










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Obesity has become the greatest threat to global public health in the last century, affecting approximately 1.4 billion adults in 2016 1. Certain eating patterns, such as the omission of breakfast, have been associated with being overweight/obese compared with breakfast consumers 2,3. In a U.S. study reported among adults, the daily breakfast eaters gained 1.91 kg less than infrequent breakfast consumers (< 4 days/week) over 18 years 4. There is also literature indicating that skipping breakfast is associated with dyslipidemia, hypertension, higher risk for type 2 diabetes and cardiovascular disease 4,5. Furthermore, skipping breakfast has been associated with a lower level of physical activity 6, and individuals who eat breakfast daily are more likely to participate in strenuous physical activity than those who never eat breakfast 7.
Most of the nutritional studies regarding breakfast consumption and physical activity have been achieved in developed countries, with scarce evidence originating from other regions such as Latin America (LA). Yet, LA is one of the two most obese low-income and middle-income regions globally . In addition, poor diets and inadequate physical activity in the region are causing high levels of diabetes and cardiovascular disease 8,9. Ecuador, has not been the exception to this regional trend. Due to important socioeconomic and demographic changes during recent decades 10, its population has transitioned from having traditional dietary habits to unhealthy food intake and physical inactivity 11,12. Currently, the prevalence of obesity in adults in Ecuador has reached almost one half of the total population 12.
At present, data does not exist on the dietary habits of Ecuadorian residents, especially with regards to their consumption of breakfast. The objectives of this cross-sectional study were to examine whether breakfast skipping is associated with nutritional status and level of physical activity. Furthermore, we examined whether the omission of breakfast presented associations with nutritional data regarding intake of macronutrients, micronutrients, as well as demographical features including sex and geographical region. This study used data from The Latin American Survey of Nutrition and Health (LANHS) to provide population-level data in order to prevent obesity in Ecuador.
MATERIALS AND METHODS
This cross sectional study is based on the data from The Latin American Survey of Nutrition and Health -in Spanish Estudio Latinoamericano de Nutrición y Salud (ELANS)-Ecuador, whose methods have been reported elsewhere 13. In brief, this is a multicenter cross-sectional nutrition and health surveillance study of the nutritional and physical activity status of adolescents and adults in eight Latin American countries. These data were collected over a 1-year period in the following countries: Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru and Venezuela. The current study used data collected in Ecuador from September 2014 to March 2015.
STUDY PARTICIPANTS AND DESIGN
The ELANS used a randomized complex, multistage sampling process, which was stratified by geographical location, gender, age and socioeconomic status in order to select a representative sample of the Ecuadorian population. The sample size was calculated with a confidence interval of 95% and a margin of error of 3.46%. A survey design effect of 1.75 was estimated based on guidance from the U.S. National Center for Health Statistics 14, and calculations of the minimum sample sizes required per strata (i.e. socioeconomic level, age and gender) performed for Ecuador. We analyzed data from 800 adolescent and adult participants from 15 to 65 years of age from nine cities including Guayaquil, Machala, Portoviejo, Manta, Quito, Cuenca, Ambato, Loja and Ibarra, which correspond to the coastal and highland regions of Ecuador (397 males and 403 females). We excluded pregnant and lactating women, individuals with major physical or mental impairments, adolescents without a signed consent form by their parent or legal guardian, individuals living in any residential setting other than a household, and individuals unable to read.
ETHICAL CONSIDERATIONS
The ELANS protocol was approved by the Western Institutional Review Board. In Ecuador, the Institutional Review Board of the Universidad San Francisco de Quito approved the study prior to its implementation. Each individual signed a written consent form prior to their participation in the study. Participant confidentiality was maintained via the use of numeric identification codes and all data transfer was done with a secure filing sharing system.
DATA COLLECTION
The ELANS data was collected via questionnaires administered in two household visits and objective anthropometric measurements. In the first visit, the socioeconomic level questionnaire (established by the Instituto Nacional de Estadística y Censo, Ecuador) and two 24-hour dietary recalls were applied, in non-consecutive days including weekend days, as well as anthropometric measurements taken. In the second visit, which took place 4 to 30 days later, a second 24-hour recall and the International Physical Activity Questionnaire (IPAQ) was administered to each participant. The information that came from the dietary recall questionnaires were transferred into energy, macronutrients, and micronutrient quantities using the Nutrition Data System for Research software, version 2013 (NDS-R, Minnesota University, MN, USA). NDS-R is an accurate nutrient and food group serving calculation software that utilizes the United States Department of Agriculture (USDA) Nutrient Data Laboratory as its primary source of nutrient values and nutrient composition.
