










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Excess in body weight may predispose to cardiometabolic abnormalities including diabetes, metabolic-associated fatty liver (NAFLD), and atherosclerosis (1). Adipose tissue secretes a variety of adipokines and hormones with pathophysiological role in whole-body metabolism regulation and systemic inflammation (2). Likewise, adipose tissue dysfunction is characterized by ectopic fat accumulation, increased production of pro-inflammatory adipokines (leptin, resistin, IL-1β, IL-6, and MCP-1), and decreased serum adiponectin (1-5).
Along with obesity pandemic, the rate of NAFLD has increased worldwide. While some epidemiological studies have shown that NAFLD is an independent risk factor for diabetes, other studies have shown that diabetes itself leads to advanced liver damage (5,6). The main drivers of diabetes progression are the loss of tissue insulin sensitivity, and β-cell function impairment (7). Thus, early identification and resolution of these abnormalities may help to prevent diabetes and advanced stages of liver disease.
Endothelial dysfunction is an early marker of atherosclerosis associated with obesity and diabetes. Endothelial progenitor cells (EPC), a subset of circulating bone marrow-derived cells, promote tissue regeneration after endothelial damage (8). Circulating levels of EPC are lower in patients with diabetes compared with healthy subjects (9). Moreover, in vitro studies have shown that EPC from subjects with obesity have a lower capacity of adhesion, migration, and angiogenesis, which suggest an active role of EPC on vascular dysfunction among these subjects (9,10).
Dietary counseling focused on improving diet QUALITY may preserve endothelium health and delay the onset of NAFLD and diabetes (11,12). Noteworthy, chia seed (Salvia hispanica) is the richest vegetal source of omega 3-fatty acids, antioxidants, and viscous fiber (13). Although animal models have suggested that chia could be useful to reduce ectopic fat depots and improve glycemic control (14), and we have previously reported beneficial effects of dietary chia supplementation on NAFLD (15), no study has analyzed if these improvements impact on adipose tissue function, diabetes progression, and endothelial dysfunction. Hence, the objective of the present study was to analyze the effect of an isocaloric chia-supplemented diet on adipose tissue inflammation, glucose metabolism, tttttttt-cell, and endothelial function markers in patients with NAFLD and early stages of diabetes.
MATERIALS AND METHODS
PATIENTS
Participants were selected from the control group of the Genetics of Atherosclerotic Disease study (GEA, for its acronym in Spanish). Subjects with NAFLD diagnosis confirmed by computed tomography (CT) imaging were included (16). Patients with previous diabetes diagnosis, use of glucose or lipid-lowering medications, unstable body weight (variation > 5 % within the preceding three-month period), consumption of vitamins, probiotics, herbal or food supplements were excluded. A written informed consent form prior to completing any assessment was obtained for each patient.
The experimental protocol was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki, it was approved by the Research and Ethics Committee of the Ignacio Chavez National Institute of Cardiology (INCICH) (No. 16-980) and was registered at clinical trials.gov (NCT03942822).
NUTRITIONAL INTERVENTION AND FOOD INTAKE EVALUATION
Dietary intervention has been previously detailed (15). Briefly, two weeks before starting chia supplementation, each participant was personally interviewed by a certified NUTRITIONist to design and explain the isocaloric diet to follow during the study and to standardize basal macronutrient dietary composition among patients. Twenty-eight sachets of 25 g of chia seeds were monthly provided, and patients were instructed to mill one sachet per day, underlying the relevance of consuming the milled seed from breakfast through lunch, but always before 6:00 p.m. To foster treatment adherence and record adverse events, patients were telephonically contacted once weekly during the intervention. Adherence was calculated as the median of the empty chia sachets returned, and 28 empty sachets were considered as 100 % compliance. Anthropometric, diet evaluation, laboratory test, and CT studies were made after dietary standardization (basal condition), and after eight weeks of chia supplementation. Patients were advised to maintain dietary recommendations and their usual level of physical activity throughout the study.
ANTHROPOMETRIC EVALUATION
Anthropometric measurements were obtained according to the International Society for the Advancement of Kinanthropometry (ISAK) regulations, by a certified NUTRITIONist. Weight (Soehnle Professional Design 7830, Leifheit, Nassau, Germany) and height (SECA 220 wall stadiometer, GMBH and Co. KG, Hamburg, Germany) were recorded before 8:00 a.m. in fasting conditions, and body mass index (BMI) was calculated as weight (kg)/height (m2). Waist circumference was measured with a non-stretch tape (Lufkin® W606PM 6 mm × 2 m, Zapopan, Jal. Mexico).
