










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Having excess fat, especially being overweight or obese, is associated with numerous chronic diseases and premature death and places strain on healthcare systems worldwide 1. According to the 2016 National Half-Way Health and Nutrition Poll (ENSANUT-MC from its acronym in Spanish), the prevalence of adults (20 years of age or older) who were either overweight or obese in Mexico was 72.5%, and the prevalence was higher in northern region of the country 2.
Obesity is a multifactorial condition 3 defined by the excessive accumulation of body fat, which can potentially lead to serious health consequences 4. Unhealthy eating habits represent the primary behavior associated with obesity and are considered as a result of the nutritional transition produced by technologic and economic development and changes in daily life. Major changes in daily habits, work environments, and access to food have promoted an increase in the consumption of foods and beverages with high sugar and fat content 1.
Ciudad Juarez, which borders the United States, has adopted many eating habits from its neighboring country, specifically the consumption of calorically dense foods, and the region has become one of the most vulnerable to obesity 5. Individuals having higher availability in fats and sugars and a predisposition to obesogenic behaviors have promoted the excessive deposition of body fat 6,7. However, individual differences in the psychological state and environment may also lead to the consumption of highly palatable foods rich in sugars and fats. This indicates that there are psychological factors, such as craving, that influence control over the consumption of these foods 8.
Food cravings refer to the almost irresistible desire or urge for eating certain types of foods 9,10 and furthermore, may initiate and promote addictive behaviors around palatable foods, causing a predisposition in individuals towards obesity 8. The most palatable foods, generally, consist of high sugar and fat contents and are sometimes referred to as "junk food" 11,12. This type of foods may have addictive properties and have been associated with cravings 13.
Behaviors associated with food cravings include lack of control of over eating 14, invasive thoughts about food, anticipation for a sense of reward from eating 15, cravings and guilt 16, and excessive eating 17. Different internal and environmental stimuli can trigger these behaviors. Individuals with obesity have been seen to anticipate a sense of relief from psychological conditions in response to food (reward), while people with normal weight showed no signs of such behavior 18. Furthermore, self-report from individuals addicted to food highlight that eating relieves them from feelings of depression, anxiety, and stress. These findings suggest psychological traits are a moderating factor in overeating habits and obesity risks 19.
Lack of control over satiety and hunger leads to overconsumption of calories and, in return, growth of adipose tissue 20. Activation in hedonic and reward circuitry and impaired functionality in areas related to executive functions have been indicated in studies of adolescents. Those with obesity exhibit a lower capacity to control sugar intake as compared to adolescents with normal weight 21. Likewise, evidence demonstrates that cravings for sugar and fat can explain excessive consumption. Within the body, sugars are transformed into fat and increase the accumulation of adipose tissue 7 determined in 2009 by Duffey et al. 6. The consumption of sugary drinks and foods is also highly associated with an increased risk of obesity 22. Furthermore, fat deposition in adipose tissue happens easily and requires low energy expenditure exacerbating the development of overweight and obesity 20.
The current study aims to determine the magnitude of the positive association between cravings, sugar and fat consumption, and body composition in a sample of Mexicans from the Mexican-US border. Specifically of interest are cravings as measured from trait and state food cravings questionnaires and how they associate with sugar and fat consumption and body composition measures. Likewise, it is important to determine the characteristics of cravings which are associated with individuals' weight status, normal weight as compared to overweight/obese.
MATERIALS AND METHODS
SAMPLE
The sample included 159 young adults, all residents of Ciudad Juarez, with an average age of 27.95 (± 6.19). Participants were recruited through flyers placed throughout the University. Participants with obesity caused by illness or pharmacological treatment were excluded.
INSTRUMENTS
Participants were evaluated at a nutrition clinic at the Biomedical Sciences Institute (ICB from its acronym in Spanish) of the Autonomous University of Ciudad Juarez (UACJ from its acronym in Spanish). First, individuals completed an informed consent form in compliance with the approval from the Ethics and Bioethics Committee of UACJ. Participants were instructed to fast prior to the evaluation and avoid drinking water or exercising. Each participant was subjected to electrical bioimpedance and had their waist circumference measured. The nutritional and psychological interview was carried out in a consulting room at the nutrition clinic by qualified personnel.
