










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
It has been recognized that breastfeeding, initiated within the first hour of birth, given exclusively for six months and continued for two years with the provision of safe and adequate complementary foods, is one of the most powerful practices to promote survival and child welfare 1. Improving breastfeeding rates worldwide could save the lives of more than 820,000 children under the age of five each year, the majority of them (87%) under six months of age. In addition, breastfeeding is also good for mothers. Breastfeeding protects against postpartum hemorrhage, postpartum depression, ovarian and breast cancer, heart disease, and type 2 diabetes. It is estimated that improving breastfeeding rates could prevent 20,000 additional maternal deaths from breast cancer 2,3.
In industrialized countries, the prevalence of breastfeeding is greater than that observed in less industrialized countries, and apparently the best socioeconomic level and education influence these differences 4,5. In Mexico, as in other countries, the prevalence of exclusive breastfeeding in the first half of postnatal life and its continuation up to 24 months is less frequent than expected. This condition is due to multiple factors: demographic, socioeconomic, cultural, occupational, psychological, medical, environment of support, decision or interest of the mother, and so on 6,7,8,9,10,11,12,13.
A less explored factor, at least in recent years, is the influence of the infant's gender on the mother's decision to offer and maintain breastfeeding. There is some evidence of gender discrimination in favor of males since the past century. In the decade of the 1980s and 1990s, several studies were published in favor of and against the potential discrimination by gender of children in different countries 14. In China, discrimination against females after the first child was recognized among the different socioeconomic groups 15. Although studies did not show significant differences in the duration and intensity of breastfeeding in Morocco and Tunisia, there were small differences in favor of Tunisian males with respect to immunization and treatment of diarrhea 16. In rural India, there were significant differences between males and females in terms of the prevalence of malnutrition that pointed to discrimination against females, including with respect to exclusive breastfeeding 17.
In our country, the published literature is scarce and less precise, but some studies have shown higher malnutrition in females (39%) than in males (20%), indicated by weight for age 14. In marginalized areas of Guadalajara 18, females aged 12 to 24 months showed a higher rate of malnutrition, with a percentage difference of 7-10 points according to the indicator weight for age or weight for height, than males. This apparent discrimination against preschool females was more marked in the Wirrarika culture, an indigenous population of the state of Jalisco 14.
At present we have found some evidence (unpublished data) that mothers prolong breastfeeding longer for males than for females and, consequently, the start of substitutes for human milk is more delayed for males. Therefore, the purpose of this report is to show some evidence that the cultural habit of exclusive breastfeeding is more common for males of mother and infant dyads belonging to a population of medium-low and low socioeconomic strata who were attended since birth in the Nuevo Hospital Civil de Guadalajara.
METHODS
DESIGN
This was a cross-sectional analysis of a sample of 170 mother-infant dyads according to type of feeding: 74 full breastfeeding (FBF), 57 partial breastfeeding (PBF) and 39 human milk substitutes (HMS). This sample was obtained from a non-random cohort study. The sampling method was non-probabilistic at the site of birth concentration. We identified 815 mother-newborn dyads who were admitted to the physiological puerperium ward in a shared room at the Nuevo Hospital Civil de Guadalajara. They were included and followed for four months if they met the inclusion criteria: healthy postpartum women living in the metropolitan area of Guadalajara who had signed the informed consent sheet, and with a full-term healthy single infant of either sex, with an adequate weight for gestational age. Dyads were not included when mothers had a history of chronic, genetic, or congenital diseases; addiction to alcohol, tobacco, or drugs; or if the newborns had congenital malformations and/or genetic diseases. Dyads were also excluded for maternal causes such as loss of follow-up, presence of subacute or chronic disease, occurrence of illness or serious accident, and/or infant causes such as subacute or chronic disease, occurrence of an accident or serious illness, or incomplete data about the mother or infant. Four hundred eight dyads were contacted by telephone at the fourth week of postnatal life; 219 dyads accepted and attended the first visit at the eighth week, and 170 dyads attended at the end of the 16th week of postnatal life. There were no significant differences in the general characteristics of the mother-infant dyads between study participants and mothers who were not located by telephone at four weeks or those who declined to participate in the study at eight weeks after postpartum. A total sample size of 148 dyads was estimated with an alpha of 0.05 and a power of 0.80. The proportion of breastfeeding comes from the ENSANUT (2012) for exclusive breastfeeding (14.4%) and for predominant breastfeeding (25%) 19.