PHYSICAL ACTIVITY
Based on the IPAQ questionnaire physical activity was categorized into low, moderate, and high categories. Low physical activity was considered when individuals do not meet criteria for moderate or high categories. Individuals with moderate physical activity where those who satisfied the following criteria: a) 3 or more days of vigorous-intensity activity of at least 20 minutes per day; or b) 5 or more days of moderate-intensity activity and/or walking of at least 30 minutes per day; or c) 5 or more days of any combination of walking, moderate-intensity or vigorous intensity activities achieving a minimum total physical activity of at least 600 MET (Metabolic Task Equivalent of Task)-minutes/week. High physical activity was considered when encompassed the following: a) vigorous-intensity activity on at least 3 days achieving a minimum total physical activity of at least 1500 MET-minutes/week; or b) 7 or more days of any combination of walking, moderate-intensity or vigorous-intensity activities achieving a minimum total physical activity of at least 3000 MET-minutes/week.
DIETARY ASSESSMENT
A single 24-hour dietary reminder is limited and usually inadequate to evaluate diet, two recalls were chosen to estimate routine food intake and to assess intraindividual variability in nutrient intake as literature shows 15. Thus dietary data were collected based on the Multiple Pass Method using two non-consecutive 24-hour dietary recalls within one week 16. The 24-hour recalls were used to divide the participants in three groups according to their morning meal behaviors: a) breakfast skippers in any one recall; b) breakfast skippers in two recalls; and c) breakfast eaters in both recalls. Breakfast was defined as a consumption of > 100 kilocalories consumed from 4 to 10 am. The 24-hour recall questionnaires were also used to describe the total energy intake of the participants, and micronutrients including calcium, total sugar and fiber.
NUTRITIONAL STATUS
The nutritional status of the participants was monitored by analyzing body weight and height, in order to calculate body mass index (BMI). BMI was categorized according to the definitions established by the World Health Organization, which divides them in underweight, normal weight, overweight and obesity 17. In order to produce a greater association between BMI and overweight/obesity, additional anthropometric measurements were analyzed, including waist circumference (WC) and neck circumference (NC). Each measurement was repeated twice to ensure accuracy, and the average used for analysis. Body weight was measured with a calibrated electronic SECA scale, model 813 with an accuracy of 0.1 kg. Height was measured with a portable SECA stadiometer, model 213 with an accuracy of 0.1 cm. The circumferences were measured with an inelastic SECA tape to the nearest 0.1 cm. Waist circumference of the participants was classified as an indicator of central obesity, if measurements for men and women exceeded 90 cm and 80 cm respectively 18. The cut-off values used for NC in this study were ≥ 37 cm in men and ≥ 35 cm in women 19. These measurements were collected by certified nutritionists/dietitians. Each measurement was repeated twice to ensure accuracy, and the average used for analysis.
STATISTICAL ANALYSIS
Descriptive statistics were used to summarize the baseline characteristics of study participants. Continuous variables are described as mean ± SD and categorical variables, as counts and percentages. We use chi-square, one-way ANOVA and Kruskal-Wallis tests to examine differences among groups, as appropriate. All tests of significance were two tailed. In addition, in order to find a correlation between neck circumference and the rest of anthropometric measurements, a Pearson's correlation test was used. Statistical significance was based on a p-value of < 0.05. Finally, in order to compare the utility of neck circumference with waist circumference, regression analysis was used. All data was analyzed by using SPSS 20.0 software and R for Mac v. 3.2.2.
RESULTS
Out of 908 eligible participants initially assessed in the first visit, 850 participants completed two visits and 800 participants met our inclusion criteria, analysis inconsistencies and partially missing data (Fig. 1).