LABORATORY TESTS
After 10-hour fasting, venous blood was collected. Total cholesterol (TC), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-C) concentrations were determined by standard enzymatic colorimetric methods (Roche Diagnostics, Mannheim, Germany), in a Cobas c311 analyzer. To perform the oral glucose tolerance test (OGTT), subjects ingested a solution containing 75 g of dextrose, and venous samples were obtained at 0, 30, 60, 90, and 120 minutes for determination of plasma glucose (G) and plasma insulin (I). Plasma G was measured by glucose oxidase method (Roche Diagnostics, Mannheim, Germany), plasma I by a sandwich ELISA (ALPCO, New Hampshire, uSA), and free fatty acids (FFA) using an enzymatic-colorimetric assay (Wako Diagnostics, Chuo-Ku Osaka, Japan). Subjects were classified accordingly to their basal OGTT (17) as having normal glucose tolerance (normal: fasting plasma glucose [FPG] < 110 mg/dl and 2-hour post-OGTT < 140 mg/dl), pre-diabetes (pre-diabetes: FPG ≥ 110 mg/dl, but lower than 126 mg/dl and/or 2-hour post-OGTT < 200 mg/dl), or diabetes (FPG ≥ 126 mg/dl and/or 2-hour post-OGTT ≥ 200 mg/dl).
Insulin function indices and oral disposition index were calculated with the following formulas:

ADIPOKINES
Adiponectin, interleukin 6 (IL-6), interleukin 1β (IL-1β), monocyte chemoattractant protein-1 (MCP-1) and resistin were quantified by a Bio-Plex® system (Bio-Rad Inc., Hercules, CA, uSA), with intra- and inter-assay variation coefficients below 4 % and 5 %, respectively.
PLASMA TOTAL FATTY ACID (TFA) ANALYSIS
Plasma fatty acids were extracted according to Folch's method (20), and analyzed in a Shimadzu GC-8A gas chromatograph equipped with a SP2330 capillary column (25 m x 0.25 mm x 0.25) as described elsewhere (15).
COMPUTED TOMOGRAPHY
Total abdominal fat (TAF), subcutaneous abdominal fat (SAF), and visceral abdominal fat (VAF) areas were measured as previously described (21). Fatty liver was defined as a liver to spleen attenuation ratio lower than 1.0 (22). Tomographic parameters were determined in a 64-slice scanner (Somatom Cardiac Sensation 64, Forchheim, Bavaria, Germany).
ENDOTHELIAL PROGENITOR CELLS
Expression of progenitor cell markers was analyzed by flow cytometry (23). Briefly, peripheral blood mononuclear cells (PBMC) were isolated from 5 ml of peripheral blood, by gradient centrifugation with Histopaque® 10771 (Sigma-Aldrich, St Louis Missouri, uSA). The samples were adjusted to 1 x 106 PBMC and incubated with anti-CD45-PERCP, anti-KDR-APC, anti-CD34-PE, and anti-CD133-FITC during 20 minutes at room temperature. Acquisition of 250 x 103 events was done in a BD FACS® (Beckton Dickinson, New Jersey, uSA). EPC were defined as CD45dim, CD34+, KDR+, and CD133+ cells.
STATISTICAL ANALYSIS
Data are presented as mean ± standard deviation, median (interquartile range) or frequencies. Basal and post-chia comparisons among OGTT categories were made by ANOVA, Kruskal-Wallis, or Chi-squared tests, as appropriate. Chia supplementation effect was evaluated by paired Student's t or Wilcoxon matched-pairs signed-rank test, as needed. The area under the curve (AuC) was calculated according to the trapezoid method using Microsoft Excel software. p values < 0.05 were considered as statistically significant. All the analyses were performed using SPSS for Windows (version 15.0; SPSS Chicago, II, uSA).
RESULTS
Thirty-two patients with NAFLD were included (37.5 % women). The mean age of the patients was 59 ± 7.4 years, 91 % had basal BMI > 25 kg/m2, and a median adherence of 95 % (88-100 %). Although no patient had previous type 2 diabetes diagnosis, RESULTS from the OGTT showed that nine subjects (28 %) had normal fasting glucose, 17 had pre-diabetes (53 %), and six newly diagnosed diabetes (19 %).
