










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Physiological changes in pregnant women lead to an increase in energy requirements (ER) in order to cover the cost of tissue synthesis, lipid and protein deposits, and increase in basal metabolic rate (BMR), which is the major component of energy expenditure during pregnancy 1. This makes ER during pregnancy an important piece of information to be considered for appropriate dietary advice that contemplates the regulation and control of body mass during pregnancy. Positive energy balance (EB) (energy intake [EI] > energy requirement [ER]) during this period allows for the accumulation of energy reserves to meet the demands of childbirth and the beginning of lactation 1. In excess, it may predispose the pregnant woman to obesity and the fetus to macrosomia 2. If insufficient, it can lead to low gestational body mass gain and restriction of fetal growth 3. In this sense, pre-conception and gestation are considered as critical periods for coping, at a contextual level, with the obesity epidemic in childhood and adolescence 4. In Brazil, the estimated prevalence of overweight and obesity in adolescents is 20.5% and 4.9%, respectively 5. In a probability sample of adolescents attending public schools in the city of Niterói in 2013, 17.9% of the girls were overweight and 8.5% were obese 6.
Micronutrient requirements also increase during pregnancy to meet the need of accelerated fetal growth and intense cell differentiation and may require adaptations in dietary intake, especially in scenarios of habitual marginal intake to promote maternal and fetal health and the prevention of unfavorable outcomes 7. Thus, the assessment of dietary intake and anthropometric nutritional status in pregnancy should be included in the list of actions of prenatal care to subsidize health education practices, directed to nutritional disorders, for a healthy pregnancy 8.
Adolescence, the period between 10 and 19 years of age according to the World Health Organization (WHO) 9, is a social construction and takes on different forms according to its historical conditioners. The behavior of adolescents is influenced by the social, economic and cultural characteristics of their reference context 10. In Brazil, adolescents living in social contexts of social and economic inequality and precarious material conditions of life are more likely to be pregnant 11. Despite the decline of 23% in the fertility rate of the Brazilian women from 15 to 19 years observed between 2004 and 2014 12, pregnancy during adolescence is still a major challenge for the society as a whole and the health system in particular 13. Dietary inadequacies and malnutrition have been reported as frequent phenomena in pregnant adolescents derived from the social context in which they live 7,14, representing a public health issue both in developed and developing countries. There are scarce data on the characteristics of dietary intake of pregnant adolescents in Brazil. Among those from low socioeconomic classes, it is assumed that the dietary intake is not balanced and does not cover the nutritional requirements and, therefore, need be evaluated. Considering the current scenario of growing prevalence of obesity in all segments of the Brazilian population 5, the present study aimed to assess the anthropometric and dietary intake (energy, macro and micronutrients) of pregnant adolescents recruited from primary health care units of a municipality located in the tropical region of Brazil.
MATERIALS AND METHODS
Between February 2008 and March 2014, all pregnant adolescents who sought prenatal medical care in basic health care units in the municipality of Niterói, RJ, Brazil, regardless of their gestational week, were contacted by researchers who provided oral and written information about the research project. At this time, identification data and obstetric history of the adolescents interested in participating in the study were collected from the Prenatal Card and a visit to the Nutritional and Functional Assessment Laboratory at the University was scheduled for anthropometric, dietary intake and BMR measurements.
Sixty eight pregnant adolescents agreed to participate in the study and came to the laboratory early in the morning accompanied by their adult legally responsible companion. All research procedures were explained one more time and the voluntary agreement to participate in the study was confirmed by all participants and their adult legally responsible companion upon signing the informed consent form. The inclusion criteria were gestation of a single and primigravida pregnancy, and maternal age below 20 years at the estimated time of delivery. The exclusion criteria included the presence of chronic diseases prior or during pregnancy.
Prior to measuring BMR, the adherence to the protocol (absence of fever, alcohol or cigarette consumption and avoidance of heavy physical activity on the day before and on the day of measurement, ten hours of fasting and eight hours of sleep) was checked. BMR was measured in a quiet room with low luminosity and noise level and controlled ambient temperature. After a 15-minute rest period in the supine position, a mask was fixed on the adolescent's face and connected to a validated 15 indirect calorimeter (VO2000 Portable Metabolic Testing System; MedGraphics, St. Paul, MN, USA), which measured oxygen consumption (VO2) and carbon dioxide production (VCO2) for 25 minutes with the pregnant adolescent lying down motionless. Minute BMR was obtained using the equation described by Weir 16 with gas exchange data of the final 20 minutes and expressed in kcal/day. ER was calculated as the product of measured BMR and the physical activity level (PAL) with the addition of the energy cost of pregnancy according to the trimester as recommended by FAO/WHO/UNU 1. Light PAL was assumed for all pregnant adolescents.
