










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
There is a great variety of techniques to evaluate the nutritional status of a patient, although there is no single parameter available. Malnutrition implies a decrease in muscle mass, which is reflected in poorer performance on functional tests and alterations in body composition 1) (2) (3. This decrease in muscle strength appears before changes in anthropometric measurements and laboratory parameters are observed. Accordingly, the measurement of muscle strength may be a useful tool in screening and assessing malnutrition 4. The American Society for Parenteral and Enteral Nutrition has included the assessment of grip strength by dynamometer as one of the six criteria to define malnutrition 5, encouraging the use of cut-off points in each population by age and gender 6.
There are numerous clinical studies in hospitalized individuals or outpatients (surgical, elderly, oncological, etc.) that demonstrate that decreased grip strength, measured by hand dynamometry, is associated with increased stays, mortality and complications 3) (7) (8. Similarly, in epidemiological studies performed in different age groups, decreased grip strength is also associated with higher mortality and impaired functionality 3. Some body composition measures, like lean mass, seem to have a close relationship with hand strength as well as with physical function 9.
The hand dynamometer evaluates the isometric force of the hand and the forearm providing a quick, easy to use, and inexpensive method to assess the grip strength and, thus, the nutritional status of patients 10. Currently, the Jamar dynamometer is the most commonly used in clinical practice 4) (11) (12) (13. Over the last few years, dynamometry reference values have been published in different countries, usually for the Jamar-type dynamometer 4) (11) (14) (15, including a meta-analysis 16.
In Spain, the normative data are from another type of dynamometer 17) (18) (19 with no studies using the Jamar dynamometer. Likewise, there are no data comparing the results of the two different types of dynamometers, so it remains unknown if the measurements of both dynamometers are comparable in clinical practice. There are only a few studies relating dynamometry results to body composition 15) (20. The objective of this study was to contribute reference values in a sample of subjects belonging to the general population in Spain using the Jamar dynamometer, to compare them with the Collin dynamometer, and to assess the relationship between dynamometry and anthropometric parameters, especially lean mass.
MATERIAL AND METHODS
Our sample comprised a total of 817 healthy adults recruited from the population-based Pizarra study (Malaga) 21. These individuals, aged between 18 and 65 years, were randomly selected from the municipal census. Individuals who were institutionalized, pregnant, or who had severe physical or psychiatric conditions were excluded as were morbidly obese subjects (body mass index [BMI] > 40 kg/m2). All subjects gave their written consent, and the study was approved by the Ethics and Clinical Research Committee of the Regional University Hospital of Malaga.
Anthropometric measurements included weight, obtained with a scale adjusted to 0.1 kg (SECA 665, Seca, Germany), and height, using a stadiometer adjusted to 0.01 m (Holtain Ltd., Croswell, UK), to calculate BMI. Skinfold thicknesses (subscapular, triceps, biceps, abdominal) were measured at standard sites 22 by a single investigator using a plicometer (Holtain Ltd., Croswell, UK) with the precision of 0.2 mm. Three measurements were taken and the mean was calculated. Arm circumference was measured using a flexible measuring tape to the nearest 0.1 cm at the midpoint of the arm. Lean mass and fat mass percentages were estimated using the Durnin 23 and Siri 24 equations. Hand dynamometry was performed using a Collin dynamometer (Medizintechnik AS, Germany) and a Jamar dynamometer (Asimow Engineering Co., Los Angeles, CA).
In the case of the Jamar dynamometer, the subjects were instructed to adjust the device so that the grip would be comfortable for their hand to obtain the best performance 25, although most chose to use the second position (3.8 cm). The subjects were instructed to squeeze the dynamometer with the maximum force they could apply after receiving a verbal command 26.
The measurements were taken with the patients sitting in a straight back chair with both feet on the ground, shoulders close to the body in a neutral position, and the elbow flexed at 90° without rotation 27.
Three measurements were obtained in the dominant hand with a rest period of at least one minute between trial 28. There was a minimum ten minute break between Collin and Jamar measurements, in that order.
The mean was calculated and the highest value was used to represent hand grip strength.
STATISTICAL ANALYSIS
Data analysis was performed using SPSS Statistics software v22. Descriptive data are shown as means and standard deviations. The Kolmogorov-Smirnov test was used to establish whether the variables followed a normal distribution.
