










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Childhood obesity is reaching epidemic proportions throughout the world 1 and has been declared a global public health problem. The increase has been associated with a greater presence of cardiometabolic risk (CMR) 2, affecting children's overall development and quality of life.
Lower physical fitness levels in children are associated with the development of cardiometabolic risk factors 3. By contrast, children and adolescents with high cardiorespiratory fitness (CRF) are exposed to lower CMR and have a healthier cardiovascular profile 4. For this reason, CRF is a basic component of development at this stage of life 5. Likewise, higher muscular strength is inversely related to the risk factors for cardiovascular disease in adults, and has proved to be a powerful protector of mortality and life expectancy 6. Developing assessments of children's health-related physical fitness at an early stage is a priority 7, since improving physical fitness provides protection against chronic illnesses 3.
Various large-scale population studies have highlighted clear associations between physical activity (PA), obesity and CMR in children 8. Overweight or obese children with insufficient levels of PA are at significantly greater risk of elevated SBP than their non-overweight and sufficiently active counterparts 9. A systematic review that evaluated the relationships between PA and health indicators in school-age children and young people reported that, overall, total PA is favorably associated with physical, psychological/social, and cognitive health indicators 10. However, despite the known benefits of PA, levels of practice among children remain very low 11.
High blood pressure is a predictor for the later development of hypertension and cardiovascular risk factors 12. Hypertension during childhood is frequently under-diagnosed; however, it shows a relationship with being overweight and obese 13, and is also considered to be the most important risk factor worldwide for cardiovascular accidents 14. Likewise, higher recreational and non-recreational PA is associated with a lower risk of mortality and cardiovascular events in individuals from low-income, middle-income, and high-income countries 15. Therefore, the examination of PA levels should be a priority.
The objective of the research was to determine the relationship between health-related physical fitness and physical activity levels, blood pressure, and anthropometric parameters for different weight statuses of Chilean schoolchildren.
MATERIAL AND METHODS
PARTICIPANTS
Participation in the study was voluntary and the sampling type was convenience. The participants were 605 schoolchildren: 272 girls and 333 boys (45% and 65% respectively), with a mean age of 12.00 ± 1.23 years, belonging to public education centers in the Araucanía Region, Chile, and having similar socioeconomic status (SES) and similar characteristics according to the Physical Education National Study 16.
The inclusion criteria were: presenting informed consent of the parents and the assent of the participant, belonging to an educational center and being aged between eleven and 13 years.
The exclusion criteria were: presenting a musculoskeletal disorder or any other known medical condition which might alter the participants' performance and health during the physical assessments, or having physical, sensorial or intellectual disabilities.
The first population included 637 in the enrolment stage. After applying the inclusion/exclusion criteria, a total of 32 were excluded.
The investigation complied with the Declaration of Helsinki (2013) and was approved by the Ethics Committee of University of La Frontera, Chile. The tests were explained to all the participants before the study began and they were asked to abstain from intense exercise for 48 hours before the study.
MATERIAL
Anthropometric assessment
The participants' body mass (kg) was measured using a set of Tanita(r) scales, model Scale Plus UM - 028 (Tokyo, Japan); the children were weighed in their underclothes, without shoes. Their height (m) was estimated with a Seca(r) stadiometer, model 214 (Hamburg, Germany), graduated in millimeters. Body mass index (BMI), calculated as the body weight divided by the square of the height in meters (kg/m2), was used to estimate the degree of obesity. The BMI is shown in the growth table of the Centers for Disease Control and Prevention, Overweight and Obesity (CDC) for the corresponding age and the sex-related percentile. Childhood obesity is defined as having a BMI equal to or greater than percentile 95, and overweight as having a BMI equal to or greater than percentile 85, among children of the same age and sex 17.
Waist circumference (WC) was measured using a Seca(r) tape measure, model 201 (Hamburg, Germany), at the height of the umbilicus 18.
To measure % body fat (% BF), the tricipital fold and the subscapular fold (Lange Skinfold Caliper, 102-602L, Minneapolis, USA) was used, and the Slaughter's formula 19 was applied:
Girls: % BF = 1.33 (tricipital + subscapular) - 0.013 (tricipital + subscapular) 2 - 2.5
Boys: % BF = 1.21 (tricipital + subscapular) - 0.008 (tricipital + subscapular) 2 - 1.7
Physical fitness
To evaluate the health-related physical fitness of the children we used the ALPHA-fitness test battery 20.
Lower-body explosive strength was assessed by a standing long jump test (SLJ), consisting of jumping a distance with both feet together. The child stood behind a marked line and jumped as far as possible 21. Each child jumped twice and the best result was recorded. Higher scores indicate better performance.
The handgrip strength was used to measure upper body strength, through a hand dynamometer (TKK 5101 Grip D; Takei, Tokyo, Japan). The test consists in holding a dynamometer in one hand and squeezing as tightly as possible without allowing the dynamometer to touch the body; force is applied gradually and continuously for a maximum of 3-5 seconds 22. The test was performed twice and the maximum score for each hand was recorded in kilograms. The average of the scores achieved by the left and right hands was used in the analysis. Higher scores indicate better performance.
Cardio-respiratory fitness (CRF) was measured by the progressive 20 meter shuttle run test 23. The participants were required to run between two lines 20 meters apart while keeping pace with audio signals emitted from a pre-recorded CD. The test has been validated among Chilean schoolchildren, and has been utilized in the Physical Education National Study 16. The results were unified according to the Leger test protocol, and the maximal oxygen consumption (VO2max) was calculated using Leger's equation 23. Higher VO2max indicates better CRF. The perception of effort was recorded using the modified 0-10 Borg scale.
Physical activity levels
To measure the PA levels the Physical Activity Questionnaire for Children (PAQ C) was used. The minimum score from all the responses is 10 points and the maximum 40; a higher score indicates a higher physical activity level 24. The answers to questions 1 and 10 were excluded from the total score.
Blood pressure
The systolic blood pressure (SBP) and the diastolic blood pressure (DBP) were measured on two occasions after 15 minutes' rest following international standards 14, using an OMRON(r) digital electronic monitor, model HEM 7114 (Illinois, USA). To classify high blood pressure we used the "Fourth report on the diagnosis, evaluation and treatment of high blood pressure in children and adolescents" 14. Pre-hypertension was defined as arterial pressure ≥ percentile 90 and < percentile 95; hypertension was defined as arterial pressure ≥ percentile 95 14.
Procedures
The trained research assistants (four evaluators) visited the selected educational centers during the Chilean school year of 2017 and carried out the evaluations of children whose parents had consented and who had given their own assent. The evaluations were carried out in a favorable space facilitated by the educational center with optimal temperature and reliable privacy. The evaluations were carried out during physical education classes in the morning.
Statistical analysis
SPSS 23.0 software was used for the analysis (IBM, SPSS statistics). The normal distribution of the data and the equality of the variances were checked using the Kolmogorov-Smirnov test and Levene's contrast, respectively. The variables were expressed as mean ± standard deviation (SD). Sex differences were determined by one way analysis of variance (ANOVA). The comparison by nutritional state was done by ANOVA, and the post hoc analysis using Bonferroni's method. To establish the relationship between the variables, partial correlations adjusted by sex were carried out. The Chi-square test was applied to compare proportions between groups for blood pressure and weight status. Values of p < 0.05 were considered as statistically significant.
RESULTS
No differences in proportions by weight status were found between boys and girls (p > 0.05). In the comparison by sex, boys were taller and had better performance for CRF, VO2max and SLJ (p < 0.001). Boys showed higher levels of PA than girls (p = 0.034) (Table 1).
Table I Description of the study variables in schoolchildren

