










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Obesity is the most common nutritional disorder among infants and adolescents in both industrialized and emerging societies (1). The prevalence of obesity has steadily increased recently. This increased prevalence is associated with the increased availability of food and changes in lifestyle, including increased physical inactivity, decreased physical activity in children and adolescents, and poor eating habits (2).
In particular, childhood obesity is a risk factor for cardiovascular, orthopedic, respiratory, digestive, dermatological, psychosocial, physical, neurological, and endocrine complications. Childhood obesity is also associated with certain forms of cancer and lower life expectancy, which justifies the prevention and early treatment of childhood obesity (3).
Research indicates that obese people have greater difficulty controlling their impulses than thin people (4). In this regard, obese individuals in weight reduction programs receive higher scores on scales that assess impulsivity, and they more frequently engage in impulsive behaviors, including substance abuse, than thin people (5,6). Impulsive individuals are less likely to engage in various behaviors that contribute to healthy eating patterns (7).
Impulsiveness might affect the ability of an individual to plan meals, eat regularly, and resist impulses to enjoy foods that are high in fat and sugars (8). In addition, research shows parallels between obesity and potentially addictive behaviors in adults – both obesity and addiction are characterized by impulsive behaviors and increased reward sensitivity (9).
This relationship is particularly important because of the prevalence of food availability in industrialized societies. In addition, a variety of environmental factors have changed over the last 30 years that are associated with increased obesity; for example, the increasing number of fast food restaurants enables greater access to cheap meals that are high in calories and fat (10). Consequently, the chance of overeating increases when greater food reward sensitivity exists (11). For example, both laboratory and real-world studies have shown that exposure to appetizing environments is more effective at increasing food intake but only among participants who are highly responsive to reward (12,13). In this sense, it is more difficult for obese people to resist the temptation to overeat, despite the negative consequences that this behavior might lead to in terms of health and quality of life (14). This finding suggests that reward sensitivity is a causal mechanism for overeating in an obesogenic environment.
In this regard, several explanations for the mechanisms that underlie the ability to control impulsiveness have been proposed. One potential and suitable mechanism is reinforcement delay, which refers to the relative preference for immediate but small rewards compared with larger but delayed rewards (15). Reinforcement delay has considerable potential to improve our understanding of the behavioral processes associated with numerous problematic behaviors, including those associated with overweight and obesity (16). Research on this matter shows that obese children choose small but immediate rewards and exhibit difficulty with postponing gratification when large meal portions are presented as alternatives (17) primarily because they are more sensitive to rewards than children of normal weight (18). In addition, recent research has demonstrated that the inability to delay gratification predicts weight gain in children between the ages of 3 and 11 years (19 20-21). The use of this basic paradigm emphasizes the value of the reward depending on delayed access to said reward as compared with another selection presented concurrently.
Research in this area has been limited to programs associated with different amounts of the reinforcer and variations in the delay of the reinforcer of a greater magnitude. In some cases, however, the delay of the latter may involve additional enhancing dimensions available within the individual's environment, such as the quality of the reinforcer, the effort of the task, and the reinforcement program. The procedures developed by Neef and Lutz (22) were successfully used to assess the relative influence of reinforcer dimensions on children's impulsive behaviors and to develop self-control and decrease impulsive behaviors through the use of basic development models of self-control, such as the fading procedure (23).
However, the literature on impulsive behavior in obese and non-obese people has focused primarily on evaluation rather than treatment because, in many cases, impulsivity is evaluated using inhibition response assignments or psychometric instruments. Currently, the focused evaluation of impulsive choice affected by reinforcer dimensions has enabled the development of procedures that increase self-control based largely on the fading procedures of late delivery of a reward of lesser value or gradual increase in the delay of a reward of greater value (23 24 25-26). Therefore, the objectives of this study were to evaluate the relative influence of different reinforcer dimensions (e.g., rate, quality, effort, reinforcement delay) on the choice behavior of overweight and obese children, as well as to identify relevant combinations of these dimensions to promote self-control.
METHODS
PARTICIPANTS
Weight and height data were obtained from measurements performed by health personnel to determine the children's body mass index (BMI; weight [in kg]/height [in m2]) and to identify cases of overweight/obesity. The children were grouped into two categories based on the International Obesity Task Force (IOTF) age- and gender-specific child BMI cutoff points of 25 kg/m2 for overweight and 30 kg/m2 for obesity (27). A total of 14 children between 8 and 10 years of age (mean = 9.14 years), including seven girls and seven boys, participated in the present study. Of the 14 participants, eight were obese and six were overweight. All children attended elementary school on the east side of Mexico City. In addition, parents signed an informed consent form.
