid and lipoprotein concentrations and indexes of rats fed defatted cocoa powder for ten weeks
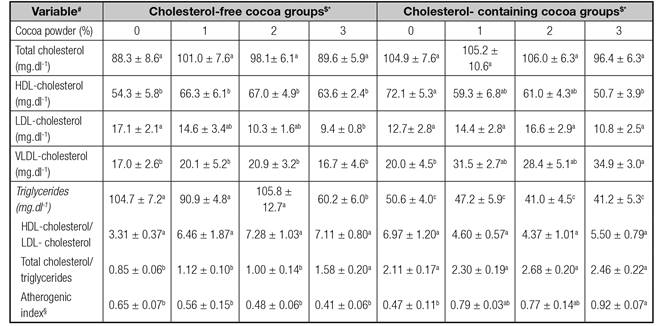
$Values are means ± SEM. *Values in rows with different superscripts are significantly different (p < 0.05). #HDL: High-density-lipoprotein; LDL: Low-density-lipoprotein; VLDL: Very low-density-lipoprotein. §{(Total cholesterol-HDL-cholesterol)/HDL-cholesterol}.
Orthogonal polynomial trend analysis of studied variables of rats fed cholesterol-free and cholesterol-supplemented diets with increasing defatted cocoa powder for ten weeks is given in table V. In both control and experimental groups, none of the lipid and other biological variables did show quadratic or cubic trends in response to defatted cocoa feeding. In cholesterol-free groups, LDL-cholesterol, triglycerides and atherogenic index exhibited marked (p < 0.05) descending linear trends, whereas both ratios of HDL-cholesterol/LDL-cholesterol and total cholesterol/triglycerides exhibited (p < 0.05) ascending linear trends. In cholesterol-containing groups, descending linear trend (p < 0.001) was obtained for HDL-cholesterol, and ascending linear trends (p < 0.05) were seen for VLDL-cholesterol and atherogenic index. No linear trends were observed for the other studied variables.
Table V Orthogonal polynomial trend analysis of studied variables of rats fed defatted cocoa powder for ten weeks
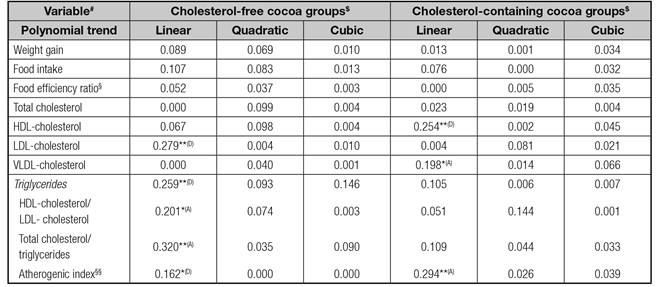
$Values are coefficients of determination (r2); *p < 0.05; **p < 0.01; (A) ascending; (D) descending. #HDL: High-density-lipoprotein; LDL: Low-density-lipoprotein; VLDL: Very low-density-lipoprotein. §Body weight gain (g)/100 g food intake. §§{(Total cholesterol-HDL-cholesterol)/HDL-cholesterol}.
DISCUSSION
The present study shows that in rats, the addition of varying amounts of defatted cocoa powder to cholesterol-free and cholesterol-containing diets did not affect body weight and food intake. There was a contradictory effect for defatted cocoa on serum lipid profile; this effect was seemingly favorable in rats fed cholesterol-free diet and unfavorable in those given cholesterol-containing diet. In effect, defatted cocoa was unable to counteract the untoward effects of cholesterol on serum lipids. The 3% defatted cocoa had the most prominent effect on serum lipids in all experimental groups. Furthermore, the recorded results were reinforced by remarkable corresponding orthogonal linear trends.
The energy and macronutrient composition of the whole cocoa powder used in this study was comparable to the literature range values 27. However, relative variability in the nutritional properties of cocoa powder has been reported. This variability may be attributed to a number of factors, such as differences in genotype, maturity stage, postharvest handling and storage conditions, product quality and analytical procedures 27. The presently obtained fat and energy values for defatted cocoa were consistent with those reported elsewhere 28.
