










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Cancer is the second leading cause of death in the world. The latest worldwide estimate, conducted in 2018, reported 9.6 million deaths due to cancer. And for each year of the 2020-2022 triennium, 625 thousand new cases are expected to occur (1).
Among the various complications triggered by cancer, malnutrition is one of the most prevalent, with a significant impact on response to treatment, length of hospital stay, hospital costs, increased risk of infections, reduced physical conditioning, worsened prognosis, and mortality (2,3).
Malnutrition affects on average 50.0 % of patients with cancer of the gastrointestinal tract (GIT) and adnexal glands (4). Planas et al. (5) observed nutritional risk in 47.9 % of patients with upper GIT cancer, in 39.1 % of those with lower GIT cancer, and of 45.0 % in patients with adnexal gland cancer.
Malnutrition is often associated with significant levels of skeletal muscle depletion, with progressive loss of strength, function, and muscle mass, which is commonly known as sarcopenia (6,7). The prevalence of sarcopenia in cancer patients is reported to be around 15.1 % (8), it being higher in those with GIT tumors (57.7 %) (9).
Sarcopenia can compromise health status, reduce quality of life, and increase mortality and treatment costs, especially when associated with malnutrition. However, its diagnosis requires expensive equipment that is not always available or accessible in clinical practice (6).
In this context, the SARC-F questionnaire is the first tool validated and accepted by the European Working Group on Sarcopenia in Older People (EWGSOP2) (6) as a test to assess the risk of sarcopenia, and consists of short, objective questions that assess muscle function and performance (10,11).
In order to improve the effectiveness of this tool, Barbosa-Silva et al. (12) suggested the inclusion of CalF circumference (CC) to SARC-F, for it is an indicator of muscle mass reserve. This adjustment improved the diagnostic accuracy and sensitivity of the instrument, increasing its ability to identify the risk of sarcopenia from 33.3 % to 66.7 % in the evaluated group. From then on, the instrument started to be called the SARC-CalF (12).
Given the negative impact of sarcopenia on cancer patients and the need to investigate the tools available for its screening and diagnosis, this study hypothesized that SARC-CalF is an instrument capable of identifying risk of sarcopenia in patients with cancer of the GIT and its adnexal glands, associated with the measures used in clinical practice to assess nutritional status. The aim of this study was to identify the risk of sarcopenia by SARC-CalF as well as the factors associated with this outcome in patients with cancer of the GIT and its adnexal glands.
MATERIAL AND METHODS
SAMPLE AND STUDY DESIGN
This cross-sectional, observational study was carried out in Vitória (ES), Brazil, from May 2018 to December 2019.
Patients aged 20 years or older, of both sexes, with a confirmed diagnosis of cancer of the GIT or its adnexal glands, were recruited, admitted to the General Surgery Unit for surgical treatment, and evaluated within the first 48 hours of hospital admission. Individuals with cognitive dysfunction reported in medical records, in respiratory isolation, in palliative care, or with edema and/or ascites were excluded.
This study was approved by the Research Ethics Committee of the Federal University of Espirito Santo (UFES), CAAE number 69321717.1.0000.5060. Patients volunteered for the study and provided their written informed consent.
CLINICAL AND SOCIODEMOGRAPHIC VARIABLES
Specific protocols were applied in order to collect sociodemographic information (age, sex, race/self-reported color). Clinical data such as tumor location and length of hospital stay were collected from the medical records. Tumor location was grouped into upper GIT, lower GIT, and adnexal glands (bile ducts, liver, and pancreas).
ANTHROPOMETRIC VARIABLES
For the present study, anthropometric variables were measured according to standardized protocols (13,14). Body mass (kg), height (m), arm circumference (AC) (cm), tricipital skinfold (TSF) (mm), CalF circumference (CC) (cm), and adductor pollicis muscle thickness (APMT) (mm) were measured.
Body mass index (BMI) was calculated by dividing current body mass (kg) by height in meters squared. Arm muscle circumference (AMC) and corrected arm muscle area (CAMA) were calculated according to validated equations (15).