MATERIALS AND CONDITIONS
Impulsive behavior was evaluated using a software program similar to that described by Neef and Lutz (22). This program is used to evaluate behavior through selections chosen for two sets of math problems concurrently displayed on a computer screen. Each set of math problems varies in terms of specific dimensions, including reinforcer quality, immediacy of reinforcement, reinforcement rate, and response effort. Furthermore, each dimension is framed within a set of visual elements that inform the dimensions associated with each addition. These characteristics are described below.
Immediacy (I)
In this study, immediacy of a reinforcer refers to the amount of time that a child must wait to access the reinforcers earned by correctly answering the selected arithmetic problem. The amount of time varied from immediately after the end of the session to a time delay of 30 minutes, one hour, three hours, five hours, or 24 hours. In case of immediacy, when the child had access to the reinforcer it was indicated inside a blue rectangle with white letters.
Quality (Q)
Quality refers to a child's relative preference for the reinforcers associated with two problem sets. Reinforcers were sampled from 10 base items to define the categories of high and low quality. The high-quality reinforcer category was built with the three most preferred items, and the low-quality reinforcer was built with the three least preferred items. The reinforcers used were stickers of cartoon characters that were attractive to the children. They were paired with images of healthy foods in the case of high-quality reinforcers or images of high-calorie foods of low nutritional value in the case of low-quality reinforcers. The food was sampled to determine relative food preferences, i.e., preferences for healthy and unhealthy foods. Images of food were presented in the lower part of the selection set.
Reinforcement rate (R)
This variable refers to the concurrent reinforcement program in effect on a respective set of sums. A VI5-s schedule was used for the high reinforcement rate, a VI15-s schedule was used for the medium reinforcement rate, and a VI30-s schedule was used for the low reinforcement rate. The visual element of reinforcement rate was the background color of the arithmetic problem: yellow represented a high rate, red denoted a low rate, and white was a medium rate.
Response effort (E)
This variable refers to the relative difficulty associated with solving an arithmetic problem. In this experiment, effort was based on the difficulty of the addition problems, from 1 to 5 included digits. Judges validated this protocol by evaluating the relative difficulty of the problems to verify that the children perceived these ranges of difficulty in the same way.
In the beginning, the software displayed a menu where the researcher selected the relative values for the reinforcer dimensions associated with each set of arithmetic problems. Subsequently, the program presented the instructions, and the researcher read them to the child. If the child had no questions about the instructions, then the researcher presented the first choice on the screen, displaying two arithmetic problems: one on the right side and one on the left side. The researcher explained each of the characteristics of the set of arithmetic problems. Next, the child began the evaluation without the help of the investigator. The computer program was designed to record the number of choices made for each problem, the dimension associated with this choice, the number of successes and failures, the points obtained for each reinforcer, and the time delay before the reinforcer could be accessed.
Impulsive behavior
This variable was measured using the definition of Neef, Marckel, et al. (28), in which the evaluation conditions 'Reinforcement rate' against 'Immediacy', 'Quality' against 'Immediacy', and 'Immediacy' against 'Effort' reflect a measure of impulsivity when the individual chooses arithmetic problems that provide immediate reinforcement.
When the child chose his or her preferred option within the set, the program showed a new screen called the “screen response”, which displayed only the selected arithmetic problem on the screen and a virtual clock indicating how much time was left to complete the problem. After the allotted time interval based on the reinforcement program, multiple response options were displayed on the screen, and the child was able to enter the correct answer using a mouse. If the answer was correct, then feedback was provided in the form of a pop-up window with the expression “Very Good”, and a point was added to the corresponding reinforcer. If the answer was wrong, then a pop-up window with a red X indicating that the response was incorrect would appear. The researcher decided how many screens of choice were presented based on the evaluation phases.
PROCEDURE
At the beginning of each session, the relative preferences of the children were evaluated through a sampling procedure of reinforcement with 10 different types of stickers of their favorite cartoon characters. The program differentiated the three most preferred stickers (high reinforcers) and the three least preferred stickers (low reinforcers) to determine the quality dimension (Q). The most preferred stickers (high quality) were paired with images of healthy foods (e.g., salad, fruit, and home-cooked food), while lower preference stickers (low quality) were paired with high-calorie foods of low nutritional value (e.g., fast foods such as burgers, pizza, and soda). Stimulus pairing was presented for all tests.