After chia supplementation, a modest waist circumference reduction was found (Table I), and it was more evident in those patients with pre-diabetes and diabetes (normal Δwaist = 0 [-3.1 to 0.3], pre-diabetes Δwaist =-2.8 [-3.6 to -1.4] cm, diabetes Δwaist = -1.4 [-4.7 to 0.15] cm, p = 0.06). However, while patients with pre-diabetes lost mainly VAF (normal ΔVAF = 1 [-14 to 16] cm2, pre-diabetes ΔVAF = -30 [-44 to -8] cm2, diabetes ΔVAF = -12 [-27 to 6] cm2, p < 0.05), those with diabetes had higher reduction of SAF (normal ΔSAF = -20 [-37 to 8] cm2, pre-diabetes ΔSAF = -8 [-13 to 11] cm2, diabetes ΔSAF =-29 [-61 to -0.2] cm2, p = ns). Liver to spleen attenuation was also improved (Table I); 33 %, 43 % and 100 % of normal, pre-diabetes and diabetes patients showed NAFLD regression.
Table I. Clinical characteristics according to oral glucose tolerance test status.
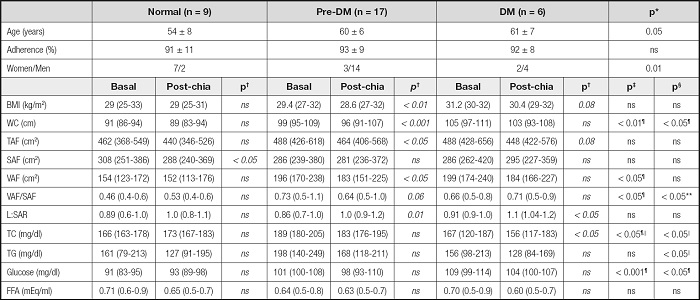
Data are expressed as mean ± standard deviation, median (interquartile range) or case number. WC: waist circumference; BMI: body mass index; TAF: total abdominal fat; SAF: subcutaneous abdominal fat; VAF: visceral abdominal fat; L:SAR: liver to spleen ratio; TC: total cholesterol; TG: triglycerides; FFA: free fatty acids.
*ANOVA or Chi-squared, as corresponds.
†Wilcoxon matched-pairs signed-rank test.
‡Kruskal-Wallis to compare basal values among groups.
§Kruskal-Wallis to compare post-chia values among groups (¶normal vs pre-DM and DM, ‖pre-DM vs DM, **normal vs pre-DM).
Overall, chia supplementation resulted in SFA, MuFA, and PuFA-omega 6 plasma concentrations reduction among patients with pre-diabetes, while PuFA-omega 3, particularly alpha linolenic acid (ALA), increased significantly in all subjects (Table II). Proportionally, ALA increase was higher for those with diabetes (normal: Δ% = 102 [68-136], pre-diabetes: Δ% = 51 [14-115], diabetes: Δ% = 121 [58-201], p = 0.06). The omega-6/omega-3 fatty acid ratio decreased significantly in all subjects, suggesting a healthier fatty acid profile after the chia intervention. As expected, fiber consumption was higher for all subjects after chia supplementation (normal: Δ% = 37 [15-72], pre-diabetes: Δ% = 82 [50-106], diabetes: Δ% = 52 [31-61], p = ns).
Table II. Dietary and plasma fatty acids composition according to oral glucose tolerance test status.
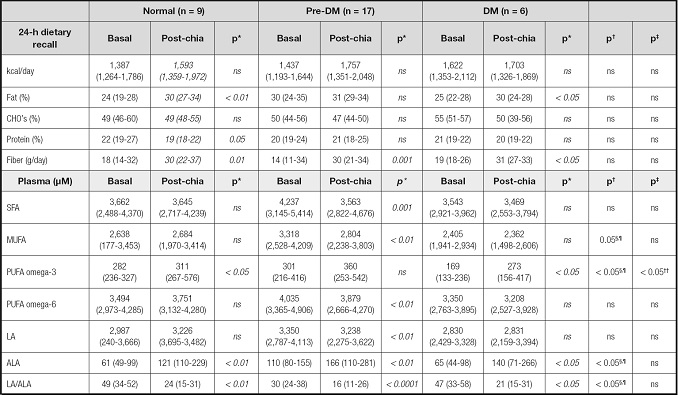
Data are expressed as median (interquartile range). CHO´s: carbohydrates; SFA: saturated fatty acids; MuFA: monounsaturated fatty acids; PuFA: polyunsaturated fatty acids; LA: linoleic acid; ALA: alpha linolenic acid.
*Wilcoxon matched-pairs signed-rank test.
†Kruskal-Wallis for basal values among groups.
‡Kruskal-Wallis for post-chia values among groups (§normal vs pre-DM and DM, ¶pre-DM vs DM, **normal vs pre-DM, ††DM vs normal and pre-DM).