CRAVINGS
The Food Cravings Questionnaires Trait (FCQ-T) and State (FCQ-S), developed by Cepeda-Benito et al. (2000), were used to measure food craving. The FCQ-T measures the intensity of desires for eating characteristic to individuals, as a permanent trait, in a Likert scale with six response options, and is composed of 39 items divided by nine factors (Spanish version). For the purposes of this study, a total of six factors resulted confirmative after a factorial analysis was conducted: a) guilt from cravings and/or for giving in to them, where the frequency of guilt feelings from eating or not resisting certain foods is measured; b) anticipation of positive reinforcement that may result from eating, where the positive emotions resulting in anticipation to eating certain foods are measured; c) anticipation to emotions caused by eating, where the frequency with which the participant eats when feeling certain emotions is measured; d) lack of control over eating, which measures the frequency with which an individual loses control over eating; e) thoughts or preoccupation with food, where the frequency with which an individual thinks about food is measured; and f) craving as a physiological state, measuring the frequency with which hunger is felt 23.
The FCQ-S measures the intensity of desires for eating in a specific moment (depending on the state). It is constituted by 15 items distributed among five factors (Spanish version). For the purposes of this study, only three were used after factorial analysis proved them confirmative: a) an intense desire to eat, which measures the urge to eat in that moment; b) craving as a physiological state, which measures hunger at that moment; c) anticipation of relief from negative states and feelings as a result of eating, which measures anticipation for relief from eating. These factors are measured in a Likert scale with five response options 23.
SUGAR AND FAT INTAKE ANALYSIS
Food consumption was measured via participants recalling intake from the past 24-hours; from this recall sugar and fat intake percentage was obtained. Additionally, the food consumption frequency questionnaire was used to determine the average sugar and fat intake. The food equivalence table from the Mexican system was used to quantify the amounts of sugars and fats consumed.
BODY COMPOSITION
Body mass index (BMI) and body fat percentage (BFP) were obtained using a Seca® mBCA electrical bioimpedance equipment and Seca® analytics mBCA 115 software for data measurement and analysis. The sample was classified according to body mass index in low weight (BMI < 18.5), normal weight (18.5 to 25), overweight (25 to 30), and obesity (> 30). These classifications are from the official Mexican norms (NOM from its acronym in Spanish) in its 2010 version for overweight and obesity 24. Body mass percentage was classified according to the cut points specified for the equipment, from the study by Gallagher et al. (2000) 25.
Waist circumference (WC) was measured according to specifications established in the 2016 National Institute for Public Health (INSP from its acronym in Spanish) manual 26. It was classified in low and high risk for health using the cut points established by the Latin American Diabetes Association (ALAD from its acronym in Spanish), considering as low risk those values inferior to 88 cm in females and 94 cm in males 27.
STATISTICAL ANALYSIS
Pearson correlations, analysis of variance and multiple logistic regression analyses were performed using the IMB SPSS v.20 software. Comparisons between groups were carried out by dividing the sample population based on body mass index, body fat percentage, and waist circumference, according to the previously mentioned cut points.
Multiple logistic regression analyses were carried out to predict overweight/obesity according to BMI, body fat percentage and risk by waist circumference, considering craving variables for the model, sugar and fat intake, gender, and age. For this model, overweight/obesity variables were dichotomized and the female gender was considered as a risk factor.
RESULTS
DESCRIPTIVE
The frequency from the sample, according to BMI was: 3.1% low weight (LW), 40.9% normal weight (NW), 32.1% overweight (OW), and 23.9% obesity (O), with a BMI mean of 26.69 (s = 5.94). As for groups, according to BFP, there was: 2.5% low percentage (LP), 40.9% normal percentage (NP), and 56.6% high percentage (HP), with a mean of 32.11 (s = 8.56). Finally, the average WC was of 86.81 cm (s = 15.33) with 54.5% of the total sample population showing high circumference (HC) and 45.5%, normal (NC). It is worth noting out that participants with low BMI and BFP were omitted since they are not of interest for the purposes of this study.