The dependent variables were type of feeding: full breastfeeding, exclusive and/or predominant 1; partial breastfeeding; and human milk substitutes.
The independent variables were demographic data: age of parents; number of family members and type of family, that is, nuclear (only parents and children), extended (parents, children and grandparents) or composed (parents, children, grandparents and other blood relatives and non-consanguineous); marital status (civil and religious marriage, religious marriage, civil marriage, free union, separated or single mother); schooling (null, equal to or less than three years of primary school, more than three and less than six years of primary school, complete primary, junior high school incomplete, junior and technical high school, senior high school, senior and technical high school, bachelor's degree, specialty; and occupation of mothers and/or parents (employee, bricklayer, laborer, driver, mechanic, tradesman, established trader, professional, student, unemployed, home, domestic employee, other).
FIELD WORK CRITERIA AND STRATEGIES
The study began in the physiological puerperium ward of the Gynecology and Obstetrics Division of the Hospital Civil de Guadalajara. Mothers were invited to participate after researchers (E.G.M., N.M.E.) promoted the practice of at least six months of full breastfeeding. We clarified that we were interested in including all the mothers who wanted to participate regardless of the mode of feeding that they chose for their infants. After the mothers signed the informed consent form, we began collecting demographic, socioeconomic, and educational dietary variables; the mothers were then contacted after a period of one month to describe the type of feeding they had chosen for their infants. Those who agreed to participate had scheduled appointments at 16 weeks postpartum.
COLLECTION OF INFORMATION, DATABASES, AND COMPUTER PROGRAMS
Information on general, demographic, socioeconomic and educational level was captured on collection sheets specifically designed for the protocol. After the information was obtained, the database was elaborated and captured, and the statistical analysis was performed with SPSS version 24 software.
STATISTICAL ANALYSIS
Levene's test was used to assess equality of variances for two or more groups, and Shapiro-Wilk and Kolmogorov-Smirnov tests were used for exploring the normality of distributions. The Kruskal-Wallis test was used to identify significant associations between variables of various proportions. In variables with non-normal distribution, the Mann-Whitney U test on samples was used. We also used the Chi-square test and odds ratio (95% confidence interval) to estimate the associations and the epidemiological significance of the data.
ETHICAL CONSIDERATIONS
The recommendations of the Declaration of Helsinki were followed in its last amendment during the 64th Annual Assembly organized by the World Medical Association, 2013. The protocol was applied to each of the participating dyads that met the inclusion criteria after the mother gave her authorization by signing the informed consent. The protocol was approved by the Committees of Bioethics and Research of the Hospital Civil de Guadalajara (CI-01314).
RESULTS
The total sample comprised 170 dyads, 70 females (41.2%) and 100 males (58.8%). Of the total sample, 74 (43.5%) received FBF, 57 PBF (33.5%) and 39 (22.9%) HMS. Of the total group of females, 22 (31.4%) received FBF, 24 (34.2%) PBF and 22 (34.2%) HMS; of the total group of males 52 (52%) received FBF, 33 (33%) PBF and 15 (15%) HMS. Table 1 shows that in females the age of the parents, number of members in the family and economic characteristics were similar in the three types of feeding, and there were no significant differences. Table 2 shows that in males, the expenditure on food (p = 0.020) and per capita food expenditure as a percentage of the minimum wage (p = 0.026) was significantly higher in the group of PBF than in the FBF and the HMS. Specifically, the monthly expenditure on food was higher in PBF vs FBF (p = 0.035) and in PBF vs HMS (p = 0.011); per capita food expenditure (percentage of minimum salary) was higher in PBF than in FBF (p = 0.050) and in PBF vs HMS (p = 0.010). The amount in Mexican pesos for feeding per capita was higher in PBF than in FBF (p = 0.050) and in PBF vs HMS (p = 0.010). These data presuppose greater purchasing power of income distribution in mothers who give PBF.
