










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Parenteral nutrition (PN) provides macronutrients (carbohydrates, amino acids and lipids) and micronutrients (electrolytes, trace elements and vitamins) intravenously to patients who cannot be fed through the digestive tract. Due to the fact that PN contains a high number of different chemical compounds, there is the possibility of destabilization, degradation or chemical interactions that may lead to iatrogenesis.
It is common for intravenous solutions to contain particles in suspension and their infusion does not produce immediate serious symptoms in most cases 1. However, its long-term infusion has been linked to increased risk of phlebitis 2, and capillary lesions have been found in necropsies that could be the cause of pulmonary hypertension 3. Recently, several studies 4,5,6 have shown a decrease in serious complications in critical pediatric patients with the use of filters for the retention of particles, supporting the hypothesis of the harmful effect of infusion.
In PN there may be particles coming from the solutions used in the PN's compounding process or formed later, during storage or administration. Therefore, it is recommended to administer the PN with a 0.2 μm filter if it does not contain lipids or 1.2 μm if it does. In addition, the use of filters has been associated with a lower incidence of phlebitis and longer life of the peripheral route.
Due to the great variability in the composition of the PN formulae, before preparation, the pharmacist validates that the concentration of the different products is within safety margins. In Spain, some years ago, a consensus document was drawn up with the aim of facilitating this validation work 7. During the infusion of parenteral nutrition without lipids in an adult patient in our hospital, the appearance of a black precipitate in the filter was observed. This nutrition had been validated by a pharmacist and met the recommendations of the consensus document. There are recent studies that also describe the retention of black precipitates in administration filters 8,9,10,11,12. The studies identified a compound with a high copper and sulfur content, probably due to the interaction of copper with sulfur-rich amino acids. Due to the few studies of this type on precipitation at the time of preparing the document, it is not usual to contemplate this possibility in the validation of parenteral nutrition.
In a previous study we observed a decrease in copper and cysteine concentrations in the PN after its filtration 13.
The objective of our study was to identify the composition of the precipitate found and to determine if by changing the order of addition of the components the formation of precipitate varied.
MATERIALS AND METHODS
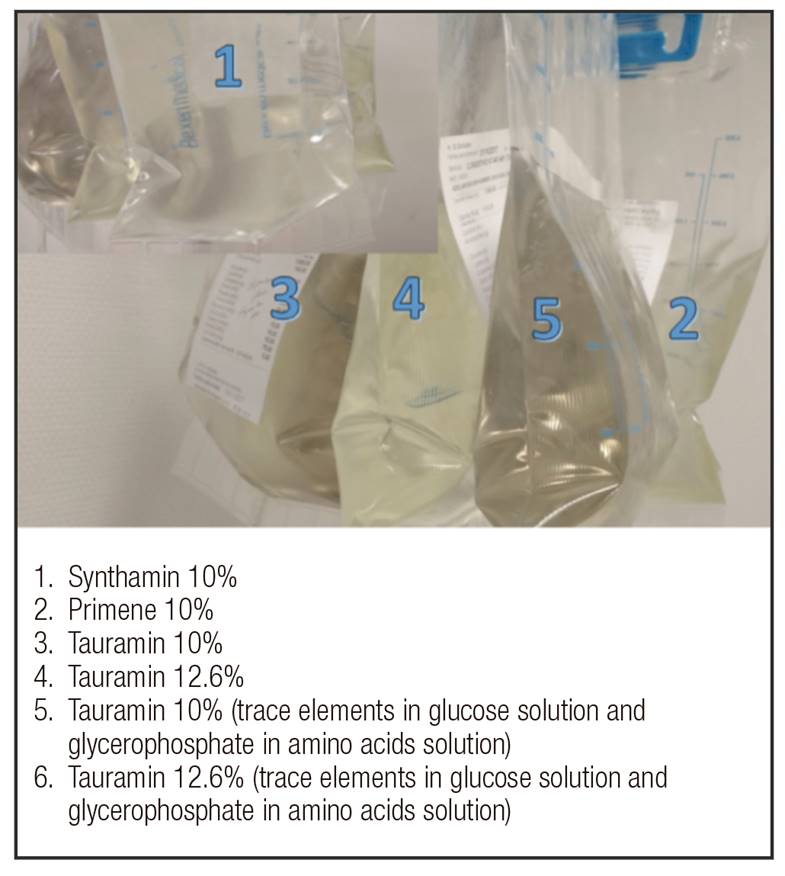
Four PN bags were prepared with the following composition: 1,000 ml of amino acids solution, 150 g glucose, 60 mEq potassium, 217 mEq chloride, 105 mEq sodium, 15 mEq magnesium, 15 mEq calcium, 18.63 mmol phosphorus and trace elements (Addamel®). Each bag was prepared using a different type of amino acids solution: Primene® 10%, Tauramin® 10%, Tauramin® 12.6% and Synthamin® 10%. Table I lists the components and quantities used in the preparation of the PN. The amounts per litre of the different types of amino acids in the solutions and the type of containers can be seen in Table II. The trace element solution used was Addamel®, whose composition can be seen in Table III.