The data shown represent the mean ± DS. Values of p < 0.05 were considered as statistically significant. BMI: body mass index; WC: waist circumference; BF: body fat; VO2max: maximal oxygen consumption; SBP: systolic blood pressure; DBP: diastolic blood pressure.
The percentage of the population located in the overweight and obesity groups was 45% (n = 272), and it was found that the obese schoolchildren presented higher values for all the anthropometric parameters (p < 0.05). For CRF, schoolchildren with normal weight presented better results than those in the other groups. For the SLJ (p < 0.001) obese schoolchildren reported the lowest levels of PA (p < 0.001) (Table 2).
Table II Comparison of anthropometric variables and physical condition by weight status

The data shown represent the mean ± DS. Values of p < 0.05 were considered as statistically significant. Different symbols in superscript indicate significant differences (p < 0.05) in comparisons between groups. BMI: body mass index; WC: waist circumference; BF: body fat; VO2max: maximal oxygen consumption; SLJ: standing long jump test.
BPs were higher in obese schoolchildren (p < 0.001) (Fig. 1).
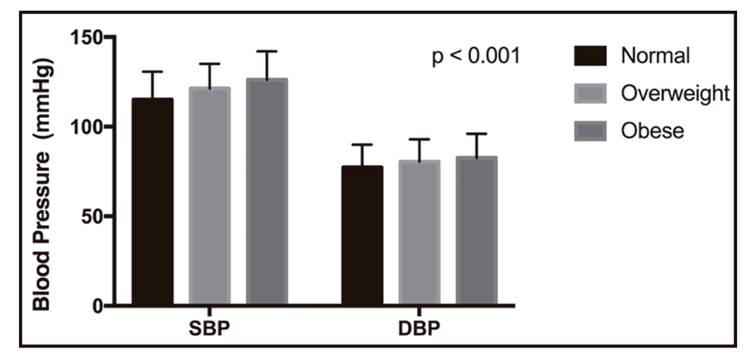
Figure 1 Comparison of systolic blood pressure and diastolic blood pressure by weight status. SBP: systolic blood pressure; DBP: diastolic blood pressure.
Physical fitness was inversely associated with SBP: VO2max (r = -0.26, p < 0.001), SLJ (r = -0.11, p = 0.007) and handgrip strength (r = -0.10, p = 0.021); and positively associated with PA: VO2max (r = 0.31, p < 0.001), SLJ (r = 0.18, p < 0.001), and handgrip strength (r = 0.26, p < 0.001). Moreover, VO2max and SLJ were inversely related to BMI and WC (p < 0.05) (Table 3).
Table III Correlation of variables adjusted for sex