Table I. General characteristics of the parents of females at four months according to the type of feeding (n = 170)
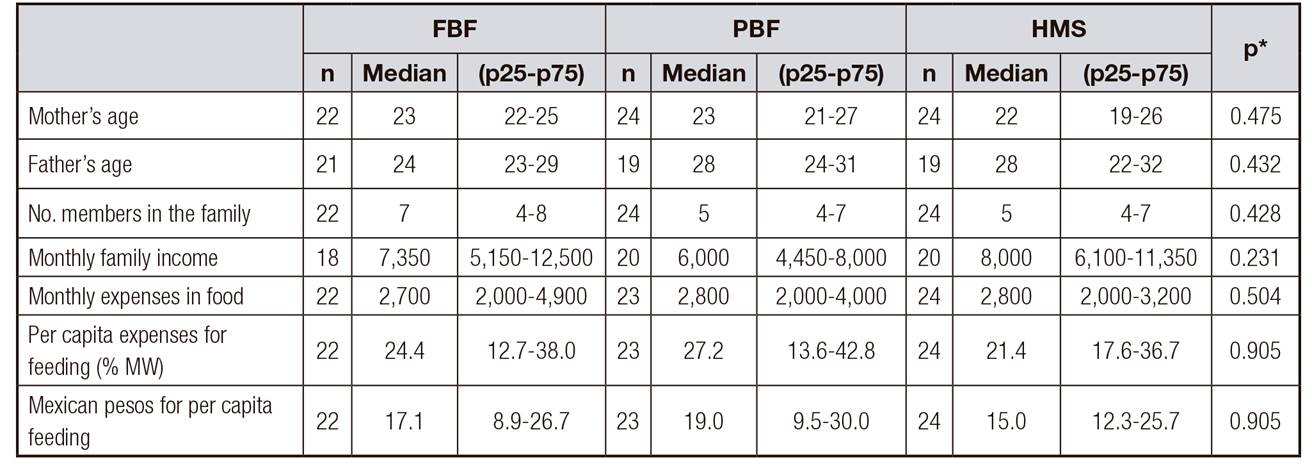
FBF: full breastfeeding; PBF: partial breastfeeding; HMS: human milk substitutes.
*Kruskal-Wallis test.
%MS: percentage of minimum wage. Rate Mexican peso:dollar was 18.4:1 (2016).
Table II. General characteristics of the parents of males at four months according to the type of feeding (n = 100)
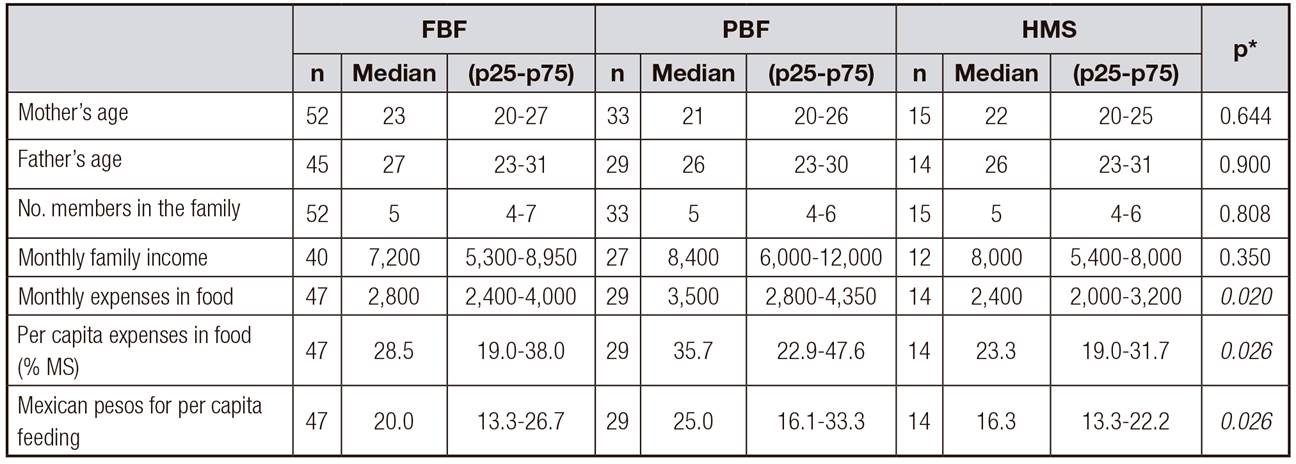
FBF: full breastfeeding; PBF: partial breastfeeding; HMS: human milk substitutes.
