










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Nutritional monitoring of children and adolescents has the early diagnosis of developmental disorders as a priority, as well as maintaining a proper immune response and quality of life during treatment 1,2.
Patients undergoing chemotherapy and/or radiotherapy, as in the case of hematopoietic stem cell transplantation (HSCT), may have protein-energy malnutrition (PEM), whether by the primary disease or by the signs and symptoms that are secondary to the procedure, such as loss of appetite, nausea, vomiting, mucositis and diarrhea 3.
PEM may determine morphological and functional changes in pulmonary (atelectasis), liver (atrophy of hepatocytes, steatosis) and gastrointestinal (malabsorption, achlorhydria, bacterial translocation) systems and contribute to a longer hospital stay, reducing quality of life and increasing the cost of treatment 4. Studies have shown that PEM is a negative prognostic factor, being associated with low survival in patients with metastatic diseases and acute myeloid leukemia 5.
HSCT is a therapeutic procedure based on the infusion of hematopoietic progenitor cells after high doses of chemotherapy and/or radiotherapy (conditioning) in order to restore the individual's bone marrow function 6. There are three types of HSCT: a) autologous, where the patient receives the hematopoietic stem cells from their own bone marrow; b) syngeneic, when the donation is performed between identical twins; and c) allogeneic, when the procedure is performed from cells of another donor who is related or unrelated 7.
The allogeneic HSCT is indicated for the treatment of neoplastic (leukemia and myelodysplastic syndrome) and non-neoplastic (immunodeficiencies, thalassemia major, osteopetrosis, adrenoleukodystrophy, Fanconi anemia and severe aplastic anemia) diseases 9. Leukemia is the leading global indication for allogeneic HSCT (71% of cases) 8.
The procedure can be divided into the stages of conditioning, infusion of progenitor hematopoietic stem cells and immunological reconstitution. Conditioning is the initial phase. Its purpose is immunosuppression and creating room in the bone marrow stroma for the hematopoietic stem cells, which shall be infused, to have room to proliferate and differentiate, reconstituting normal hematopoiesis and eradicating the disease. In some cases, high-dose chemotherapy may be combined with total body irradiation (TBI) to induce greater immunosuppression 10. The infusion is the transfusion of hematopoietic stem cells from the donor to the receiver. Immunological reconstitution is based on the restoration of the receiver's normal hematopoiesis 11.
HSCT conditioning regimen, total body irradiation (TBI) and the presence of graft-versus-host disease (GVHD) in the gastrointestinal tract may determine signs and symptoms that progressively impair the patient's nutritional status (NS). Among them, it is possible to mention oropharyngeal mucositis, esophagitis, taste alteration, xerostomia, anorexia, nausea, vomiting and diarrhea. These complications may persist for weeks or even months, implying a negative effect on intake, absorption and loss of macro and micronutrients 12. The resulting malnutrition is related to these patients' increased morbidity and mortality 13,14.
Few studies in the literature describe the most relevant aspects related to the evolution of NS during hospitalization of children and adolescents undergoing allogeneic HSCT. Because of this, this study has its importance since it can demonstrate the nutritional aspects that influence the nutritional status of children and adolescents undergoing this treatment.
METHODS
A retrospective cohort study was carried out including 63 patients, between zero and 19 years of age (incomplete), who have undergone an allogeneic HSCT at a university hospital in the Brazilian city of Porto Alegre, from January 2009 to December 2014. Data were collected by the researcher herself from consulting electronic medical records. A patient who performed two transplants at the same hospitalization was excluded from the research.
Clinical data were collected related to the original illness, conditioning, and length of stay (LOS), time for getting the bone marrow, the presence of GVHD, infection and signs and symptoms from the gastrointestinal tract. Regarding the nutritional aspects, data were collected on nutritional evaluations performed during hospitalization, adequacy of caloric intake, verified through intake controls, as well as the nutritional therapies used (enteral, parenteral and/or oral), which were described. These variables were analyzed at the time of admission, at time D0 (day of cell infusion), D+7, D+14, D+21 and D+28.
For the diagnosis of NS, weight and height were used plus computer software WHO Anthro 15 and WHO Anthro Plus 16), versions 3.2.2. Body mass index/age (BMI/A) z-scores were calculated. Values between -1 and +1 were indicative of eutrophy, values between -2 and -1 diagnosed nutritional risk and values below -2 indicated standard deviations, undernourished. For the diagnostic of overweight, values between +1 and +2 were used and for obesity z-score values greater than +2 were used 17.