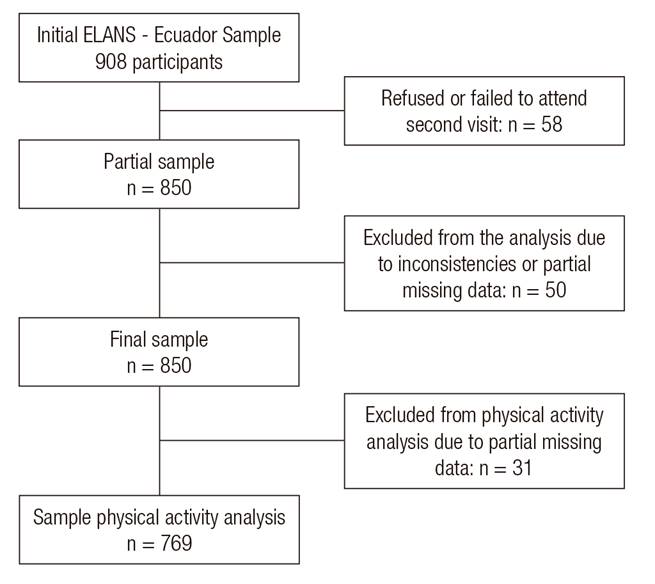
Figure 1. STROBE flow diagram of the study participants in the Latin American Study of Nutrition and Health - Ecuador
The study sample (n = 800) represented a population of whom 50.4% were female, 39.5% were individuals aged 20 to 34 years, 55% were living in the coastal region, and 49.9% of the participants reported a low socioeconomic status. Overall 73.1% of participants reported breakfast intake in both recalls, 20.3% of participants reported breakfast in one of two recalls, and 6.6% individuals reported to have skipped breakfast in both recalls (Table I).
Table I. Characteristics of study participants
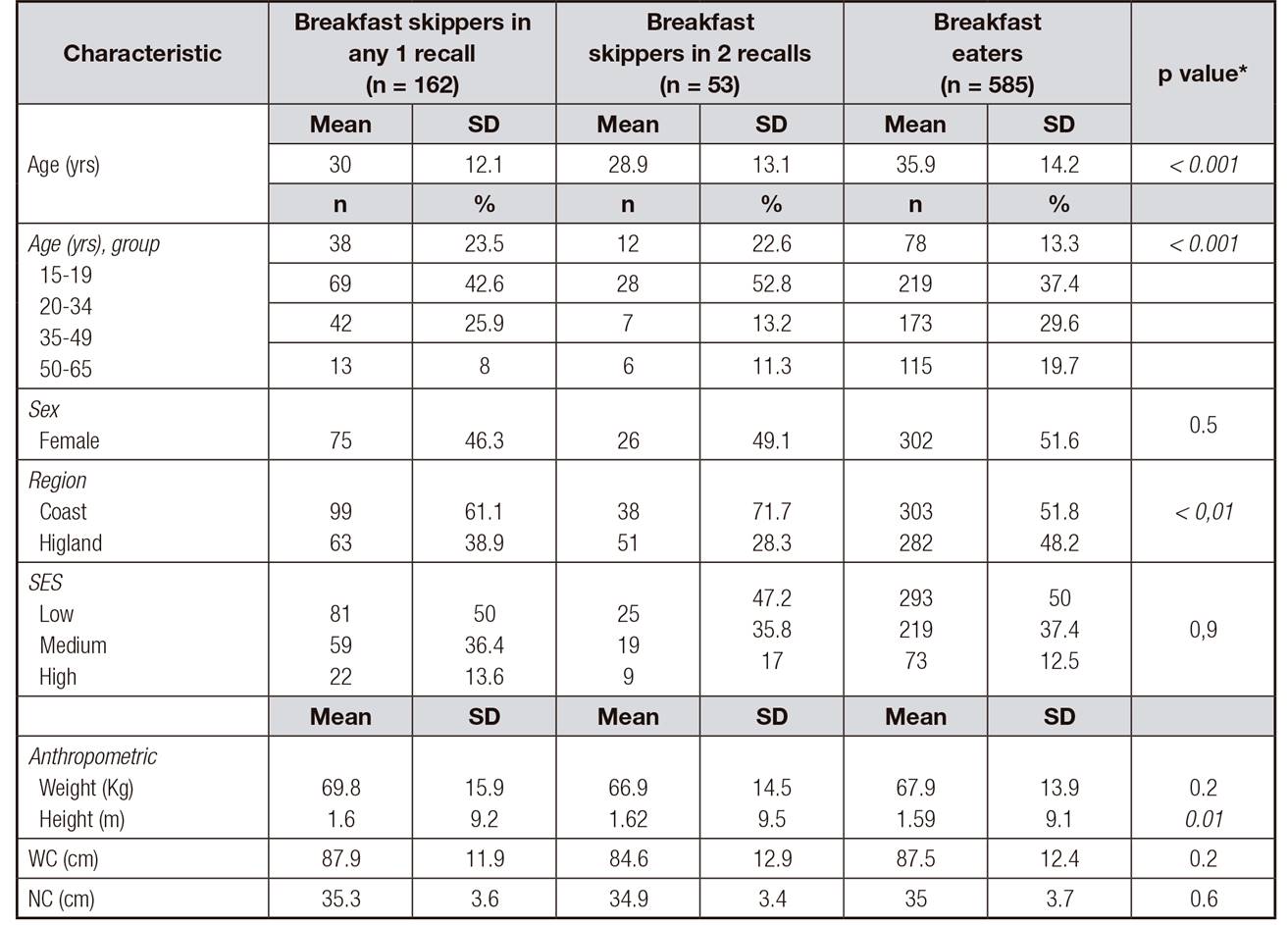
SES: socioeconomic status; WC: waist circumference; NC: neck circumference.
*p value for the difference among breakfast skippers in any 1 recall, breakfast skippers in 2 recalls, and breakfast eaters; statistically significant value (p < 0.05) indicated in bold font.
The majority of the participants who skipped breakfast in one or both recalls were most likely to be young adults 20 to 34 years of age and reside in the coastal regions of the country. In addition, most of the breakfast skippers were categorized as being low socioeconomic status.