Anthropometric measures were obtained with the pregnant women wearing standard clothing and barefoot following standardization described in Lohman et al. 17. Stature was measured twice in a wooden stadiometer with precision of 0.1 cm. The measurement was carried out at the end of an expiration and the average of the two measurements provided the final value. Body mass (BM) was obtained in an electronic scale (TANITA(r) BC-418) with precision of 0.1 kg. Body mass index (BMI) was calculated as the division of BM by squared stature. Pre-pregnancy BMI was calculated with the self-reported pre-pregnancy BM but when not available, the BM measurement obtained before the 13th gestational week was used. Pre-pregnancy nutritional status assessment was available for 33 of the pregnant adolescents and it was determined by the WHO BMI for age cut-off recommendations 18 for nonpregnant adolescents. Gestational nutritional status was determined with BMI for pregnancy age cut-off points 19 as suggested by the Brazilian Ministry of Health 8. For both instances, nutritional status was classified as underweight, adequate and overweight + obesity.
After these measurements, the pregnant adolescents were scheduled to respond 24-hour dietary recalls (R24h) during telephone interviews on three non-consecutive days, including one weekend day within the following week. All of these procedures (anthropometry, BMR and dietary intake) were planned to be repeated every four weeks thereafter.
Of the 68 pregnant adolescents who agreed to participate in the study, 21 did not respond at least two R24h and five either had infectious or contagious disease, had some discomfort with the facemask or BMR was not measured or pregnancy was not confirmed. Thus, the final sample was composed of 42 pregnant adolescents with dietary, anthropometric and BMR data. Eighteen pregnant women were assessed on two or more occasions, resulting in R24h data of 208 days.
During the R24h, ingested portion sizes were estimated with the help of an album containing photographs of foods and preparations given to participants on the day of the visit to the laboratory. The reported foods were converted to energy, macro and micronutrients according to the Brazilian Food Composition Table 20. When the food item was not available in TACO, the American food composition table 21 was used.
Protein recommendation was based on the safe level of protein intake and the additional protein for the adolescent's pregnancy trimester 22. The macronutrient and sodium intake adequacies were based on the intake goals for the prevention of chronic diseases 23. The percentage of energy, macro and micronutrient (calcium, iron, zinc and vitamin A) intake adequacies was calculated for each category of nutritional status. EI was considered to be excessive when it was over 100% of the individually-determined ER.
The economic class of the adolescents was based on the possession of goods in households and on the education level of the head of the household according to the economic classification in Brazil 24. Schooling was measured in number of full years of school attendance. Information on the occupation of the head of household was available for only 36 of the pregnant adolescents.
The project and its procedures were approved by the Ethics Committee of the Universidade Federal Fluminense. All statistical analyses were carried out in the software SAS for microcomputer version 9.2. Descriptive statistics (means, standard deviations, medians, 95% confidence intervals, coefficients of variation and percentage of distribution or adequacy) were calculated. The results were expressed in relation to both pre-pregnancy and gestational nutritional status because the diagnosis of altered nutritional status may be useful clinically in nutritional care. The association of the percentage of adequacy of energy, macro and micronutrient intakes with variables related to body size (gestational BMI), gestational week (GW) and day of the week (coded as 1 for Sunday, 2 for Monday, etc.) was assessed by mixed linear models. In these linear models, the random effects were included in the intercept, subject and GW to take into consideration the inter and intra-subject variability of the repeated dietary intake measurements during pregnancy. The models were adjusted using the restricted maximum likelihood (REML) method. The significance level was defined as α < 5% for all analyses.
RESULTS
Two-thirds of the pregnant adolescents had completed between five to eight years of schooling and 57.1% were attending school. Among the adolescents who had interrupted their studies, the most often alleged motives were moving to a different house and the lack of willingness to study. All pregnant adolescents maintained some form of relationship with the baby's father but the minority (38.1%) lived with them as an extended family or as a nuclear family. Only two pregnant adolescents were smokers. Most belonged to the low economic class (C1 and C2 = 73.8%) and 62.0% received benefits from the Bolsa Família (Family Allowance Cash Transfer Federal Program). The average schooling of the head of the household was low and equal to the pregnant adolescent's (7.3 ± 3.3 years) and 73.2% of them worked, while 14.6% were unemployed.