The outcomes analyzed were: NS related to the time to get it, length of stay and number of infections.
Data were entered in a Microsoft Excel spreadsheet and then exported to the SPSS v. 18.0 program for statistical analysis. Categorical variables were described by frequencies and percentages. Quantitative variables with symmetric distribution were described by the mean and standard deviation and the ones with asymmetric distribution, by the median and interquartile range. Quantitative variables were compared between two categories of factors by the Student's t-test for independent samples and among three or more by the analysis of variance (ANOVA) test. A 5% significance level was considered for comparisons established.
The study was approved by the scientific committee and the research and ethics committee on health of the HCPA, under protocol number 993,062, dated March 18, 2015.
RESULTS
Sixty-three patients were evaluated, being 56% males. The median age was ten years 5,6,7,8,9,10,11,12,13,14,15,16. Table 1 shows the population's characteristics in relation to diagnosis, type of transplant, conditioning and NS classification at hospitalization.
Table I Features of the population of the study

HSCT: hematopoietic stem cell transplantation; BuCy: busulfan + cyclophosphamide; ATG: anti-thymocyte globulin (thymoglobulin); Cy: cyclophosphamide; TBI: total body irradiation. *Data were expressed as absolute frequency (N) and relative frequency.
During the study period, 19 types of conditioning protocols were used. Of these, 64% were high intensive regimen and 36% were low intensive regimen. The four most applied (59% of cases) were: BuCy (busulfan + cyclophosphamide) with and without ATG (anti-thymocyte globulin) (thymoglobulin), as well as CyTBI (cyclophosphamide + total body irradiation), also with and without ATG.
The average length of stay was 58 days (± 25 days), with no variation among the different nutritional diagnoses (p = 0.275). The time to handle bone marrow was 20 days (± 6 days), with no difference among the four types of transplantation performed (p = 0.126) or even among the different nutritional diagnoses at hospitalization (p = 0.352). Ten patients (16%) died during hospitalization. Of these, six (60%) underwent transplantation of the unrelated donor type.
Average weight loss during hospital stay was 1.8% (± 5.8) (p = 0.001). The weight loss median of patients who died during hospitalization was 3.7% (2.0-5.6), in a maximum period of 28 days (D0-D28). When analyzing the presence of signs and symptoms during hospitalization, regardless of the time, 98% of patients had poor appetite, 67% had nausea and 83% had mucositis (50% grade 3 and grade 4). Odynophagia was present in 57% of patients, vomiting in 44%, and diarrhea in 43%. Figure 1 shows the prevalence of signs and symptoms at different times analyzed.

The association was positive when analyzed the regimen intensity (mieloablative) with mucositis (RR = 1.51 [1.10-2.08]) as well as with the use of parenteral nutrition (RR = 2.49 [1.17-5.13]).
In relation to diet administration routes, seven patients (11%) used enteral nutrition (EN) and 31 patients (49%) used parenteral nutrition (PN), simultaneously or not with oral administration (OA). The average duration of PN was 20 days (± 9 days). Figure 2 shows the prevalence of the use of different routes of nutritional therapy (NT) during hospitalization. On D+7, 40% of patients were having PN and on D+14 the prevalence was 45%. OA intake was kept on D+7, D+14 and D+21 by about 68% of patients, regardles s of the total energy value (TEV) reached. Although less frequent, EN was more used on D+14 (8%) and D+21 (11%).

Figure 2 Use of different routes of nutritional therapy during hospitalization (OA: oral administration; EN: enteral nutrition; PN: parenteral nutrition).
Figure 3 shows the TEV achieved according to the combination of NT used throughout hospitalization. A minimum food intake between 31 and 36% of energy needs was observed on D0 in the three groups analyzed (OA exclusive, OA + PN and OA + EN).