CORRELATIONS
Craving and obesity
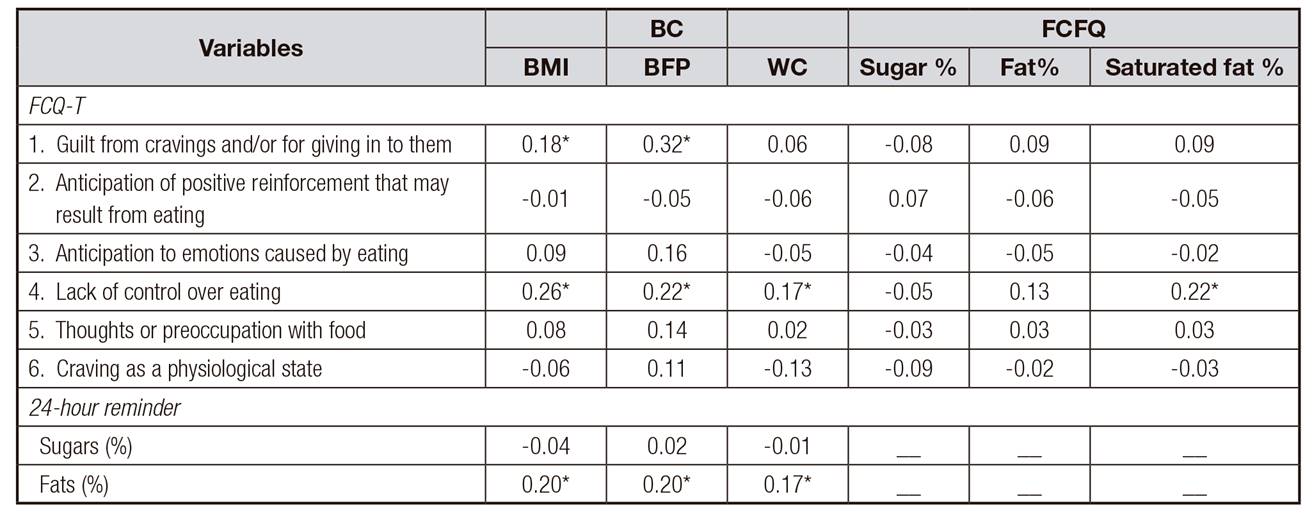
The FCQ-T results (Table 1) show positive correlations which are statistically significant with lack of control over eating scale and BMI (r = 0.26, p < 0.01), BFP (r = 0.22, p < 0.01), and WC (r = 0.17, p < 0.05). A positive correlation was also found with the guilt for guilt from cravings and/or for giving in to them in scale and BMI (r = 0.18, p < 0.05) and BFP (r = 0.32, p < 0.001). The FCQ-S questionnaire did not produce any significant statistical correlations with body composition.
Sugar and fat intake and obesity
BMI, as well as BFP and WC, were positively correlated with fat intake measured by the 24-hour reminder (Table 1). BMI reports (r = 0.20, p < 0.05), BFP (r = 0.20, p < 0.05), and CC (r = 0.17, p < 0.05). Results demonstrate that the higher the fat intake, the higher the BMI, BFP, and WC. However, there were no statistically significant correlations to sugar and saturated fats intake measured through the consumption frequency questionnaire, or with sugar intake measured through the 24-hour recall.
Sugar and fat intake and cravings
A small positive correlation was also found (Table 1) between saturated fat consumption (measured by frequency of consumption) and the lack of control over eating from the FCQ-T (r = 0.22, p < 0.01). No significant correlations were found between the FCQ-S and sugar and fat intake.