In the hypothesis testing for continuous variables between groups, the Student's t test was used in the variables that followed a normal distribution and a non-parametric test (Mann-Whitney) was used for variables that were not normally distributed. We rejected the null hypothesis with an alpha of 0.05 for two tails. The degree of association between hand dynamometry, BMI and body composition measurements was analyzed using the Pearson's correlation coefficient.
RESULTS
A total of 817 adults, 364 men and 453 women, were studied (Table I).
The measurements were valid for the Jamar dynamometer in all subjects studied, but only in 748 cases for the Collin dynamometer (364 men and 384 women), due to the difficulty for grasping the dynamometer. A total of 69 women could not apply the necessary force. Their mean age was 54.6 (± 9.2) years, significantly higher (p < 0.001) than in the group of women who were able to perform the test (47.8 ± 9.2 years). Table II and Table III show the grip strength values for the two dynamometers used, grouped by gender and distributed by age, together with their corresponding percentiles.
Table I General and anthropometric characteristics of the study population

n: number. BMI: body mass index.
Table II Strength of the dominant hand by gender and age, measured with a Collin dynamometer
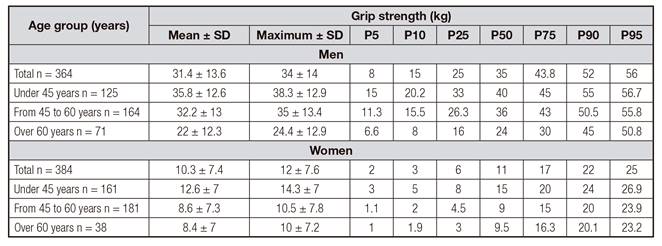
SD: standard deviation.
Table III Strength of the dominant hand by gender and age, measured with a Jamar dynamometer

SD: standard deviation.
A high correlation was found between the data obtained with the Jamar and Collin dynamometers (r = 0.782; p < 0.001) (Fig. 1). Mean strength was higher in men than in women with both instruments and in all age groups (p < 0.001). There was a tendency towards a negative correlation between age and grip strength with the Jamar dynamometer (r = -0.67; p = 0.58), which was significant with the Collin dynamometer (r = -0.143; p < 0.001). This significant correlation was observed with the Collin dynamometer in the subjects between the ages of 45 and 60 (r = -0.1; p = 0.04), and those above 60 years (r = -0.22; p = 0.02), which was not the case in those under age 45 (r = 0.02; p = 0.74). With the Jamar type dynamometer, this correlation was significant in the group of subjects under age 45 (r = 0.12; p = 0.04), in those between the ages of 45 and 60 (r = -0.12; p = 0.023) and in subjects over 60 years of age (r = -0.2; p = 0.02).
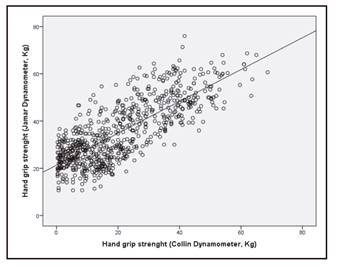
Figure 1 Relationship between hand grip strength measured by Collin dynamometer and Jamar dynamometer.
A positive correlation was found between grip strength using the Jamar dynamometer and BMI (r = 0.086; p = 0.014). This relationship increased when subjects were classified as normal weight (r = 0.268; p < 0.001) or overweight (r = 0.146; p = 0.006). No association was found between BMI and grip strength in obese patients.
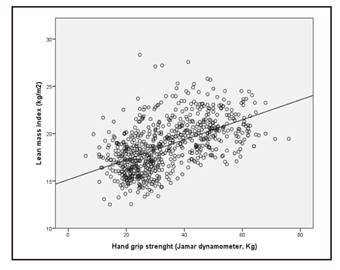
The values obtained using the Jamar dynamometer showed a positive correlation with weight (r = 0.514; p < 0.001), height (r = 0.714; p < 0.001), and arm circumference (r = 0.249; p < 0.001), and a negative correlation with fat mass in kg: (r = -0.597; p < 0.001), triceps skinfold (r = -0.497; p < 0.001), biceps skinfold (r = -0.404; p < 0.001) and subscapular skinfold (r = -0.209; p < 0.001). There was also a significantly positive correlation between muscle strength and lean mass in kg (r = 0.774; p < 0.001) and lean mass index (LMI) (r = 0.538; p < 0.001) (Fig. 2 and Fig. 3).