The condition of pairing stickers with foods respected the federal norm regarding the inclusion of unhealthy foods in elementary schools in Mexico. In this sense, the tangible item to deliver was the sticker, not the food.
Baseline
At this stage, a choice screen was presented to the child, and each pair of math problems differed by only one dimension (immediacy, quality, rate or effort) per session. For example, a choice screen with the condition of immediacy against delay was formed by two sets of arithmetic problems, both showing a problem of low difficulty associated with a reinforcer of the same quality and with the same rate of reinforcement; however, one was delivered at the end of the session, and the other was delivered the next day. The objective of this condition was to establish the child's sensitivity to each dimension in isolation (high quality versus low quality, high effort versus low effort, high reinforcement rate against low reinforcement rate, or immediacy against delay). This procedure allowed us to evaluate the capacity of intradimensional discrimination for reinforcer dimensions.
The baseline period lasted approximately 15 minutes or until more than 80 % of selections were for the option with the highest reinforcer value.
Evaluation phase
The objective of this phase was to evaluate impulsive behavior. All dimensions were put in direct competition through paired comparisons of six evaluation conditions: quality against immediacy, quality against effort, quality against reinforcement rate, immediacy against effort; immediacy against reinforcement rate, and effort against reinforcement rate.
This procedure allowed us to obtain a measure of the proportion of preference for an option associated with one of two reinforcement dimensions. That is, under the matching theory (29,30), this procedure measured the effect of a reinforcer on behavior in the context of other reinforcers for concurrent response options.
As a baseline, the children chose, based on their preferences, one of the food-character pairs associated with the arithmetic problems that appeared on the choice screen. The evaluation session lasted 15 minutes or until all 30 choice screens were completed.
Self-control training phase
During this phase, the fading principle described by Mazur and Logue (24) was applied. In the first session, the minimum values of the dimension that generated more impulsive behavior (immediate) and the dimension that led to the devaluation of the reinforcing value (effort or reinforcement rate) were used for both choices; quality was the only dimension in direct competition (high quality against low quality). The session ended when the child preferentially selected one of the two options 80 % of the time. In subsequent sessions, the value of the dimension associated with high quality increased gradually up to the original values, which were presented during the evaluation phase.
Follow-up and post-evaluation phases
The follow-up and post-evaluation phases were conducted under the same conditions to determine the effect of the self-control training program in relation to the competing dimensions. During the follow-up phase, the baseline conditions were replicated (only one dimension competed against the four evaluation conditions), while during the post-evaluation phase the evaluation conditions were replicated (two dimensions competed across six evaluation conditions).
RESULTS
For each child being evaluated the number of choices was quantified per competing dimension for each of the evaluation conditions throughout the trials. The individual responses of each participant are presented in table I. The proportion of choices for the option associated with a dimension is presented on the left side, while the selections for the competing dimension are presented on the right side. For example, at baseline, when the evaluation condition was the direct competition of high-quality against low-quality reinforcement (HQvsLQ), child 3 assigned 60 % of his choices to healthy foods associated with higher-value stickers, while the remaining 40 % were assigned to unhealthy foods associated with lower-value stickers. After the intervention, the same child assigned 100 % of his choices to the healthy foods associated with the high-quality reinforcer. In this sense, the sensitivity to the quality of the reinforcer was more acute after the intervention. In the quality against immediacy evaluation, one option consisted of unhealthy food associated with the immediate delivery of a low-quality reinforcer, while the other option consisted of healthy food associated with the delayed delivery of a high-quality reinforcer. In this condition, the same child assigned 60 % of his choices to the condition associated with the higher-quality delayed reinforcer (exhibiting self-control), while he assigned the remaining 40 % of his choices to the option with the immediate delivery of the lower quality reinforcer. Subsequent to treatment, the child assigned 100 % of his choices to healthy food associated with the highest-quality reinforcer, despite a delay in access to the reinforcer of up to 24 h.
Table I. Percentage distribution of choices along reinforcer dimensions for evaluation conditions and experiment phases

HQ: high quality; LQ: low quality; I: immediacy; D: delayed; HE: high effort; LE: low effort; HR: high reinforcement rate; LR: low reinforcement rate; CvsI: quality versus immediacy; QvsE: quality versus effort; QvsR: quality versus reinforcement rate; IvsE: immediacy versus effort; IvsR: immediacy versus reinforcement rate; IvsE: effort versus reinforcement rate.
The average percentages and standard deviations for each condition across the four reinforcer dimensions, which indicate the changes related to the sensitivity to reinforcer dimensions and their effects on food choice, are shown in figure 1.