Analysis of variance and the Student's t-test
Body composition
In the comparison between groups by BMI (Table 2), the results showed a statistically significant difference in four FCQ-T factors: guilt from cravings and/or for giving in to them (F [2,142] = 3.88, p < 0.05, d = 0.61), thoughts or preoccupation with food (F [2,143] = 3.98, p < 0.01, d = 49) (in these cases the obese group scored higher than the overweight group). In craving as a physiological state (F [2,143] = 4.96, p < 0.01, d = 0.63) the normal weight group displayed higher scores than the overweight group. It is worth noting that in lack of control over eating the normal weight group scored higher than overweight (F [2,143] = 6.34, p < 0.01). FCQ-S results showed significant differences in the anticipation of relief from negative states and feelings as a result of eating factor (F [2,139] = 4.29, p < 0.05, d = 0.56) where the normal weight group displayed higher scores than the overweight group. No significant differences were found in sugar and fat consumption.
Table II. ANOVAS between BMI groups and the Trait and State FCQ
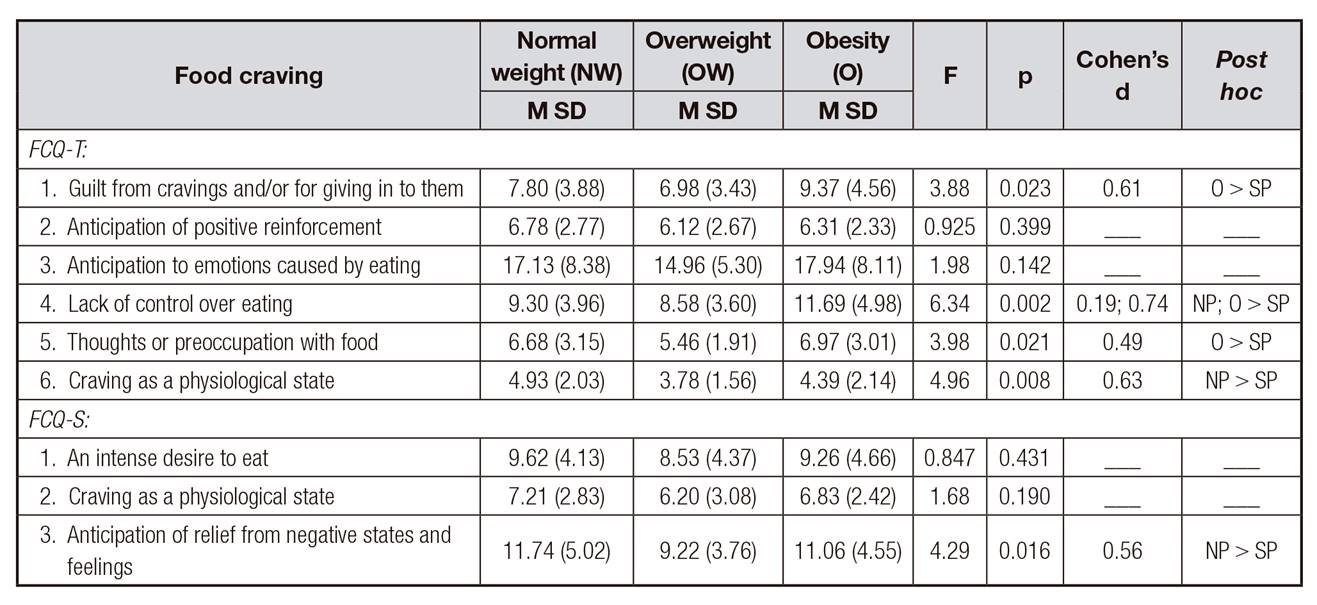
BMI: body mass index; FCQ-T: Trait Food Cravings Questionnaire; FCQ-S: State Food Cravings Questionnaire.
On the other hand, significant differences from the sample divided by the BFP (Table 3) were observed in craving as a physiological state (t [145] = 1.98, p < 0.05, d = 0.34) where the normal weight group displayed the highest score. No significant differences were found in FCQ-S results or in sugar and fat consumption.