*Kruskal-Wallis test.
%MS: percentage of minimum salary. Post-hoc test (Mann-Whitney U). The monthly expenditure on food was higher in PBF vs FBF, p = 0.035; PBF vs HMS, p = 0.011. Spending in food per capita (% MS) was higher in PBF vs FBF, p = 0.050; and PBF vs HMS, p = 0.010. The amount in Mexican pesos for feeding per capita was higher in PBF vs FBF, p = 0.050, and PBF vs HMS, p = 0.010.
Table 3 shows that, in general, there were no significant differences between the three types of feeding regarding the family composition in the groups of females and males. In a particular way, it was observed that in the group of females, the frequency of extended families was higher for females who received FBF (55%) than in those who received PBF (25%) or a HMS (29%) (p = 0.10). Although this association was not significant, it is likely that a type II error was made considering the small number of cases in some cells.
Table III. Family composition of lactating mothers of females and males according to the type of feeding at four months (n = 170)*
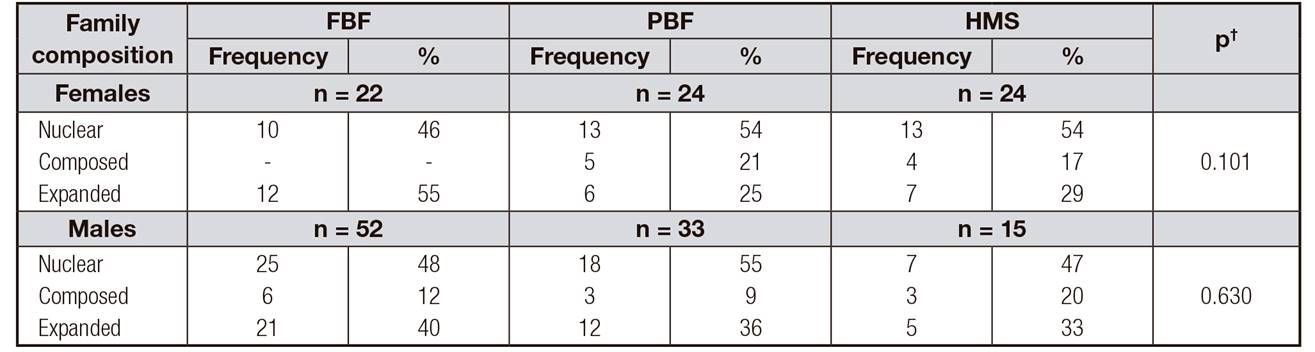
FBF: full breast feeding; PBF: partial breastfeeding; HMS: human milk substitutes.
*Chi-square test.
†FBF vs others (PBF and HMS) when the family composition was non-nuclear (composed and expanded) vs nuclear.
There was no association between the three types of feeding in relation to the marital status of the parents in the groups of females and males. The great majority of the marital status of the parents, when both genders (male and female) were linked for each type of feeding, was in free union in FBF (65%), in PBF (52.5%) and in HMS (62.5%). This would mean that the marital status of the parents is not associated with the type of feeding. It was also observed that in the three types of feeding, those married by civil and/or religious laws were less frequent than other civil status. Likewise, when we combined the percentages of the three types of feeding, a significant frequency (15.7%) of the mothers were single (Table 4).