Table II shows that individuals, who were more likely to skip breakfast, had an overall poor nutritional status according to their BMI, WC and NC, although it was not statistically significant (p > 0.05). Approximately 59% (127) of breakfast skippers (BS) were overweight or obese according to their BMI, while 60.7% (355) of the breakfast eaters (BE) were found to be overweight or obese using the same anthropometric measurement. Furthermore, 57.1% of the total sample had a positive indicator of central obesity through their WC measurements, and 26.7% of them are breakfast skippers. Neck circumference did not demonstrate a statistical association between being overweight and not reporting breakfast consumption, with only 39% of the BS showing upper trunk adiposity (p > 0.05). Overall, the study sample showed that 45.4% of individuals reported a medium level of physical activity but as the breakfast skipper groups were analyzed (BS in any 1 recall and BS in 2 recalls), there is a tendency to have a low physical activity level, 28.6 vs. 41.2%, respectively (p>0.05).
Table II. Association between breakfast patterns, anthropometric measures and level of physical activity
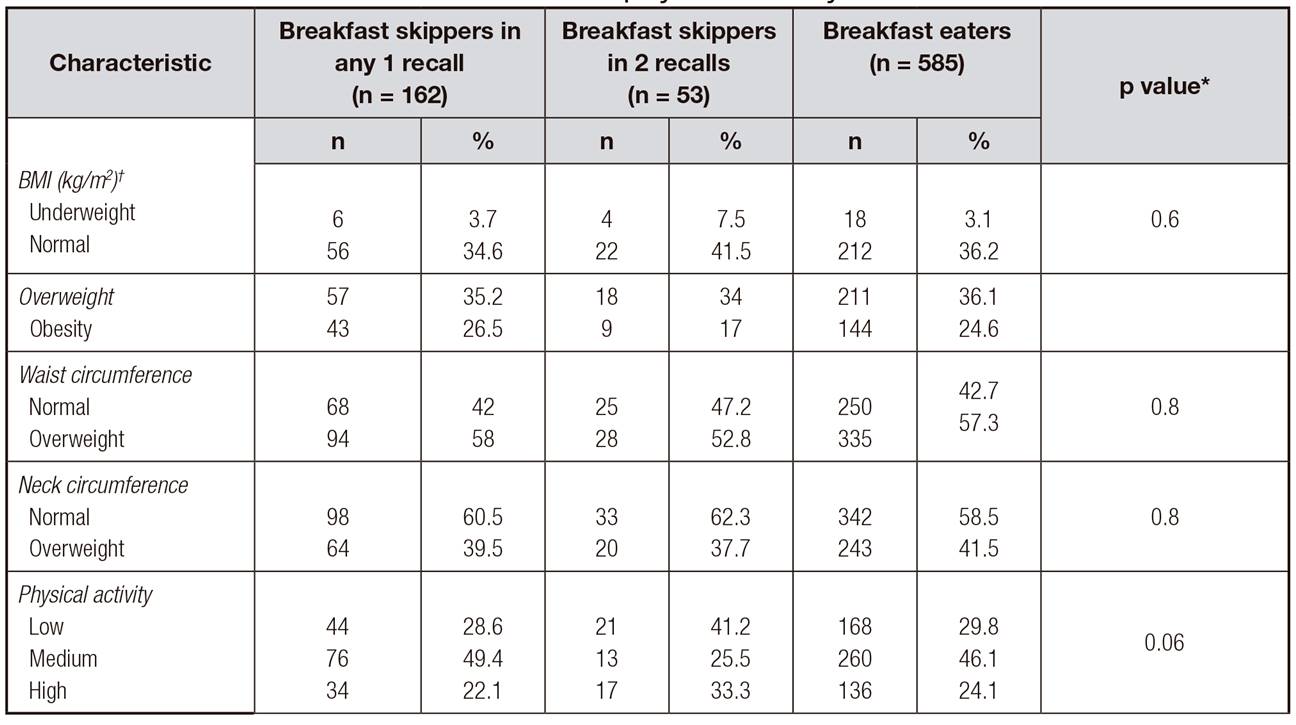
BMI: body mass index.
*p value for the difference among breakfast skippers in any 1 recall, breakfast skippers in 2 recalls, and breakfast eaters; statistically significant value (p < 0.05) indicated in bold font. †BMI groups: underweight < 18.5 kg/m2; normal 18.5-24.9 kg/m2; overweight 25-29.9 kg/m2; obesity > 30 kg/m2.
†BMI groups: underweight < 18.5 kg/m2; normal 18.5-24.9 kg/m2; overweight 25-29.9 kg/m2; obesity > 30 kg/m2.
In terms of nutritional quality, BS were most likely to consume less total calories, protein, carbohydrates, fat, sugar, fiber, and calcium compared to BE. Thus, breakfast eaters consumed a much higher amount of protein, exceeding the daily recommendation (46-56 grams/day) by ~54%. The amount of carbohydrates and total fat consumed were within acceptable ranges across all groups. Furthermore, breakfast skippers on average consume approximately 56% of the adequate intake of fiber (25-38 grams for men and women), compared to a 68% of fiber consumed by breakfast eaters (Table III).
Table III. Mean daily energy intake of breakfast skippers compared to breakfast eaters
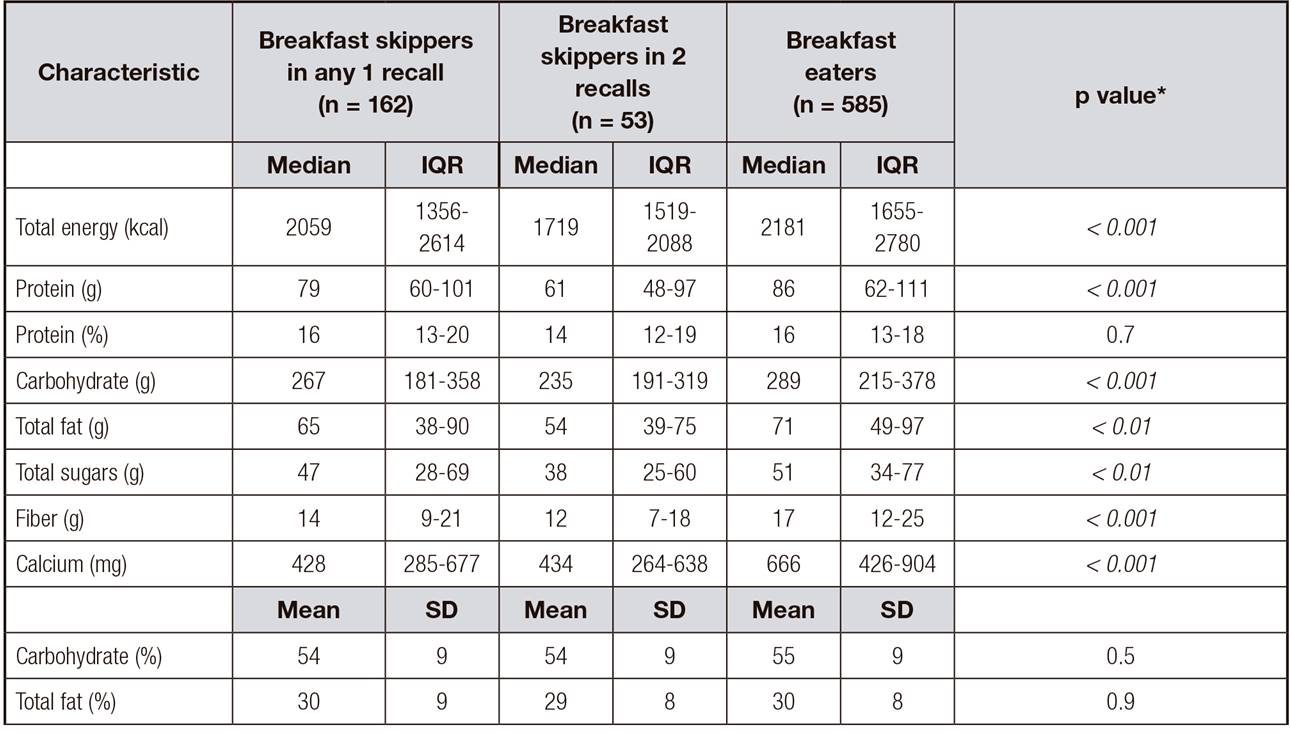