Table III. Student's t-test between BFP and the FCQ-T

BFP: body fat percentage;
FCQ-T: Trait Food Cravings Questionnaire. According to the Levene's test in all comparisons, equal variances are assumed.
Analysis by WC demonstrated no significant differences in craving behavior, unlike fat intake according to the 24-hour reminder (Table 4) where the cardiovascular risk group (high WC) showed higher intake than normal WC (t [152] = -2.95, p < 0.01, d = 0.48).

MULTIPLE LOGISTICAL REGRESSIONS
The multiple logistical regression was used to predict overweight and obesity according to BMI, BFP, and risk from WC; according to the Hosmer and Lemeshow test, the three models showed acceptable model fit statistics (p = 0.233, p = 0.486 and p = 0.612, respectively).
Results demonstrated that the regression model to predict overweight/obesity from the 38% according to Cox and Snell's R2 to the 51.1% according to the Nagelkerke's R2 (p < 0.001). Specifically, risk factors observed were: higher lack of control over eating (OR [1] = 1.211, p < 0.05); higher fat intake (measured by 24-hour reminder) (OR [1] = 1.081, p < 0.01); gender (female) (OR [1] = 10.010, p < 0.001); and older age (OR [1] = 1.176, p < 0.001), as observed in Table 5.
Table V. Logistic regression to predict obesity risk
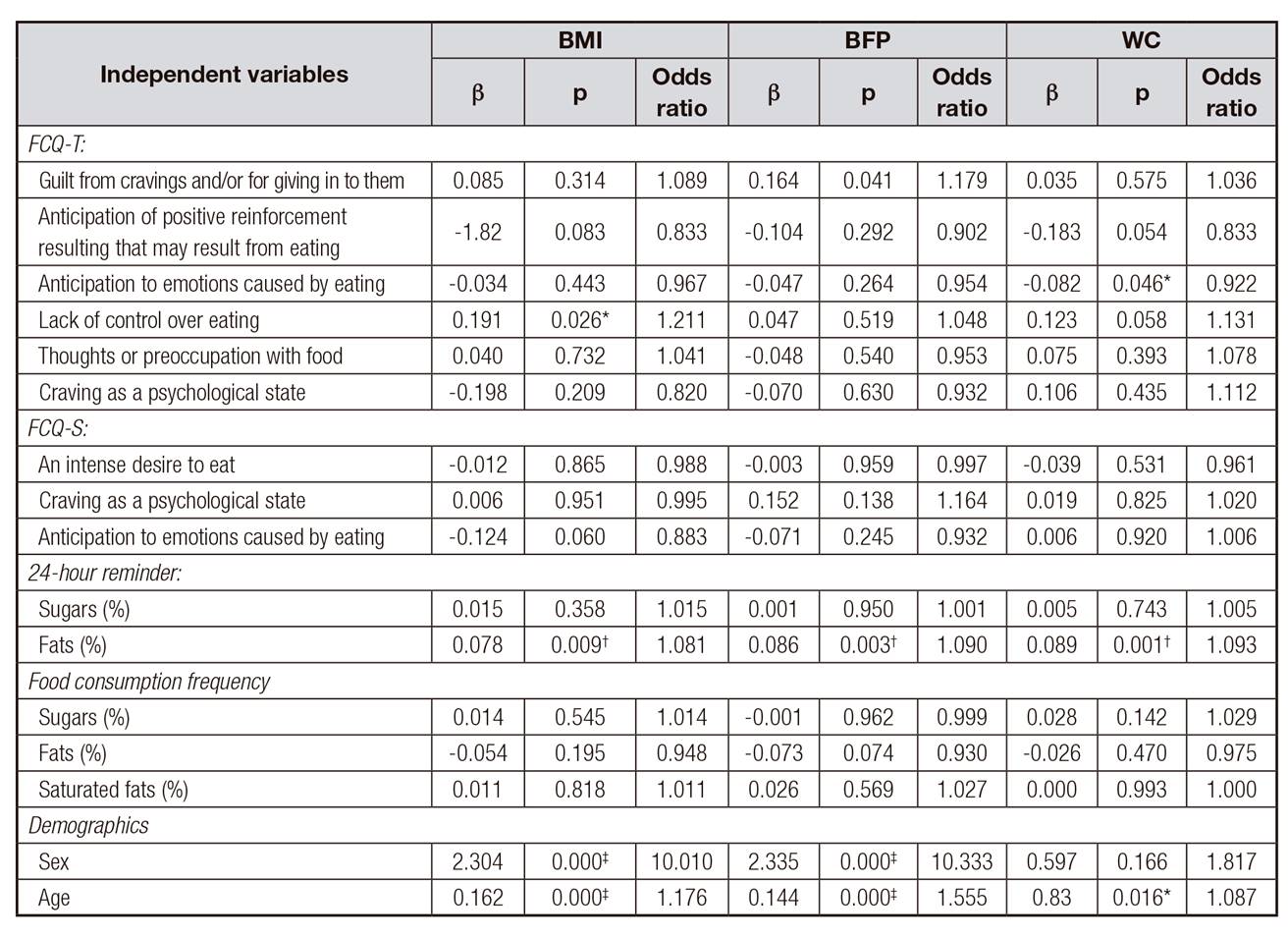
FCQ-T: Trait Food Cravings Questionnaire; FCQ-S: State Food Cravings Questionnaire; BMI: body mass index; BFP: body fat percentage; WC: waist circumference; β: Beta.
*p < 0.05;
†p ≤ 0.01;
‡p < 0.001.
Risk factors found from high BFP (Table 5) were: guilt from cravings and/or for giving in to them (OR [1] = 1.179, p < 0.05); high fat intake (measured by 24-hour reminder) (OR [1] = 1.090, p < 0.01); gender (female) (OR [1] = 10.333, p < 0.001) and older age (OR [1] = 1.155, p < 0.001). Variables predict risk for having high BFP from 34.8% to 46.7% (p < 0.001) according to Cox and Snell and Nagelkerke, respectively.