The average GW of the adolescents was 23.3 (SD = 8.0) and most of them had adequate nutritional status prior to pregnancy (Table I).
Table I Physical, physiological and nutritional status characteristics of the 42 pregnant adolescents in Niterói, RJ
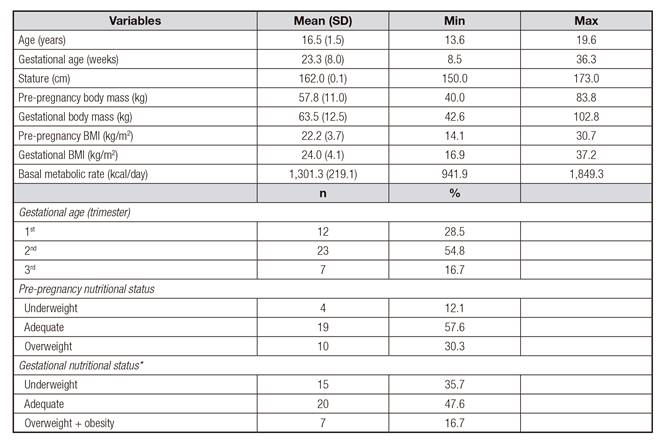
Data are from the first visit to the laboratory. SD: standard deviation; BMI: body mass index; BMR: basal metabolic rate. *Based on body mass index for gestational week (19).
Table II Physical and physiological characteristics according to pre-pregnancy nutritional status of the 42 pregnant adolescents in Niterói, RJ
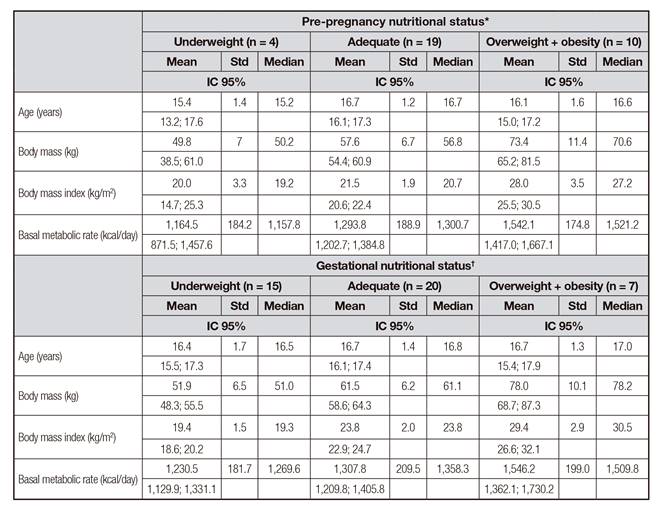
Data are from the first visit to the laboratory. *Based on body mass index for age (18). †Based on body mass index for gestational week 19.
Table II presents the physical and physiological characteristics of the pregnant adolescents according to the pre-pregnancy and gestational nutritional status. Independently of stages, there was a tendency of BMR to increase with increasing BMI. Energy intake decreased with increasing BMI and lipid intake remained approximately around 30% of EI in both pre-pregnancy and gestational nutritional status (Table III and Table IV). Dietary intake of sodium, vitamin A and zinc were higher than required except for pre-pregnancy underweight but they were insufficient for iron and calcium in both analyses (Table V and Table VI).
Table III Dietary intake of energy and macronutrients according to pre-pregnancy nutritional status of the 33 pregnant adolescents in Niterói, RJ
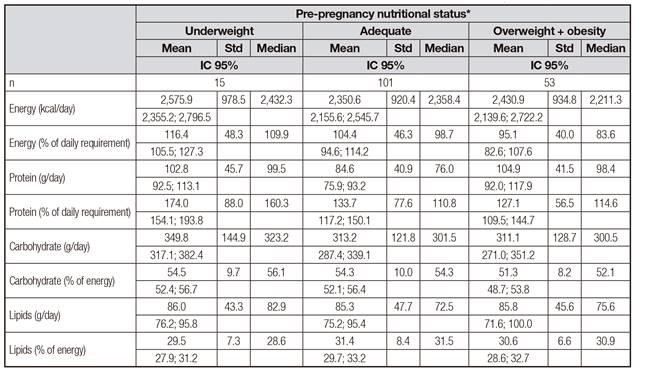
Data are from the repeated 24h dietary recalls. *Based on body mass index for age (18).