Dietary cholesterol has been widely used in animals to modify lipid metabolism 25) (26. Consistently, in this study, cholesterol feeding increased serum HDL-cholesterol and total cholesterol/triglycerides ratio, and decreased triglycerides. Cholesterol had some increasing effect on total cholesterol and VLDL-cholesterol, but this effect did not reach statistical significance. In line with these results, serum total cholesterol has been shown to increase or remain unchanged as a result of cholesterol feeding in animals 25. Furthermore, there is a general agreement regarding the triglyceride-reducing effect of cholesterol and the lack of its influence on body weight and food efficiency ratio 25,26, a matter that accords with the findings of the current study.
It is noteworthy that the currently recorded body weight and food intake were kept unchanged in all experimental groups. Several human studies have investigated the effect of cocoa or its products on body weight, but no animal studies are available. In agreement with our results, ingesting 100 g/day dark chocolate (70% cocoa) for seven days has not been shown to affect body weight in obese women 29. Similar results have been obtained in 49 healthy women following daily consumption of 41 g chocolate, 60 g almonds, or almonds and chocolate together for six weeks 30. Furthermore, no changes in body weight have been documented in men and women ingesting 50 g/day dark chocolate for three weeks 31.
There is a surprisingly large human literature on the relationship between cocoa and CVD, which has expanded rapidly since the 1990s. Despite this, there appears to remain a relative scarcity of the literature dealing with cocoa and CVD lipid markers 13) (14) (15) (16) (17) (18) (19) (20, and findings also remain controversial. This might be due to the large discrepancy between the various experimental protocols used. In fact, the type and complexity of the cocoa source, genotype, manufacturing processes or chemical structure, the amount consumed, feeding duration, energy intake, basal diet composition and other lifestyle patterns are among many potential confounders that may contribute to this inconsistency. It may be also noticed that the aim of most of the previous studies was to evaluate the effect of whole cocoa or chocolate polyphenols, particularly flavonoids, in normal or pathological conditions. However, studies involving defatted cocoa inclusion to cholesterol-containing diets or those investigating such diets on serum lipids in humans and animals are generally scarce. This certainly limits the comparison of the present results with those of the other studies.
To the best of our knowledge, this study is perhaps the first demonstration that specifically links defatted cocoa with serum lipid parameters in the cholesterol-fed rats. It is generally accepted that this model has disturbed lipid metabolism 25) (26. Under the present experimental conditions, the 3% defatted cocoa had the main impact on serum lipids. A significant fall in serum LDL-cholesterol and triglycerides, and a rise in total cholesterol/triglycerides ratio occurred in response to 3% defatted cocoa in rats fed cholesterol-free diet as compared to control. The decrease in triglycerides was obviously the reason behind the increase in total cholesterol/triglycerides ratio. On the other hand, in contrast to control, the 3% defatted cocoa induced an evident increase in serum VLDL-cholesterol and atherogenic index, and a decrease in HDL-cholesterol in rats fed cholesterol-containing diet. Moreover, the 3% defatted cocoa caused significant rise in VLDL-cholesterol, atherogenic index and total cholesterol/triglycerides ratio, and fall in triglycerides in rats fed cholesterol-containing diet compared to those fed cholesterol-free diet. Interestingly, the triglyceride-reducing action of cholesterol was maintained in rats fed cholesterol-containing diet without a noticeable effect of the different defatted cocoa levels. In essence, these results clearly demonstrate a favorable effect of defatted cocoa on serum lipid fractions in rats fed cholesterol-free diet, and an unfavorable effect in those fed cholesterol-containing diet. The reasons responsible for these findings and their physiologic and clinical significance are not clear. However, the following discussion will focus on the available literature.