According to the results obtained (Table 5), the predicting percentage from variables accounted for risk from waist circumference oscillates between 20.9% (Cox & Snell) and 27.9% (Nagelkerke), p < 0.05. Risk factors for this variable are: higher fat intake (measured by 24-hour reminder) (OR [1] = 1.093, p ≤ 0.001) and older age (OR [1] = 1.087, p < 0.05). Besides, anticipation for emotions that might be caused by eating was identified as protector factor.
DISCUSSION AND CONCLUSIONS
The presence of craving towards sugars and/or fats makes one more susceptible to the development of obesity. If excessive consumption of these foods causes craving, it will be difficult to achieve a change in eating habits without adequate psychological intervention.
Larger amounts of sugar and fat intake were found to be associated with obesity 4. Observations made in this study confirm that higher fat intake represents a higher risk for high BMI, BFP, and WC. However, no evidence was found of a correlation between sugar and these factors. Certain properties in fats make them a risk factor for the development of obesity since they provide a higher caloric value than carbohydrates and proteins. Additionally, deposition of fats in adipose tissue represents less effort and energy expenditure to the body. Sugars, on the other hand, undergo metabolic processes that require higher energy expenditure to become fats, which might explain the absence of correlation 20. Significant differences were found in fat intake in the WC group, which suggests a high tendency to fat deposition in the core area, consequentially increasing cardiovascular risks.
Evidence shows the relationship between obesity and the consumption of foods rich in fats and sugars which are highly palatable and are associated with craving. As mentioned before, the irresistible desire or urge to eat a particular food is referred to as craving 10 and is one of many disorders associated to the regulation of food consumption. Craving behaviors like lack of control 14 and overeating represent a risk factor for overweight and obesity 17. Another craving-related behavior is having persistent thoughts about food which push individuals towards its consumption. Excessive consumption triggers a feeling of guilt and develops a vicious cycle influenced by environmental stimuli 28.