Table IV. Marital status of the parents according to the type of feeding of females and males at four months (n = 170)*
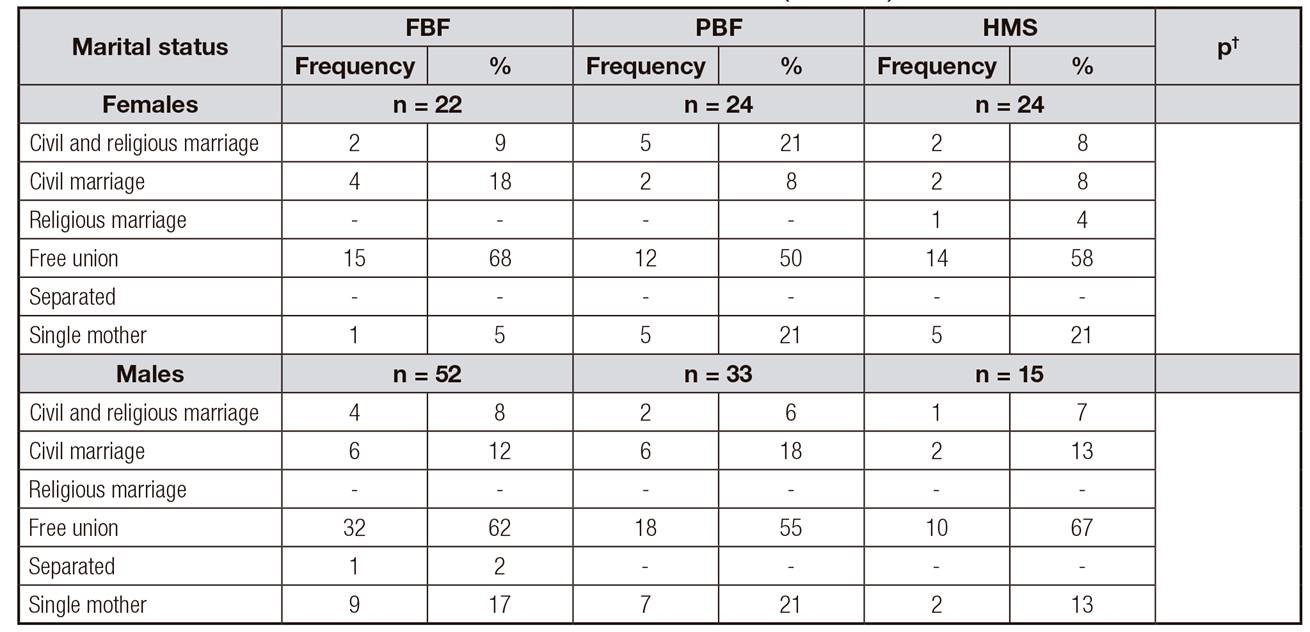
FBF: full breast feeding; PBF: partial breastfeeding; HMS: human milk substitutes.
*Chi-square test.
†FBF vs others (PBF and HMS), when the marital status was free union vs marriages.
Regarding the schooling of mothers and fathers in the group of girls, it was observed that the frequency of FBF vs PBF and HMS was higher when schooling was the same or lower than incomplete junior high school, although the association was not significant (p = 0.079 and p = 0.134, respectively). In the group of males, the schooling of mothers and fathers did not show any association tendency (p = 0.804 and p = 0.449, respectively).
In the group of females, the mothers' occupation was not associated with the type of feeding either, although the household occupation was lower in infants who received PBF (71%) than in infants who received FBF (82%) or HMS (83%). On the contrary, in the group of males, the household occupation was higher in FBF (83%) than in PFB (66%). This association was not significant due to a type II error, considering the small number of cases per cell in the contingency table. The occupation of the father did not influence the type of feeding in the group of females (p = 0.857). In the group of males, when the father was in a stable employment situation, the frequency of FBF was higher (46%) than when the father had a less stable occupation (27%). This included less paid or more remunerated occupations even if they were less stable.