APMT was measured according to the technique proposed by Lameu et al. (16). The procedure was performed three times in each hand, and the mean value obtained was considered for analysis. Cut-off points for malnutrition were considered to be < 13.4 mm for adductor pollicis muscle thickness in the dominant hand (DAPMT), and < 13.1 mm for adductor pollicis muscle thickness in the non-dominant hand (NDAPMT) (17). These measurements were not taken in patients with disabled hands.
HAND GRIP STRENGTH (HGS)
For the evaluation of handgrip strength we used the Jamar Hydraulic Hand Dynamometer® in both hands. The test was carried out according to the methodology recommended by the American Hand Therapy Association (ASHT) (18). The procedure was performed 3 times in the dominant hand (DHGS) and 3 times in the non-dominant hand (NDHSG), with maximum effort for about 5 seconds, with an interval of 1 minute between measurements. The test was not performed if the participant had undergone hand, arm, or forearm surgery less than 60 days before the procedure and/or had a venous access or edema of the upper limbs. Therefore, the HGS analysis was conducted with a reduced sample. The cutoff points were the ones defined by the European Working Group on Sarcopenia in Older People (EWGSOP2): < 16.0 kg for women and < 27.0 kg for men (6).
PATIENT-GENERATED SUBJECTIVE GLOBAL ASSESSMENT (PG-SGA)
Nutritional status was assessed using the PG-SGA. For this study, the validated version translated to Brazilian Portuguese (19) was used with permission from the PG-SGA/Pt-Global Platform (www.pt-global.org).
This version is divided into two parts. The first part evaluates issues related to the symptoms of nutritional risk, such as functional deficit, changes in weight, dietary changes and depression. The second part assesses questions based on factors associated with the presence of metabolic stress, percentage of weight loss in 1 month or 6 months, and the presence of other factors related to one’s health condition such as cancer, pulmonary or cardiac cachexia, decubitus ulcer, trauma, age over 65, and acquired immunodeficiency syndrome (AIDS). In this study, the evaluators assisted by reading the questionnaire and helping the patient to understand it. Nutritional status is classified into three categories: well nourished (A), suspected malnourishment or moderately malnourished (B), and/or severely malnourished (C).
This instrument also allows one to assess the need for nutritional intervention through the sum of scores at four levels: 0-1 points: without need for nutritional intervention; 2-3 points: nutritional education of the patient and his/her family should be provided; 4-8 points: need for nutritional intervention, and ≥ 9 points: critical need for nutritional intervention and symptom improvement. In the present study, we employed a global classification of well-nourished (A) and malnourished (B + C). The PG-SGA score was grouped into two categories: 0-3 points: no need for nutritional intervention or requires nutritional education provided to the patient and their family, and ≥ 4 points: requires nutritional intervention and symptoms control.
SARC-CALF
The risk of sarcopenia was assessed by through the SARC-CalF as validated for the Brazilian population (12). This instrument is structured into six components that assess difficulties related to strength aspects, use of walking aid, getting up from the chair, climbing stairs, number of falls, and finally the CC measurement. At the end of the evaluation a score ranging from 0 to 20 points is produced. Values between 0 and 10 are not suggestive of sarcopenia; values between 11 and 20 are suggestive of sarcopenia (12).
CC was measured at the point of greatest horizontal protuberance in the right CalF using an inextensible measuring tape. The patient was advised to stand up, with legs relaxed and feet 20 cm apart, according to the recommendation by Barbosa-Silva et al. The cut-off point used in the SARC-CalF, which considers the reduction in muscle mass, was a CC value below 34 cm for men and 33 cm for women (12).
In order to better assess the efficiency of the SARC-CalF - an instrument validated for elderly Brazilians - in detecting the risk of sarcopenia in this population, considering that this study is composed of individuals aged 20 years or older, data analyses were divided according to the classification of life stages used in Brazil: < 60 years for adults and > 60 years for the elderly.
STATISTICAL ANALYSIS
A descriptive analysis was performed expressed as means, medians, standard deviations, and minimum and maximum to describe continuous variables, and as percentage for categorical variables. The Kolmogorov-Smirnov test was used to verify the normality of quantitative variables. Length of stay, PG-SGA score, and SARC-CalF did not present a normal distribution. For the analysis and distribution of SARC-CalF mean scores according to categorical variables the Man-Whitney and Kruskal-Wallis tests were used. The correlation between SARC-CalF scores and continuous variables was analyzed using Spearman’s correlation according to stage of life. Correlation coefficients can vary from -1 to +1, being categorized as weak (r = < 0.3), moderate (r = 0.3-0.7) or strong (r = > 0.7) (20). A multivariate linear regression analysis (stepwise method) was applied to determine the influence of independent variables on the SARC-CalF score (dependent variable) according to stage of life. All variables that showed significance in the correlation test were included. Data were analyzed using the SPSS 22.0 software. The level of significance adopted for all tests was 5 %.