Figure 1. Average percentages and standard deviations of choice allocated to response alternatives across assessment conditions (HQ: high quality; LQ: low quality; I: immediacy; D: delayed; HE: high effort; LE: low effort; HR: high reinforcement rate; LR: low reinforcement rate; QvsI: quality versus immediacy; QvsE: quality versus effort; QvsR: quality versus reinforcement rate; IvsE: immediacy versus effort; IvsR: immediacy versus reinforcement rate; IvsE: effort versus reinforcement rate).
In the upper panel, the quality of the reinforcer is shown, and the relative preferences (before and after) are plotted for the baseline and evaluation conditions. The choice of quality exhibited high variability among participants before treatment; that is, they had a greater number of impulsive behaviors before treatment. In contrast, after treatment, most participants preferentially assigned their answers to the quality of the reinforcer as opposed to the dimensions in competition, showing greater self-control. With regard to immediacy, the same effect as with quality was observed but in favor of self-control; that is, a preference for other dimensions rather than immediacy of reinforcement was shown. In the case of effort and reinforcement rate, the effect was clearer when competing against quality. Among immediacy, reinforcement rate and effort, however, the effect varied across participants.
After the delayed reinforcement procedure all frequencies of the total selections of each reinforcer dimension were graphed (see Fig. 2). As shown, all dimensions showed differences before and after the intervention.
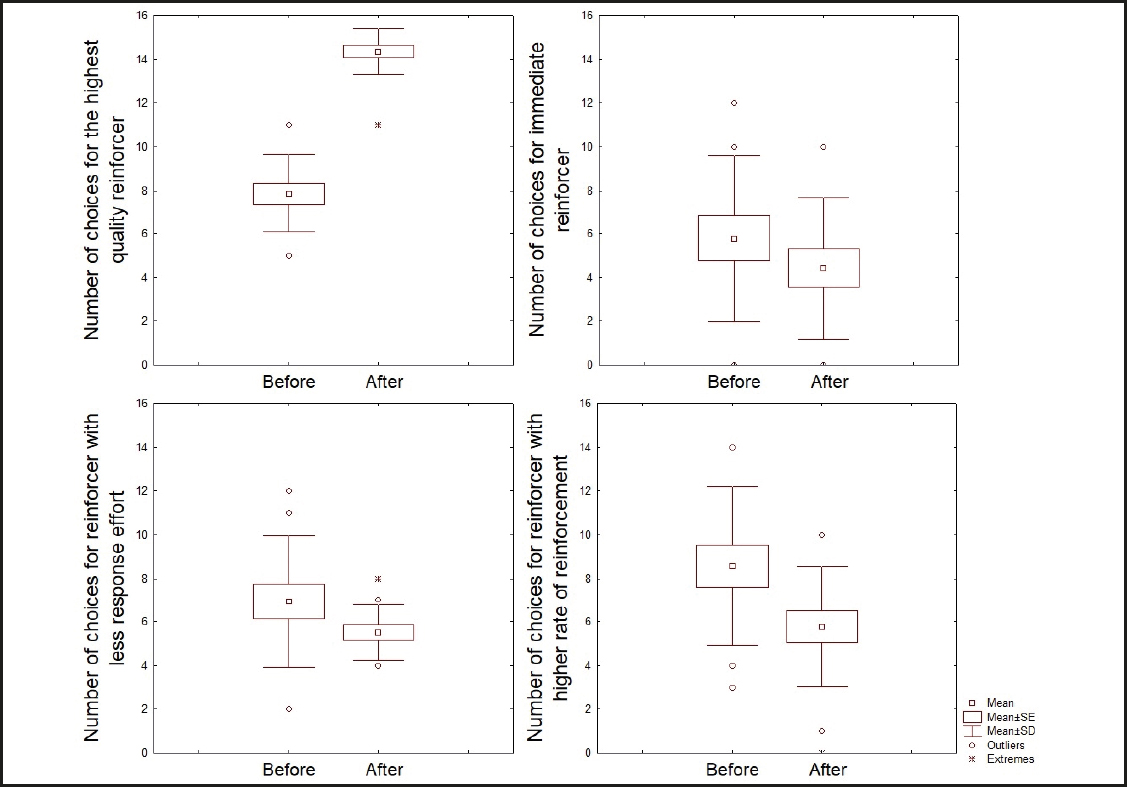
Figure 2. Comparisons before and after the intervention with regard to the children's choices for each reinforcer dimension.