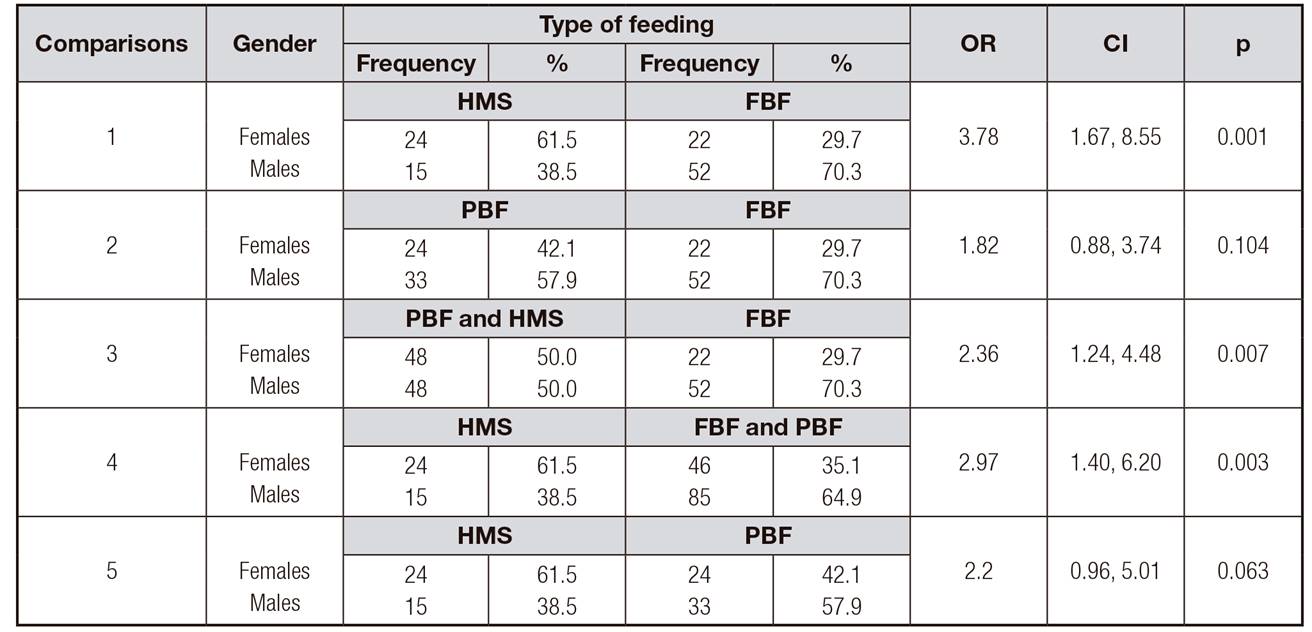
Table 5 shows that the odds of FBF were 3.8 times lower for females than for males. The likelihood of FBF would be less frequent than PFB for females, though in a non-significant way, whereas the likelihood of FBF would be lower than the combination of PBF and HMS for females. Likewise, the likelihood of FBF and PBF would be lower than HMS for females; even the probability of PBF would be lower than HMS, although it did not reach a significant association, probably due to the diversity in the frequency (percentage during the day) of nursing times in PBF.
DISCUSSION
During the process of identification and invitation of mother-newborn dyads in rooming in (allowing mothers and infants to remain together 24 hours a day), exclusive breastfeeding was promoted to all mothers attending the physiological puerperium area. For this purpose, a brief talk was given on the multiple benefits of breastfeeding for the infant and the mother. In addition to the talk, two leaflets were provided with information on breastfeeding and tips for successful breastfeeding. Therefore, all mothers participating in the study knew the importance of offering the breast exclusively. In this way, the contacted mothers were able to decide freely which feeding option was most suitable for them and their infants.
Our study showed that the probability of receiving FBF was about four times lower in females than in males. Even the likelihood of FBF and PBF vs HMS was significantly lower in females than in males. These results undoubtedly reflect that in this population of low and medium-low socioeconomic strata of the metropolitan area of Guadalajara, full breastfeeding is privileged in males over females.