*p value for the difference among breakfast skippers in any 1 recall, breakfast skippers in 2 recalls, and breakfast eaters; statistically significant value (p < 0.05) indicated in bold font.
Male breakfast skippers on average consumed 1913 (1400-2558) kcal and female breakfast skippers reported a consumption of 1706 (1276-2365) kcal on the days they omitted the first meal of the day, neither sex reaching their total energy intake recommendation (2500 kcal and 2000 kcal for men and women, respectively). In addition, male breakfast skippers were more likely to consume lower macronutrients and micronutrient quantities with the exception of total sugar compared to male breakfast eaters. However, among women breakfast skippers only the consumption of total sugar, fiber, and calcium were lower compared to breakfast eaters (Table IV). In addition, although neither group consumed the estimated average requirement (EAR) of calcium (1000-1500 mg), both male and female breakfast skippers consumed 43% of the EAR (Table IV).
Table IV. Mean daily energy intake of breakfast skippers vs. breakfast eaters according to sex
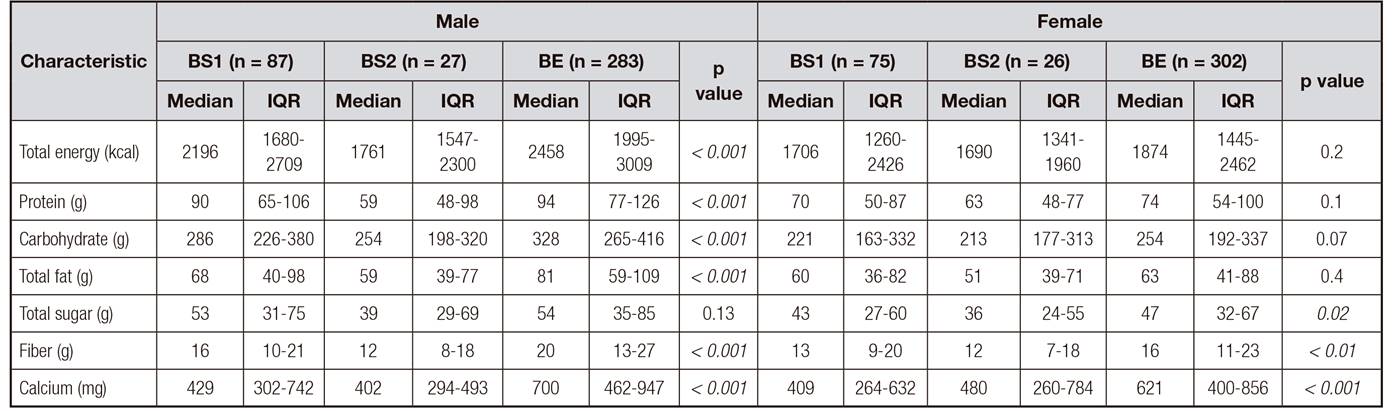
BS1: breakfast skippers in any 1 recall; BS2: breakfast skippers in 2 recalls; BE: breakfast eaters.