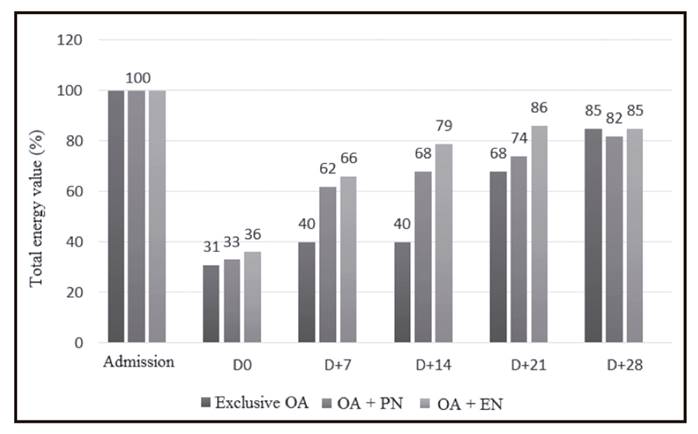
Figure 3 Total energy value (TEV) reached according to the set of nutritional therapies used (OA: oral administration; EN: enteral nutrition; PN: parenteral nutrition).
On D+7, patients with OA exclusive still kept a low caloric intake (40%), remaining so until D+14. As for patients with PN or EN associated, they were able to achieve a greater intake than 60% of their needs. From D+21 there was an increase in caloric intake by OA in the three groups analyzed, reaching a TEV of 68% in OA exclusive, 74% in OA; PN and 86% in OA + EN. The combination OA + EN enabled those patients who had the possibility of using this route a higher calorie intake at all times of hospitalization.
When analyzing the presence of GVHD, 21 patients (33%) presented the disease in any organ. Skin GVHD was diagnosed in 52% of these patients, as well as GVHD of the gastrointestinal tract. Liver GVHD was diagnosed in 57% of these patients. Twenty-four percent had GVHD in the three organs mentioned above.
Regarding infections, 89% of patients had at least one type during hospitalization. The most frequent infections were febrile neutropenia (52.6%), septicemias by coagulase-negative Staphylococci (14%) or Escherichia coli (7%) and typhlitis (7%).
DISCUSSION
This study describes general aspects that during hospitalization can interfere with NE and NT used in children and adolescents undergoing allogeneic HSCT.
A study carried out by Ferreira et al. 18 has analyzed 64 adult HSCT patients and described a handling time (18 days) similar to the one in the present study (20 days). During hospitalization, they had a similar prevalence of death (17.2%). Hospitalization time in the study by Ferreira et al. was lower (36 days), as well as in the study by Sommacal et al. 19 (39 days), when compared to the present study, whose study group was of children and adolescents (58 days).
Hadjibabaie et al. 20 have included 50 adult patients undergoing allogeneic and autologous transplantations in their study and showed a significant difference for handling of three days for eutrophic ones and four days for patients with overweight/obesity when compared to malnourished patients.
It was possible to identify a loss of 1.8% of the weight between hospitalization and on D+28. Weight loss was not enough to change the nutritional diagnosis, but by itself, this weight loss already provides a high nutritional risk due to the patients' ages. The loss percentage was shown to be the most sensitive method in the study by Sommacal et al. 19, which weekly compared methods available for nutritional assessment between D-7 and D+28 in 17 adult patients undergoing the same treatment. It is important to note that the patient may have changed their weight during hospitalization due to overhydration (treatment protocol) and also by the volume infused by PN 21.
In a study carried out with 89 pediatric patients who had undergone both allogeneic as autologous HSCT, the use of PN by 48% and EN by 35% of patients was described. In this study a larger indication of EN can be identified, probably due to the second type of transplant cited. This behavior may be related to increased gastrointestinal toxicity experienced by patients undergoing allogeneic HSCT. When analyzing only the allogeneic-type HSCT, calorie intake by PN was 54% of energy needs, similar to that found in the present study 22.
Some criteria are used to define the need for PN, such as severe malnutrition at hospital admission, insufficient oral intake (< 60% of nutritional requirements) for a period longer than five days, and/or weight loss greater than 10% during the treatment 23. In this study, patients had insufficient food intake throughout hospitalization and nutritional intervention was necessary, especially with the use of PN.
Thus, in this study, evaluating 63 patients with a median age of ten years, it was observed that at the time of hospitalization, 100% of patients had their energy needs by mouth, decreasing from D0 (about 30%), with more prevalent use of PN and EN from D+7. In addition, from D+21 it was possible to observe an increase in caloric intake by mouth. Mieloablative regimen needed more nutritional therapy intervention when compared to non-mieloablative regimen.
Patients showed decreased food intake throughout hospitalization, but in this hospital it has been already possible to get calorie intake closer to the ideal one with the help of alternative nutritional therapies. Results demonstrate that an appropriate nutritional screening tool considering these aspects could help to intervene earlier maintaining an adequate nutritional status.