Table IV Dietary intake of energy and macronutrients according to gestational nutritional status of the 42 pregnant adolescents in Niterói, RJ
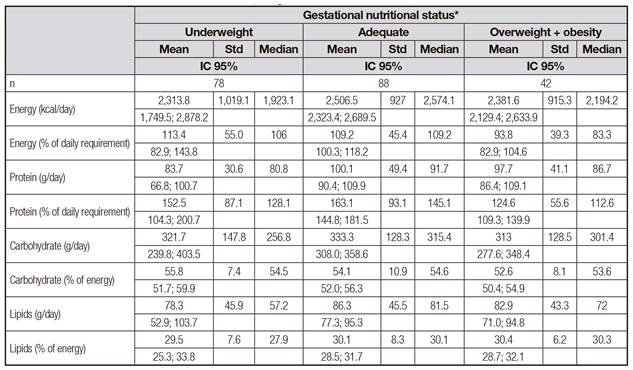
Data are from the repeated 24h dietary recalls. *Based on body mass index for gestational week (19).
Table V Dietary intake of micronutrients according to pre-pregnancy nutritional status of the 33 pregnant adolescents in Niterói, RJ
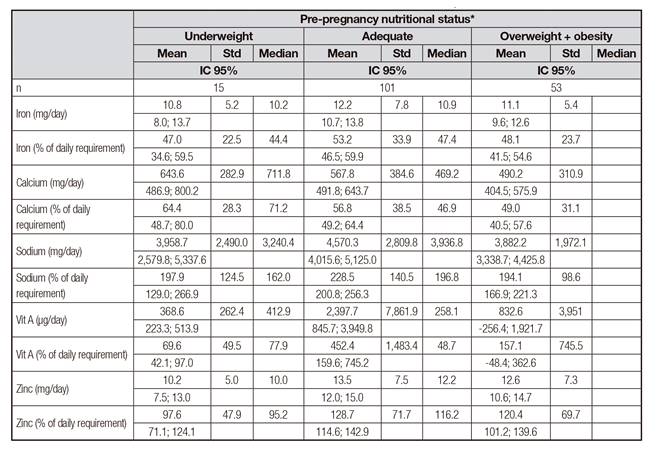
Data are from the repeated 24h dietary recalls. *Based on body mass index for age (18).
Table VI Dietary intake of micronutrients according to gestational nutritional status of the 42 pregnant adolescents in Niterói, RJ
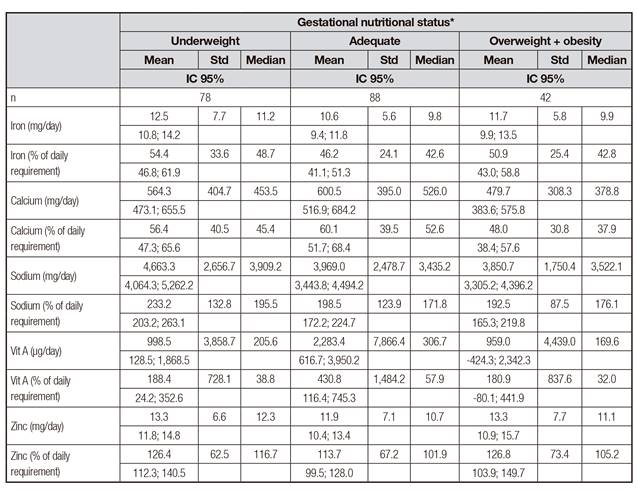
Data are from the repeated 24h dietary recalls. *Based on body mass index for gestational week 19.
Table VII Summary results of mixed linear models of % energy and protein daily requirement of the 42 pregnant adolescents in Niterói, RJ
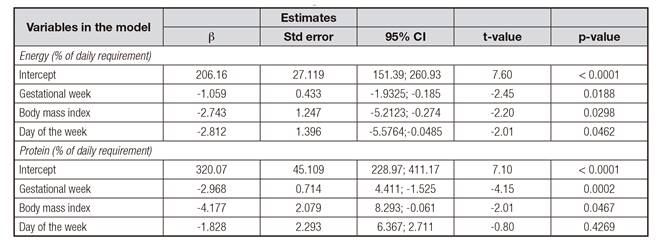
The mixed linear models were only significant for the percentage of energy and protein adequacy (Table VII). In both models the coefficients for GW, BMI and day of the week were negative.