RESULTS
Seventy patients aged on average 58.2 ± 13.2 years were evaluated. Among these, there was a higher proportion of elderly (52.9 %), women (55.7 %), and non-whites (64.3 %). Tumors in the lower GIT were most prevalent, and were identified in 38.6 % of the subjects. All patients at this time received only surgical treatment (Table I).

Table II presents the nutritional diagnosis, risk of sarcopenia, HGS, and need for nutritional intervention of the patients evaluated here. According to the PG-SGA, 50.0 % of the patients had some degree of malnutrition (B + C), while SARC-CalF pointed to 28.6 % of the sample being at risk for sarcopenia. There was a predominance of adequacy for DHGS (78.8 %) and NDHGS (73.0 %) for both hands. Regarding APTM, malnutrition values were observed for DAPTM (59 %) and NDAPMT (59.7 %). The PG-SGA® score revealed that 90 % of the patients needed a nutritional intervention. The median PG-SGA score was 10, indicating a need for nutritional intervention, while the SARC-CalF was 6.50, indicating absence of sarcopenia.
Table II. Nutritional status, risk of sarcopenia, handgrip strength, and need for nutritional intervention in cancer patients
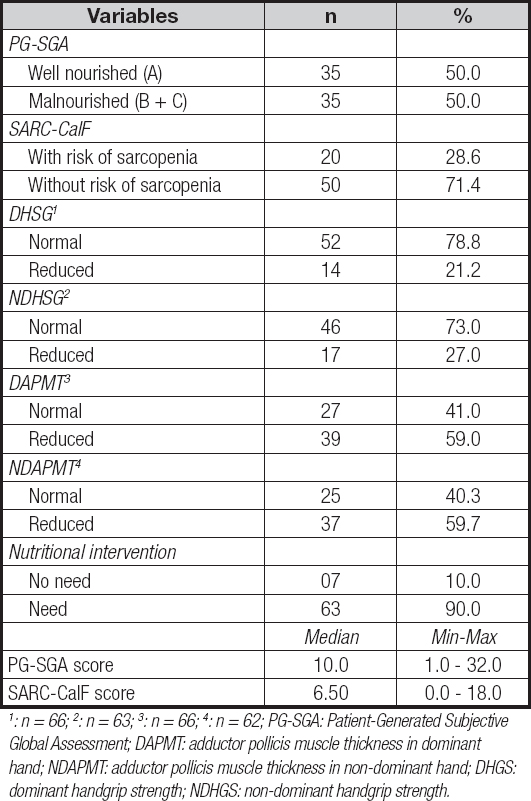
1: n = 66; 2: n = 63; 3: n = 66; 4: n = 62; PG-SGA: Patient-Generated Subjective Global Assessment; DAPMT: adductor pollicis muscle thickness in dominant hand; NDAPMT: adductor pollicis muscle thickness in non-dominant hand; DHGS: dominant handgrip strength; NDHGS: non-dominant handgrip strength.
Table III shows the correlations of the SARC-CalF score with age, anthropometric variables, and PG-SGA score according to stage of life. In adults (< 60 years) significant and moderate correlations were found between the SARC-CalF score and current weight, AC, AMC, CAMA, DAPMT, NDAPMT, DHSG, NDHSG, BMI, and PG-SGA score. In the elderly (≥ 60 years), significant and moderate correlations were observed with current weight and DAPMT.
Table III. Correlation between SARC-CalF score and age, anthropometric variables, handgrip strength, body mass index, and PG-SGA score of cancer inpatients

Sperman’s correlation. *: < 0.05; †: < 0.001; AC: arm circumference; TSF: tricipital skinfold; AMC: arm muscle circumference; CAMA: corrected arm muscle area; BMI: body mass index; DAPMT: adductor pollicis muscle thickness in dominant hand; NDAPMT: adductor pollicis muscle thickness in non-dominant hand; DHGS: dominant handgrip strength; NDHGS: non-dominant handgrip strength; PG-SGA: Patient-Generated Subjective Global Assessment.