*p value for the difference among BS1, BS2, and BE by sex; statistically significant value (p < 0.05) indicated in bold font.
When comparing breakfast skippers from the coastal and highland regions of Ecuador, we found that BS within the coastal region in overall consume less total amount of energy, macronutrients, and micronutrients compared with BE. Further, when comparing BS from both regions there was a tendency to have a higher intake of total energy, total fat, total sugar, fiber and calcium in the highland than that of the coastal region (Supplementary Table I). Overall, the consumption of protein, carbohydrate, fiber, and calcium were higher in BE across age stratum. In addition, the consumption of sugar was higher in the younger age group (Supplementary Table II).
Supplementary Table I. Mean daily energy intake of breakfast skippers vs. breakfast eaters according to geographical region

BS1: breakfast skippers in any 1 recall; BS2: breakfast skippers in 2 recalls; BE: breakfast eaters.
*p value for the difference among BS1, BS2, and BE by sex; statistically significant value (p < 0.05) indicated in bold font.
Supplementary Table II. Mean daily energy intake of breakfast skippers vs. breakfast eaters according to age groups

BS1: breakfast skippers in any 1 recall; BS2: breakfast skippers in 2 recalls; BE: breakfast eaters.
*p value for the difference among BS1, BS2, and BE by age group; statistically significant value (p < 0.05) indicated in bold font.
DISCUSSION
The present study of a nationally representative sample of the Ecuadorian population based on the ELANS study shows that ~7% of middle-aged adults have skipped breakfast. This pattern was most prevalent among those individuals aged 20 to 34 years and residing in the coastal region of the country. We were not able to find an association between skipping breakfast and being overweight/obese, nor achieving a low level of physical activity. However, several associations where established between the breakfast skipping groups and the breakfast eaters when analyzing their nutrient intake.
BREAKFAST CONSUMPTION
In our study, the prevalence of breakfast skipping was low. This is consistent with several studies worldwide. For example, studies in Croatia and the UK reported low prevalence as 1.7% and 6% of breakfast non-consumption 20,21, respectively. Although this study did not identify a predominant sex that skips breakfast, various studies have found that the female sex is more likely associated with breakfast omission 21. Furthermore, our study found that the young adult age group (ages 20 to 34) that has been identified as those who frequently skip breakfast, have a normal body adiposity distribution, which can be explained through numerous factors. First, this study does not analyze the timing or number of remaining meals of the day, which may have a compensating influence on the nutritional status 22. Secondly, the younger adult group is consistent with other studies and other obesity-related eating habits, as well as being part of a "social business eating pattern", which is characterized by busy schedules, unhealthy food choices and frequent eating out 4,21. Finally, the normal body adiposity distribution may reflect the efficiency of the metabolic rate that this younger group has in comparison to the older age groups 23.
ENERGY AND NUTRIENT INTAKE
The breakfast omission is being known to be associated with lower 24-hour energy intake; our study found that energy intake was significantly different across breakfast categories. As such breakfast consumption was usually associated with a greater reported energy intake compared to breakfast skipping, indicating a large energy intake throughout the day in accordance with their first meal of the day. Total sugar, fiber and calcium were evaluated in this study, due to its nutritional importance in the breakfast meal. An association was found between groups, when analyzing protein, carbohydrate, total fat, total sugars, fiber and calcium. It seems that skipping breakfast lead to a reduced consumption of these macro and micronutrients. This could be due to several factors, including socioeconomic status and time management. A greater amount of protein was consumed on breakfast day by men than the days that breakfast was omitted, as well as fiber and calcium, despite the recommended requirements for calcium not being met in any of the breakfast groups. Females consumed a statistically significant amount of total sugar, fiber and calcium on the days that breakfast was consumed compared to those who chose to skip breakfast. This shows the tendency for women to reach for foods with a higher amount of sugar throughout their day 24. There were notable differences in nutrient intakes when comparing participants from the coastal and highland regions of Ecuador. Thus, the amount of fiber consumed daily in the coastal region is significantly less, which should be adjusted in order to maintain bowel health, lower cholesterol levels, help control blood sugar levels and aid in achieving a healthy weight 22,23. In addition, there is evidence reporting that micronutrient-rich breakfasts and morning meals are potentially satiating and have a beneficial effect on appetite regulation, which helps balance the energy intake throughout the day and prevent overeating and subsequently obesity 4.