DISCUSSION
The situation of social vulnerability of the present sample of pregnant adolescents is confirmed by the fact that most of them were registered in the Bolsa Família, a federal cash transfer program. This is in agreement with Vieira et al. 13, who reported that the situation of social and economic inequality does not appear as a direct consequence of adolescent pregnancy, but reflects the context of inequality in which the adolescents live. In the present study, favorably, just a few of the adolescents smoked but many maintained high bond with the baby's father, although most did not live together with their partner.
Pre-pregnancy overweight/obesity was more frequent than underweight but the opposite was observed for the gestational nutritional status. The pre-pregnancy results are consistent with the changes in the nutritional profile of the Brazilian female population in the last decades, characterized by an increase in the prevalence of obesity and a decrease in malnutrition 5). The high prevalence of underweight observed during pregnancy suggests that the Atalah's curve 19 used to classify the nutritional status of adolescents is inadequate. This method is adopted in the gestational weight policy in three other American countries 25, and in Brazilian adolescents it has been shown to overestimate the low gestational weight 26. The Brazilian Ministry of Health 8 recommends that the interpretation of the results obtained using this method be flexible for this specific group due to the possibility of many adolescents being classified as having low gestational weight. Thus, pregnant adolescents should be viewed as having some nutritional risk but careful attention must be given not to induce excessive weight gain. It is well documented that gestational obesity increases the chances of complications in the course of pregnancy 27 and has negative effects on the growth of the child in the short, medium and long terms 28.
Bianchi et al. 29 simulated the effects of pregnancy on the nutritional adequacy of the diet of women at childbearing age in the United States and France. Various nutrients (vitamins A and zinc) had reduced probability of adequacy induced by pregnancy. Calcium was not affected because their intake by women of childbearing age was already deficient. Further, the increase in EI by approximately 150 kcal daily did not imply improvement in the nutritional adequacy of the diet, except when the additional energy was provided by dietary sources based on fruit and dairy foods.
The diet of the present sample of pregnant adolescents was inadequate, characterized by excessive intakes of energy, protein and sodium and insufficient intakes of iron and calcium. Comparing the intake estimates obtained in this study with those in the literature, one can speculate that it is not difficult for the pregnant adolescents of low-income urban areas to meet the ER. Lee et al. 7 also observed positive energy balance (EB) in adult and adolescent pregnant women from Latin American countries of low and medium income including Brazil. On the other hand, in an area with a high concentration of social inequalities in the UK, the energy intake (2,148.0 ± 623.6 kcal/day) of 290 sedentary pregnant adolescents who were late in pregnancy was slightly lower (3%) than the recommendation 26. Since a third of them were overweight + obese, they may have been oriented to restrict the EI 30. Aspects inherent to the methods of assessment limit the comparability of results between studies.
The inadequacy of the micronutrient intake observed here confirms what was observed among the adolescent population in Brazil 31. On the other hand, the results of the present study contrast with the findings of Campos et al. (2013) 32, who investigated 139 pregnant adolescents attending prenatal care at a public maternity hospital in Rio de Janeiro. Estimates of calcium and vitamin A intakes, although inadequate, outweigh the values found in the present study. Low sodium intake, lower than the required, and less variability in nutrient intake, especially vitamin A, were also observed. This contrast may reflect aspects related to the use of a food frequency questionnaire, used in that study, which consisted of a list of only 20 food items.
In the present sample of pregnant adolescents, GW and BMI were inversely related to the percentage of adequacy of EI. One possible explanation is the reduction in dietary intake in order to control the gain of body mass after some inadequate high accumulation in the early stages of pregnancy. The presence of negative EB (percentage of adequacy of EI < 100%) observed in the overweight/obese adolescents is in agreement with data in nonpregnant individuals 33. This finding may have been due to underreporting of dietary intake, caused in part by the characteristics of the method of obtaining dietary intakes and by the inadequacy of the calculation of the ER. To our knowledge, this is the first study in which the ER of pregnant adolescents was estimated using measured BMR values. The lack of studies on energy metabolism of adolescents does not allow the development of specific procedures and methods for ER determination in this population, a gap recognized by the international agencies that establish the nutritional requirements 1. The use of measured BMR data in this study made it possible to obtain closer estimates of ER for the pregnant adolescents, since this is the metabolic component that contributes the most to total daily energy expenditure. Usually, studies evaluate the dietary adequacy of pregnant adolescents using either individual dietary pattern or BMR estimated by equations as suggested by international health/nutrition agencies 1. In addition, there is no specific anthropometric method for the nutritional assessment of pregnant adolescents. To this end, the positive EB observed in the adolescents with adequate nutritional status of the present investigation, even though small, considering both pre-pregnancy and gestational nutritional status, is of concern within the context of the obesity epidemic and requires doubled attention in health surveillance actions with the use of appropriate methods for its determination.