Table IV shows the multivariate linear regression analysis considering the SARC-CalF score as dependent variable. For adults, it remained in the final AMC and DAPMT model, explaining 53.0 % of the SARC-CalF score. DAPMT was the variable that most influenced the SARC-CalF score, reducing it by 0.830 points for each mm of measurement. In the elderly, the variables current weight and DAPMT remained in the final model, explaining 38.6 % of the SARC-CalF score. DAPMT was the variable that most influenced the SARC-CalF score also in this age group, reducing it by 0.574 points for each mm of measurement.

DISCUSSION
This study showed that approximately one third of the evaluated patients were classified as being at risk for sarcopenia by the SARC-CalF tool. Cancer has been considered one of the main causes of secondary sarcopenia, associated with an increase in infectious complications, and a higher incidence of malnutrition and immunosuppression (6,8).
A study carried out with 77 individuals of both sexes, with different types of cancer, concluded that the risk of sarcopenia in this population predicts a worsening of 49.0 % in nutritional status and 29.0 % of comorbidities (21).
The presence of preoperative sarcopenia in patients with GIT cancer has been shown to be an important risk factor for postoperative complications (22). Among sarcopenic patients who underwent gastric cancer surgery, 43.8 % had postoperative complications (23). Thus, identifying pre-sarcopenia and performing an adequate, individualized nutritional management is one of the strategies that can reduce postoperative complications and negative clinical outcomes (24).
In sarcopenic patients, the amount of available amino acids is insufficient for tissue repair, which leads to delayed healing and, consequently, infectious complications (22,25). With the reduction of skeletal muscle mass and increase in adipose tissue, a process known as myosteatosis, an imbalance in the production of anti-inflammatory and pro-inflammatory cytokines is triggered, resulting in a pro-inflammatory state with weakening of the immune system (22,25).
The high prevalence of malnutrition and the need for nutritional intervention demonstrate the vulnerability of cancer patients, especially those with GIT cancer. These conditions may be related to inadequate intake and absorption of nutrients, anorexia, and other symptoms of nutritional impact, which are very common in these patients (26,27). Early diagnosis of the risk of sarcopenia and of nutritional status with appropriate tools can reduce problems and consequently improve patient prognosis.
Among the correlations we found here, it was possible to observe that the SARC-CalF score in adults was associated with HSG and most anthropometric variables, especially those indicative of muscle reserve, whereas in the elderly correlations with current weight and DATPM were detected.
After a regression analysis, AMC and ATPMD were found to be the variables that most influenced SARC-CalF score in adults. Besides being indicative of muscle mass reserve, AMC can reveal the presence of nutritional risk, as shown by previous studies in which it identified a higher percentage of malnutrition in individuals with cancer of the GIT and its attached glands (28,29).
Regardless of the stage of life, ATPMD was the variable that most influenced the SARC-CalF score, with ATPM having been identified as a promising measure, as a result of it being capable of revealing changes in body muscle composition by indicating early changes related to malnutrition and recovery of nutritional status (29-31). In this study, ATPM was associated with the SARC-CalF score, strengthening its association with the reduction of muscle mass, thus working as a predictor of sarcopenia.
Although SARC-CalF is a screening tool based on self-reporting, having been validated in the elderly population, its use proved to be viable when diagnosing the risk of sarcopenia in both adults and the elderly, as it was associated with sensitive anthropometric measures while measuring muscle mass and impaired nutritional status (12,29,32).
However, these results were not compared with advanced tests such as full-body X-ray densitometry (DEXA) or computed tomography, tests that are considered the gold standard to quantitatively and qualitatively identify changes in muscle mass (33), which limits some statements about the results.
Another limitation is the absence of tumor staging, as the hospital at which the investigation took place specializes in surgical rather than antineoplastic treatment. This fact makes this information not a priority for this type of treatment.
To our knowledge, this is the first Brazilian study that assesses risk of sarcopenia and associated factors in patients with GIT cancer. SARC-CalF was presented as an alternative, practical, and low-cost tool that can be used by health professionals to identify risk of sarcopenia in cancer patients.