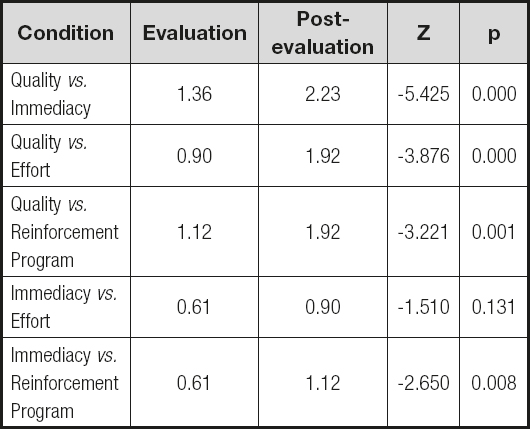
To identify whether these differences were statistically robust, a nonparametric Wilcoxon test with repeated measures was conducted to determine the existence of differences before and after the procedure with regard to the total number of selections in each reinforcer dimension. The results of the analysis are shown in table II. Furthermore, comparative analyses were performed before and after the intervention to ensure that the process of self-control development led to changes in the number of impulsive behaviors and a devaluation of the quality reinforcer of a higher value; a nonparametric Wilcoxon test was used for each evaluation condition. The results are shown in table III.

DISCUSSION AND CONCLUSION
Our results showed that children with overweight or obesity exhibited changes in their preferences. For example, children who chose low-quality but immediate reinforcers with less effort or with high reinforcement rates (associated with unhealthy food) changed their choice to higher-quality reinforcers associated with healthy food despite the additional delay, and this change involved greater effort or a lower reinforcement rate.
These results are similar to those described in the literature (23,28,31). For example, the children's selections showed a greater reinforcement delay even with regard to the dimensions that were not manipulated directly via the fading process. Importantly, however, many children associated some of their responses with unhealthy foods at baseline, perhaps because of their initial bias for high-calorie foods.
In general, and for most participants, the fading strategy led to a change in preferences for the conditions in which the gain was a reinforcer of higher quality despite its delay (24 hrs). During the intervention phase, participants generally showed changes in their choices of unhealthy food over healthy food, as well as with regard to the dimensions during the intervention phase (immediacy, reinforcement program and effort), through the gradual increase in reinforcer delay (24,32).
According to the results collected during the follow-up and post-evaluation phases, the participants maintained their preferences for healthy food and showed self-control with regard to the dimension in which they were trained, even for those that were not manipulated directly via the delayed reinforcement procedure (23).
The current study extends the research on self-control in humans with the use of procedures of choice influenced by reinforcer dimensions among overweight and obese populations. The current data extend the generalization of tasks and procedures to the development of self-control as well as to the problems of overweight and obesity, which are associated with low impulse control (8,33) and the devaluation of delayed rewards (34).
In terms of applicability, the present investigation started with the assumption that the value of a reinforcer is relative to the options of reinforcement that are available and the reinforcer dimensions associated with each option. This position is easily applicable to feeding behavior, which is viewed as a choice that depends on the motivational state of the individual and the availability of food. In the current scenario, a wide variety of reinforcement options are modeled between consumption and synergy, with the food industry offering (among other things) foods with high calorie content (Q), foods that are easily accessible (E), foods offered more frequently (R), and foods that are ready to eat (I). However, sensitivities to these dimensions are susceptible to modification via behavioral procedures such as fading. The process of fading of the reinforcer delay or of the value of the competing dimension is one example of how an individual's experience can determine his or her subjective estimation of time and organize his or her choices in favor of self-control or impulsivity, in the sense that individuals with little exposure to delayed conditions with a high probability of reinforcement tend to behave more impulsively. In the case of healthy food options the same happens: children have more immediate access to the relatively small benefits of unhealthy food and have little experience with the delayed benefits of consuming healthy food. Therefore, their estimate of the sizes of the reinforcer or the response dimensions accompanying food are biased in favor of junk food, as was observed in the baseline results of this study before exposure to the associated reinforcers and fading procedure. Consistent with the results of previous research (35,36), overweight might be a consequence of the way people discount future health benefits.
In this regard, considering the impulsivity of children with overweight and obesity as a choice behavior, where the relative value of a high-quality reinforcer is devalued by delay, effort and reinforcement rate, enables the operationalization of part of the problem and thereby quantifies the progress achieved in scenarios with multiple enhancement options. To the extent that insensitivity to delayed consequences contributes to the emergence and maintenance of these behavioral problems, an understanding of the variables that control this temporary reduction is critical for the development of effective treatments (37).