Results in this study linked BMI and BFP to lack of control over eating and guilt from cravings and/or for giving in to them. Participants with higher BMI and BFP scored higher in both instances. Besides, lack of control came up as a risk factor for overweight/obesity and guilt increases the risk of having a higher BFP. These results match previous reports by Moreno et al. (2009) 14 and Fletcher et al. (2007) 16.
A higher score from the overweight group in comparison to the obese group in guilt over craving, lack of control over eating, and thoughts about food suggest craving can be a determinant factor for obesity. However, a recent discovery revealed the normal weight group got high scores in lack of control over eating and greater physiological hunger (not craving). These results were unexpected since, theoretically, individuals suffering overweight and obesity present higher levels of food craving 17,29. Further analysis on the normal weight group revealed the higher the hunger levels, the greater the lack of control (r = 0.61, p < 0.01). One possible explanation might be that while the physiological state (physiological hunger) influences lack of control over eating, consumption might not be excessive because it is a physiological stimulus. This could also explain this group's lack of predisposition for obesity.
Hunger activates the decision-making system. If this need is not satisfied, it can trigger behavior associated to food craving like lack of control. A study on people with normal weight found that food-related stimuli triggered food ingestion but not loss of control over it 30. However, a different study found that individuals with normal weight and obesity respond similarly to food rich in calories, unlike those involved in a weight loss program. This suggests groups going through weight loss intervention present cognitive strategies that allow them to inhibit junk food consumption and maintain their weight 31, potentially explaining this study's results on lack of control among the normal weight and obese population.
According to results, it can be argued that the normal weight group is vulnerable to suffer overweight and obesity. However, among this group, the presence of physiological hunger as a trait was notable, showing no signs of thoughts of food or guilt over craving like the obese group. Arguably, lack of control in the obese group is linked to addictive behavior (food craving) unlike the normal weight group.
Another interesting finding is that, contrary to expectations, the overweight group did not display craving behavior. A possible explanation is that this group, when hungry or craving, satisfies this need quickly, avoiding intrusive thoughts 31 triggered by food craving like intense desires to eat, lack of control, or anticipation for relief from eating 32. Matching this study, researchers have found that overweight people exposed to stimuli from palatable foods felt motivated to eat them but not in high quantities 33, suggesting they do satisfy such urges quickly without presenting lack of control or guilt.
The obesity group, on the other hand, presented greater craving behavior like thoughts of food, lack of control, and guilt as expected. Thoughts about food can trigger lack of control over eating and guild for craving 34. However, no signs of addictive behavior induced by mood swings were identified, unlike other studies such as those previously mentioned. This suggests thoughts of food, above mood swings, trigger food craving 35.
Waist circumference was only positively correlated to lack of control over eating. This correlation is quite small; however, no reports of such phenomena are known by this association. Additional research on the subject is recommended since waist circumference is currently considered to be one of the main risk indicators for cardiovascular disease, regardless of body fat percentage and body mass index.
An important finding is represented by the lack of correlations between sugar and fat intake and craving behavior. This suggests these two variables are independent factors for the development of obesity since craving behavior was associated with obesity can be considered a determinant factor. Meanwhile, the relationship between craving and diet cannot be discarded since the former could result from consumption of different types of food. Another factor potentially influencing this phenomenon is inadequate reporting of sugar and fat intake. This might occur because of a distorted perception of the diet and eating habits among other factors 36. Some studies have reported higher BMI values have been associated with perception of reduced consumption of foods 37.
This study opens a door for future lines of investigation, one of which would be to investigate how cravings may affect food portion size perception among people with obesity. Another point of interest would be to investigate what causes the lack of control over eating in people with normal weight. It is known that long periods of fasting tend to condition overcompensation in the following meal, particularly happening in expense of fats. It is also recommended to study food craving under fasting conditions or after eating and analyze responses from different groups (with and without obesity). Another point of interest is the evaluation of reactions to craving in overweight, obesity, and normal weight groups facing stimuli from palatable foods to identify craving behavior associated to specific foods.