Unlike energy and macronutrients, minerals and vitamins are nutrients whose adequacy seems harder to achieve during pregnancy. Except for sodium, these nutrients are scarce in the diet when the dietary patterns are characterized by industrial products with low quantity and little variation in natural vegetable sources and, on the contrary, with high energy density 29. This may explain the inadequate intakes of iron and calcium observed in the present pregnant adolescents, as well as among other Latin American pregnant 7) women, for whom the intake of zinc, iron and calcium was also inadequate. In the present study, the higher protein intake may have led to adequate zinc intake since the main sources of this mineral are foods, such as bovine, chicken, fish and beans, among others.
Regarding calcium, only a third of the pregnant adolescent reached the recommendation. Inadequacy was observed in the three categories of pre-pregnancy and gestational nutritional status and may be related to insufficient intake of milk and dairy products, since these foods, the main sources of calcium, are one of the groups less consumed by the Brazilian adolescent population, presenting an estimated inadequacy in more than 90% of the population 31. Calcium has a preventive role for some chronic diseases, including arterial hypertension, whose presence during pregnancy puts at risk maternal and fetal health 27.
The iron requirement during pregnancy increases almost three-fold and is difficult to achieve by dietary intake. The prevalence of inadequacy among pregnant adolescents was critical, similar to what was found in English adolescents 30. According to a national dietary survey conducted in Brazil in 2008, the diet of adolescents between 14 and 18 years of age presented 21.7% of inadequacy, twice that observed in the 10-13 year age range 31.
The high variability observed in vitamin A intake was relevant, especially among pregnant women with adequate nutritional status. This high variability can be explained by the ingestion of certain foods with a high concentration of the vitamin, such as viscera; their intake may not be regular but is encouraged in dietary counseling during prenatal care 8.
Sodium is an important marker of food quality and high intake of this mineral may be related to the ingestion of ultra-processed foods such as snacks, processed meats, snack foods, biscuits and soda, among others. The median sodium intake by the pregnant adolescents exceeded the estimates of the adolescent female population in the southeastern Brazilian region (2,815.0 mg for the 10-13 year age group and 2,774.0 mg for the 14-18 year old age group) 31.
This study can contribute to a better understanding of relevant aspects of nutrition and health of pregnant adolescents cared for in primary health care units. An important aspect of the study was the possibility of measuring BMR in the pregnant adolescents, making it possible to calculate the ER as accurate as possible. The number of R24h obtained in the present study covered a wide period of time, as well as a variety of foods and preparations, despite the small sample size. Nutritional anthropometric assessment during gestation proved to be a critical issue given the limitations of the criteria recommended and adopted. One of the possible limitations of this study is the presence of information bias. The effects of socioeconomic level and nutritional status on self-reported IE were observed in pregnant and adult pregnant women from developed countries 34 where EI underreporting was positively associated with socioeconomic status and excessive BM gain. In the present study, this effect may have been neutralized or minimized due to the low socioeconomic class to which they all belonged.
It is expected that the knowledge generated herein may be of practical importance for professionals involved in nutritional care of pregnant women, who must consider the specificities of adolescence pregnancy, without losing sight of the dimension that the nutrition/food has in the life of the subjects. At the local level, educational actions must be made in light of the dietary counseling based on the approach through dialogue with the adolescents, to understand the reality of their life, considering their beliefs, cultural values, material conditions of access and, especially, their relative autonomy 35. The situations of excessive intake should also be worked under a more comprehensive understanding of food, although the need for dietary restriction is pressing.
CONCLUSION
This study found that adolescents seen during prenatal care in primary care units living in disadvantageous socioeconomic settings have excessive intake of energy, protein and sodium. The dietary intake was insufficient for some important micronutrients such as iron and calcium. There is a negative association between the adequacy of energy and protein intakes with GW and BMI when considering inter and intra-subject variability. The pre-pregnancy overweight and obesity levels as well as the high intake of sodium are reasons for concern due to future implications to the health of the adolescents. The official Brazilian recommended criterion for anthropometric assessment in pregnancy of adolescents may not be adequate for pregnant adolescents.