We do not have a clear explanation for this finding, considering that it is a mestizo population that lives in a metropolitan area, the second largest in the country. Pérez Gil-Romo and Díez-Urdanivia 20 have pointed out that in Mexico, gender has been scarcely incorporated as a category of analysis in nutrition and food research. However, a study conducted by this research group on indigenous women of the Sierra Juárez, in the state of Oaxaca 21, included interviews related to the practice of breastfeeding. The first thing they observed was that breastfeeding continued longer in male infants. One of the aspects that drew attention was the meaning of strength of human milk for these indigenous women: "males need to take more time from their mothers to have more strength and thus be healthier to work in the field and keep his family", unlike the females who stay at home helping their mothers with the housework.
In other words, human milk substitutes and domestic work have lower value than male labor. Therefore, it is possible that this cultural trait observed in Mexican women is more ingrained than it seems, and not only in the indigenous population. Therefore, we consider that this privilege granted mainly to males in the metropolitan area of Guadalajara has deep ancestral roots as those observed in the indigenous population of the Oaxaca study. Of course, these are different populations, with different socioeconomic and cultural contexts, but in the background, exclusive breastfeeding is favored for males for the same reasons that were pointed out by the women of the Oaxaca population. In addition, they are mothers of low and medium-low socioeconomic strata that would not necessarily be applicable to the privileged economic strata of the same metropolitan area of Guadalajara and to our country.
Another potential implication of these findings is that, in the same way that there is a metabolic programming of the human being from pregnancy and the first semester of life related to nutrition and other factors, it could be possible that some mestizo families had a behavioral programming of the mother privileging the feeding of the male. That behavior would be defined from the first semester of the postnatal life and continue during the first stages of life, a period in which the feeding habits are defined.
This distinction in privilege of exclusive breastfeeding would have some effects. For example, a study by Pivik et al. 22 showed that in the analysis of syllable processing, there was greater discrimination of syllables in breastfed infants than in infants fed formula. However, they recognized that it cannot be determined to what extent this difference reflects the dietary influences, the feeding method, or the interactions between the influences of the diet and the differences of background factors between breastfed and formula-fed infants. Also, the important findings of Victora et al. 2 suggest that breastfeeding improves intelligence up to adulthood, and that it has an effect at both the individual and societal level, by increasing educational attainment and earning ability. In addition, there are other important benefits such as the consolidation of the human microbiome in those who receive exclusive breastfeeding, are born via vaginal delivery 23 and receive other short- and long-term health benefits 24,25.
Another interesting finding of our study was that monthly per capita food expenditure was significantly higher for males in the PBF group vs FBF and HMS than for girls. Family income was also higher in PBF than in FBF and HMS, although the differences were not significant. These data imply greater interest in food expenditure by the PBF group, greater purchasing capacity, and probably greater awareness of maintaining breastfeeding for males than for females.
LIMITATIONS
The size of the population sample circumscribed to a group of mothers whose children were born in a public hospital in a population of low and medium-low socioeconomic status. This fact does not allow making inferences to populations of other strata of the metropolitan area of Guadalajara and other Mexico states. The main strength is that it is a cohort of mother-newborn dyads, obtained from birth and followed for four months, in which the mothers themselves decided to feed their infants with FBF, PBF or HMS.
CONCLUSION
There is a differentiated character in the privilege of exclusive breastfeeding being four times higher for males than for females in a public hospital in the metropolitan area of Guadalajara. Therefore, this potential discrimination by gender in favor of males would have disadvantageous implications in the short and long term for the health of females who do not receive the privilege of full breastfeeding, and that should be considered by health professionals and the society. It is necessary to expand the size of the sample in different socioeconomic strata to identify whether this specific practice of preferential FBF privilege for males and other feeding variables for females is repeated throughout the metropolitan area of Guadalajara and the country. In addition, it is likely that another methodology, probably qualitative, will be required to deepen the knowledge of the origin and roots of this behavior.