Mean values obtained using the Collin dynamometer showed a positive correlation with weight (r = 0.434; p < 0.001), height (r = 0.663; p < 0.001) and arm circumference (r = 0.206; p < 0.001), and a negative correlation with fat mass (kg): (r = -0.569; p < 0.001), triceps skinfold (r = -0.518; p < 0.001), biceps skinfold (r = -0.404; p < 0.001) and subscapular skinfold (r = -0.214; p < 0.001). There was also a significantly positive correlation between grip strength and lean mass (kg) (r = 0.683; p < 0.001) and LMI (r = 0.462; p < 0.001).
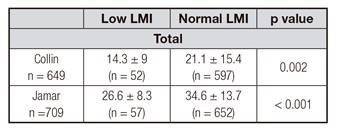
Stratifying our population by European Society of Clinical Nutrition and Metabolism criteria (LMI of 17 kg/m2 for men and 15 kg/m2 for women [29]), patients considered as malnourished due to low lean mass had significantly lower mean grip strength than normally nourished patients, both with the Jamar dynamometer and with the Collin dynamometer (Table IV).
DISCUSSION
In this study, we present normative reference values for the Spanish population using a Jamar hand dynamometer, a dynamometer for which there were no previous references in Spain, providing cut-off points to define malnutrition. Our results are similar to those of other studies that have published reference values for the Jamar-type dynamometer in Caucasian populations 14) (20) (30.
In the total sample, the cut-off points to define malnutrition (5th percentile) were 29 kg in men and 14 kg in women for the Jamar dynamometer, although this varied depending on age (Table III). These values are similar to those of other studies 15) (20 and may be related to poorer functionality, as some authors suggest 31) (32.
Similar to other studies 4) (20) (27, our values were significantly higher in men than in women for all age groups and negative correlations with age were observed, finding a decrease in grip strength (4). This has been attributed to age-related sarcopenia, since the weight loss that occurs with aging is primarily due to the loss of lean mass, thus leading to loss of grip strength 17. In our sample, no significant differences between the groups of individuals under 45 years and between 45 and 60 years were found, possibly because age-related sarcopenia appears especially in subjects aged 60 and older 4.
As in other studies, a positive association was found between grip strength and anthropometric measures such as weight, BMI, arm circumference, and height 11) (33, although the association is weak 14.
A close correlation between dynamometry values and lean mass was also observed. Patients who met criteria for malnutrition according to LMI 29 presented lower hand grip strength. Since malnutrition due to low lean mass is primarily associated with increased morbidity and mortality related to malnutrition 29, dynamometry becomes a measure that provides a clear added value to nutritional assessment.
In subjects with acute or chronic disease, numerous factors may influence decreased muscle strength, including immobilization, decreased intake, inflammation, oxidative stress, electrolyte disturbances, use of drugs (corticosteroids, muscle relaxants, etc.). In this respect, grip strength is an excellent marker of functionality as, unlike weight, it can discriminate between malnourished individuals and those who are simply underweight and share the same BMI 10.
Furthermore, nutritional intervention studies have demonstrated significant improvement in muscle strength in the short and medium term, which also supports hand grip usefulness in patient follow-up 3) (34.
We found good correlations between grip strength measured with both dynamometers. Although the Collin dynamometer is significantly more economical, we believe its use may be less suitable than that of the Jamar dynamometer because some people (especially older women) have some difficulty in correctly grasping the device and applying force, so the measurement may not be valid. This may be of special relevance in the hospital setting, where the mean inpatients age is high.
STRENGTHS AND WEAKNESSES
Our work was carried out in the context of a population-based epidemiological study with an adequate sample size. Moreover, we measured anthropometric parameters enabling us to relate muscle strength to body composition, especially to lean mass.
Nonetheless, this was a cross-sectional study in which other parameters of functionality were not evaluated, nor was the long-term effect on morbidity and mortality verified. Measurements were only taken in the dominant hand, although some studies suggest that dominance does not affect grip strength 15) (33) (35. Finally, there was a large percentage of subjects with obesity, which could have partially conditioned the results.
CONCLUSIONS
We present reference values for hand dynamometry using a Jamar hand dynamometer for a Spanish population, providing cut-off points to define malnutrition. We recommend using the Jamar dynamometer as opposed to the Collin dynamometer in clinical practice. Hand dynamometry is associated with lean mass, which supports its usefulness in nutritional assessment.