In humans, consumption of 16-50 g dark or milk chocolate daily by healthy free-living normocholesterolemic individuals for periods of 2-4 weeks has been shown to increase HDL-cholesterol 10) (31) (32) (33) (34, decrease LDL-cholesterol 13) (14) (15) (16) (17) (31 and triglycerides 31) (34, or to produce no effects on total cholesterol, LDL-cholesterol, VLDL-cholesterol and HDL-cholesterol/LDL-cholesterol ratio 10) (33. Cocoa products have also been reported to increase HDL-cholesterol in hypercholesterolemic individuals 32. In obese women, ingesting 100 g/day dark chocolate containing 70% cocoa for seven days has been shown to increase HDL-cholesterol and decrease ratios of total cholesterol/HDL-cholesterol and LDL-cholesterol/HDL-cholesterol 29. Furthermore, several comprehensive reviews examining the effects of consumption of cocoa or its products on serum lipids have shown that short-term ingestion of these products led either to decrease in LDL-cholesterol and total cholesterol with no major effects on HDL-cholesterol and triglycerides 13,14, or just to marginal effects on LDL-cholesterol and HDL-cholesterol 9. Apparently, some of these results are consistent with our findings; however, a remarkable variation in the experimental approaches still exists. It seems that the currently recorded favorable effect of defatted cocoa on serum lipid fractions in rats fed cholesterol-free diet somewhat accord with that reported in normocholesterolemic individuals 10) (17) (31) (34. On the other hand, the effect of feeding cocoa and cholesterol together on serum lipids has not been yet investigated in humans or animals.
It may be noted that whole cocoa-containing chocolate was the study substance for the aforementioned human studies. In this respect, it has been stated that the great differences in the chocolate consumption in different population groups, and varied chocolate composition in terms of cocoa concentrations (15-85%), added food ingredients particularly milk, fat or sugar, or bioactive components such as polyphenols, carotenoids and phytosterols, make it rather difficult to evaluate the impact of chocolate on blood lipids in observational studies 8) (15. Unlike these studies, we used solely defatted cocoa powder and incorporated it into a standardized rat diet. In view of these facts, in contrast to chocolate, cocoa itself has been recommended as a cardioprotective strategy 20.
The recorded results of the orthogonal polynomial linear trend analyses provided further substantiation for the discriminative effect of defatted cocoa on serum lipids in rats fed either cholesterol-free or cholesterol-containing diet. Marked descending linear trends for LDL-cholesterol, triglycerides and atherogenic index, and ascending linear trends for ratios of HDL-cholesterol/LDL-cholesterol and total cholesterol/triglycerides were demonstrated in the former rat group; whereas in the latter group, substantial descending linear trend for HDL-cholesterol, and ascending linear trends for VLDL-cholesterol and atherogenic index were obtained. Noteworthy, such data approaches have not been yet documented elsewhere.
However, some limitations to the present study need to be noted. The possible bioactive component in defatted cocoa neither was determined nor was its serum level assessed. Thus, the mechanisms by which defatted cocoa and cholesterol interact and affect serum lipids cannot be clearly explained. Nevertheless, we were able to report a favorable effect of defatted cocoa on serum lipid profile in rats fed cholesterol-free diet and unfavorable effect in those given cholesterol-containing diet.
CONCLUSIONS
Taken together, when incorporated into isocaloric and isonitrogenous diets in varying amounts, the particular 3% defatted cocoa appears to exert a profound favorable effect on serum lipids in cholesterol-deprived rats and, evidently, an unfavorable effect in cholesterol-fed rats. Defatted cocoa is seemingly ineffective to counteract the atherogenic effect of cholesterol in rats. It is also obvious that a sort of interaction between cholesterol and defatted cocoa took place, though it was not addressed. Thus, it would be of great importance to explore the mechanisms by which defatted cocoa and cholesterol interact and modify lipid assimilation and metabolism under cholesterol diet conditions. This could be useful to lessen the debate surrounding the claim that consumption of cocoa or its products can reduce the risk of dyslipidemia, atherosclerosis and CVD in man.