ANTHROPOMETRY
Our results did not demonstrate that breakfast skipping was associated with overweight or obesity in the study sample analyzed by various anthropometric indices including BMI, WC, and NC. Being as this is a cross-sectional study that analyzed only two 24-hour recalls, it does not reflect the daily eating habits of an individual. Eating breakfast may also reflect better lifestyle and food choices across the day, explaining some of the limited association we observed with anthropometric measures.
Although it was not statistically significant, over half of the breakfast skippers being overweight or obese, may reflect this obesity-related behavior. In addition, most of the breakfast eaters were also classified as overweight or obese, which may be due to the nutritional quality of their diet, lack of physical activity or a combination of eating habits that should be analyzed in future studies.
PHYSICAL ACTIVITY
Our study demonstrated a self-reported medium level amount of physical activity amongst the participants who skipped breakfast in one or two recalls. This can be explained by the following reasons: the participants reported a socially-acceptable amount of physical activity, the participant consumed a compensatory meal or meals following the lack of breakfast, or their dinner time and/or amount of energy intake led to the omission of the first meal of the day. In a study that analyzed a sample of US adolescents and young adults, they reported similar results 25, in that there was no association found between skipping breakfast and meeting physical activity guidelines for age among US adolescents and young.
IMPLICATIONS
Despite the fact that two recent clinical trials conducted in lean and obese adults has not found noteworthy differences between breakfast intake and weight change 26,27, literature shows that skipping breakfast can lead to multiple health consequences with long term implications such as heart disease, atherosclerosis, and type 2 diabetes 4. Furthermore, there is evidence showing that having a regular breakfast in lean individuals can maintain insulin sensitivity and glycemic control 27,28; and a large breakfast rich in protein and fat improves glycemic control in type 2 diabetes 29. Thus, there are important health benefits of regular breakfast consumption beyond mere weight management, which should be taken into account by health professionals, key stakeholders and mass media.
STRENGTHS AND LIMITATIONS
There are several strengths that this study possesses, including the large representative sample of the Ecuadorian population. To the best of our knowledge this is the first study that analyzes the association between breakfast skipping and nutritional status, including physical activity in an ethnically diverse adult population in a Latin American country. In addition, this study utilizes a novelty anthropometric measure, neck circumference, as one of the parameters to evaluate adiposity. Numerous limitations have been identified in this study, as well. The exposure, breakfast skipping, was measured based on two 24 hour dietary recalls. It is possible that participants may have given socially desirable responses by reporting eating breakfast when they actually did not consume any food during breakfast or that they reported an incorrect amount of physical activity. Furthermore, the two recalls may not have appropriately captured participants' typical dietary behaviors. For example, it may not be accurate to classify someone who skipped breakfast on one or two days, as a breakfast skipper, even though this method has been used in previous studies, thus exposure misclassification may be possible. For future studies, should be considered to add an additional dietary recall (in total three 24-hour dietary recalls). And lastly, it does not describe the long-term effects of this eating habit and have no follow-up data on our participants due to its cross-sectional design.
CONCLUSIONS
The present study found that ~ 7% of middle-aged adults in Ecuador have skipped breakfast. This eating behavior was not associated with being overweight/obese or achieving a low level of physical activity. However, an association was found between breakfast skipping and a reduced consumption of protein, carbohydrate, fiber and calcium in their diet. It is important to consider the long-term health consequences (heart disease, atherosclerosis, and type 2 diabetes) of this unhealthy behavior that can be avoided by changing this eating habit in the population and not only see it as a mere weight management strategy.