The order of addition used was: amino acid solution, glucose, electrolyte solution, trace elements and sodium glycerophosphate.
Two more bags with the same composition were made, one with Tauramin® 10%, and another with Tauramin® 12.6%. However, the order of addition in the preparation was altered, so that instead of adding trace elements and sodium glycerophosphate at the end, the trace elements were added to the glucose and the glycerophosphate to the amino acid solution.
All the solutions were filtered with Pall NEO96E® filters (Pall Corporation) of 0.2 μm immediately after the preparation and were observed during the infusion to detect color changes. Subsequently, these filters were transported to Pall Corporation for further analysis.
Filter membrane preparation for analysis was by the introduction of air into the Pall NEO96® filter inlet connector using a 20 ml syringe to remove any liquid residue from the membrane. The filters were then opened and a 1 cm2 filter section was removed. The samples were mounted for analysis by scanning electron microscopy (SEM) with the membrane oriented upstream side uppermost. The samples were dried in a desiccator before SEM analysis.
The filter samples were examined using a computer-aided scanning electron microscope (SEM Hitachi TM300) and equipped with an X-ray scattering spectrometry system (Quantax 70). The samples were coated with gold before analysis by SEM and EDS. A thin gold coating was deposited on the surface of each sample using a vacuum coating system (Gold Agar Sputter Coater), to increase the conductivity of the samples. All the samples were initially analyzed at the point with coordinates 0.0 to 100x magnification through SEM. The images obtained by SEM were also analyzed at 500x and 1,000x in the 0.0 field of view with an acceleration voltage of 15 kV. The analysis by EDS was carried out at 1,000x magnification.
RESULTS
Immediately after the PN preparation, a darkening of the solution in the bags was observed, and this became more pronounced with time (Fig. 1).
The images at 1,000x magnification (Fig. 2) show a large amount of precipitate in PNs with amino acids that contained cysteine and that were packed in glass. The precipitates appeared compacted in the filter. In the Primene® 10% and Tauramin® 10% filters, a greater amount of precipitate was observed than with Tauramin® 12.6% and Synthamin® 10%. The EDS analysis showed that the percentage of copper and sulphur in each area of the filter studied was much higher in the solutions with Tauramin® 10% or with Primene® 10%, than in the rest (Table IV).
There were no differences in the percentages obtained by the order of addition.


DISCUSSION
All the filters where the black precipitate was observed contained sulphur and copper, and it seems that this precipitation is produced with solutions of amino acids with cysteine and multi-elements containing copper. However, no correlation was found between the cysteine concentration of the amino acids and the formation of the precipitate. In our study, we found this precipitate with Tauramin® 10%, and not with Tauramin® 12.6%, when the concentration of cysteine is higher in the latter. This could be due to the different type of container. Tauramin® 12.6% is packed in a plastic bag that could be permeable to gases, unlike Tauramin® 10%, which is packed in glass.
Several authors described precipitates similar to those we have found 2,3,4,5,6. In all cases there was a darkening of the filter which alerted about the presence of the precipitate. Most of them used pediatric amino acid solutions, since they contain cysteine, an amino acid considered to be essential in premature babies. In our case, the finding occurred in adult parenteral nutrition, but with a Tauramin® solution, which, unlike other adult solutions, contains cysteine and taurine.
Thibault used Primene® as a source of amino acids, but the precipitate found is different from that observed in the present study. A solid yellow-brown substance in suspension is described in the filter. The concentrations of the PN solutions where these precipitates are found have ranges of 1-4.3 mcg/ml of copper and 2.8-5 mg/ml of cysteine, which are considerably higher than the theoretical ones of our PN solution (0.78 mcg/ml of copper and 0.3 mg/ml of cysteine) 10.
Foinard et al., also with Primene® as a source of amino acids, found black precipitates similar to ours. They studied mixtures of pediatric PNs with concentrations of 1.2-2.68 mcg/ml of copper and 0.77 to 1.72 mg/ml of cysteine and found a decrease in the concentration of cysteine in the filtered solution with respect to the previous one. They described a very pronounced decrease in the concentration of cysteine at time 0 compared to the theoretical value, which is in line with the darkening observed in the bags immediately after preparation. They also studied, as in our case, the filters by SEM and EDS and found particle conglomerates on the surface of the filters that are very similar to those we have found. The EDS analysis identified high concentration of copper and sulphur and low amount of chlorine, phosphorus, calcium, silicon, selenium, magnesium and potassium 12. Our results were very similar. In addition to high percentages of sulphur and copper when the composition of the PN involved Tauramin® 10% or Primene® 10%, in some of the filters we also found chlorine, potassium, silicon or selenium, although in much lower percentages.
Hanff et al. found darkening of filters with concentrations of 0.51-0.72 mcg/ml of copper and 0.53-0.59 mg/ml of cysteine, concentrations more similar to those found in our case. They also used Primene® and observed this precipitation due to the change of trace element solution, from Peditrace® to Addamel® in patients with long-term PN in order to provide iron. Addamel® has much higher amounts of copper. They solved this problem by changing again to Peditrace® or decreasing the amount of Addamel® 11.
The amount of copper provided by an Addamel® ampoule (1.27 g) is much higher than the recommended daily dose (0.3-0.5 mg) 14,15,16,17. More studies are needed with trace elements supplements that are more in line with the recommendations.
It would be necessary to carry out more research to know from what concentrations of copper and cysteine these precipitates are produced and what other variables of the preparation and composition of PN are involved in their formation.
We used filters in the administration of all the PNs and for this reason we have been able to detect the formation of these precipitates. In our case, it was a PN without lipids, so the black precipitate was detected immediately in the filter and a darkening of the solution and black spots in suspension were observed in the bag. In all-in-one PNs, although black dots could be seen in suspension, this precipitation could go unnoticed, and if filters are not used, these precipitates would pass to the patient. We do not know the clinical implications that it may have, but it does not seem advisable to infuse a large quantity of particles into the bloodstream.
In conclusion, the findings found in our composition analysis based on EDS on the filters indicate that sulphur and copper intervene in the composition of the precipitate. These precipitates are produced when amino acid solutions containing cysteine and packed in glass and high concentrations of copper are used. It is important to use filters in the administration of parenteral nutrition to avoid the passage of these precipitates to the patient.