BMI: body mass index; WC: waist circumference; BF: body fat; SBP: systolic blood pressure; DBP: diastolic blood pressure; PA: physical activity; VO2max: maximal oxygen consumption; SLJ: standing long jump test.
Table 4 shows that the group of obese schoolchildren contained the highest proportion of individuals with hypertension; the group of overweight children had the next highest proportion (p < 0.001).

DISCUSSION
The objective of the research was to determine the relationship between health-related physical fitness and physical activity levels, blood pressure, and anthropometric parameters for different weight statuses in Chilean schoolchildren. It was found that physical fitness was inversely associated with SBP and positively associated with PA.
Overweight and obese schoolchildren had higher SBP and DBP than those with normal weight. The results of this study are consistent with those of other studies of children and adolescents in different parts of the world, in which BP presents a positive correlation with BMI and various anthropometric markers 25,26. An important finding is that the group of schoolchildren with obesity contained the highest proportion of individuals with hypertension, which is similar to a finding reported in another study in Chilean schoolchildren 27. These results stress the need for routine measurement of BP in child and adolescent populations because of the silent risks posed by hypertension 14.
In the measurements of physical fitness, boys obtained better results than girls for VO2max, handgrip strength and SLJ. Similar results were found in samples of Spanish schoolchildren 28 and Colombian schoolchildren 29, with boys showing a better performance in the same study variables. In the comparison by weight status, schoolchildren of normal weight presented better results for health-related physical fitness than children in the other two groups (overweight and obese). Similar results were reported for a sample of schoolchildren in which obese individuals showed significantly lower levels of physical fitness, in a study that also reported that increased BMI limits the proper development of motor skills 30.
In the present investigation, strength (explosive and handgrip) and CRF were related to a reduction in SBP. An investigation among Spanish schoolchildren has reported that good muscular fitness is associated with lower CMR, but particularly when accompanied by normal weight 31. Similar results were reported in an investigation in which increased CRF was associated with a reduction in cardiometabolic risk among obese children 32. Moreover, in a systematic review, higher levels of muscular strength in the upper and lower parts of the body were associated with a lower risk of mortality in the adult population, independently of age and follow-up period 33.
Schoolchildren with obesity demonstrated lower levels of PA, and this is the same in several countries in which it has been found that a lack of PA increases the individual risk factors for becoming overweight or obese 34. In one investigation, obese children and adolescents had low levels of physical activity, and the vast majority were not meeting national recommendations for PA 35; also, lower physical activity has been shown to lead to increased adiposity 36. Lack of PA is a very important behavioral risk factor, and works together with other factors associated with a sedentary lifestyle (lack of sleep and hours spent watching television) 37. An investigation has reported that there is a greater risk of hypertension in people with low levels of PA who are also overweight or obese 27; furthermore, these factors also increase the risk of developing diabetes, with higher levels of insulin in circulation 38. Overweight and obese children need support and encouragement to exercise, and physical education (PE) classes in school represent a major opportunity for stimulating the enjoyment of PA 39. The main elements of positive interventions in PE classes included training staff (PE specialists and/or classroom teachers), changes in PE curricula, provision of equipment and materials, and adjustment of the interventions to target specific populations 40. Some studies have shown that schools have made progress in improving school-provided food and physical activity environments, but that much more work is needed 41.
For this reason, increasing PA among children is a priority; however, interventions to this end must stress the support of the parents and their ability to promote PA in their children, providing positive feedback, serving as active models and facilitating participation in PA programs. Therefore, the best space for carrying out interventions is at school. This suggests continuing support for PE classes worldwide.
LIMITATIONS
One limitation of the study was the lack of direct assessments of PA among the obese children and the other study groups, since perceptions of practice may be altered by emotional factors. Future studies should incorporate biomarkers which can show stronger relationships between health-related physical condition and cardiovascular risk in obese children.
CONCLUSIONS
In conclusion, the results obtained in this study are that physical fitness has an inverse relationship with SBP and a positive relationship with PA levels. Moreover, CRF and the long jump test were inversely associated with the predictors of risk factors for cardiovascular diseases. Finally, obese children presented lower physical fitness, and a higher proportion of them had hypertension. For this reason, these results stress the need for routine measurement of physical fitness and BP in child and adolescent populations, because of the silent risks posed by hypertension, as well as the need to improve and increase PA in schoolchildren.