An OGTT was used to assess insulin secretion/sensitivity. After chia supplementation, glucose AuC tended to decrease in all subjects. In fact, patients with diabetes showed a 17 % glucose AuC decrease (p < 0.05) (Fig. 1). Although no significant changes were found for insulin and FFA curves, or insulin resistance indices (data not shown), IGI30 and DIO increased significantly in patients with diabetes (Fig. 2).

Figure 1. Effects of chia supplementation on oral glucose tolerance test (OGTT), stratified according to basal OGTT. Normal (FPG < 110 mg/dl and/or 2-h post-OGTT < 140 mg/dl), pre-diabetes (110 mg/dl ≤ FPG ≤ 126 mg/dl and/or 140 mg/dl ≤ 2h post-OGTT < 200 mg/dl) or diabetes (FPG ≥ 126 mg/dl and/or 2-h post-OGTT ≥ 200 mg/dl). Data are expressed as median (interquartile range) and analyzed by *Wilcoxon matched-pairs signed-rank test.
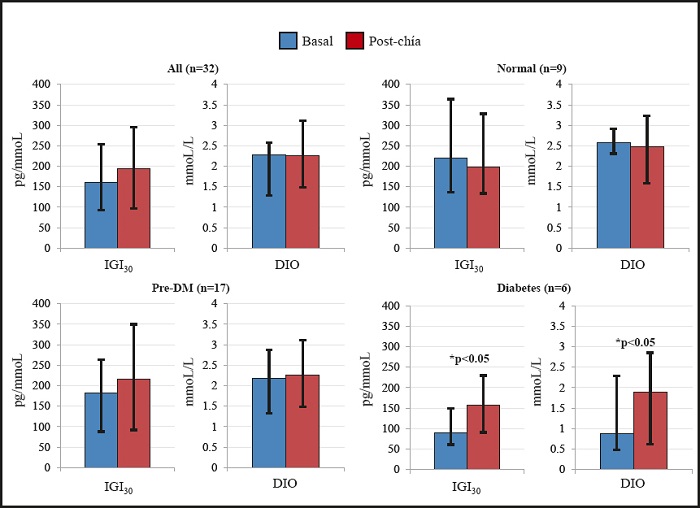
Figure 2. Effects of chia supplementation on pancreatic β cell function estimators. Data are expressed as median (interquartile range). IGI: insulinogenic index; DIO: oral disposition index. *Wilcoxon matched-pairs signed-rank test.
Figure 3 shows the effect of chia supplementation on the inflammatory profile. Overall, the data shows a significant increase on adiponectin, and reduction on resistin and MCP-1. Moreover, a decrease on IL-6 was also found in those patients with diabetes (basal 5.2 [4.1-6.4] vs post-chia 3.4 [2.0-3.8] pg/ml, p < 0.05), and IL-1β (basal 2.3 [1.6-2.9] vs post-chia 2.1 [0.9-2.2] pg/ml, p < 0.05). Progenitor endothelial cell count, which was used as a systemic indicator of endothelial function, showed significant improvements in all subjects after chia intervention (Fig. 3).
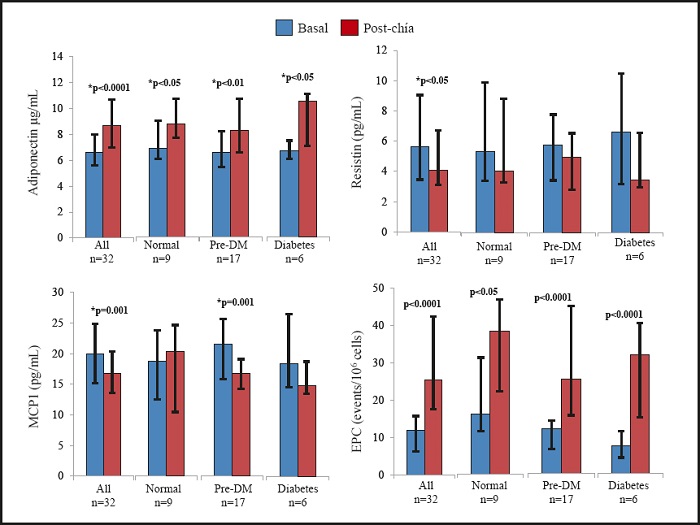
Figure 3. Effects of chia supplementation on inflammation and endothelial function markers basal post-chia. Data are expressed as median (interquartile range). For EPC, percent change for basal vs post-chia values were as follow. All: Δ% = 126 (41-264); normal: Δ% = 73 (23-212); pre-diabetes: Δ% = 108 (42-262); diabetes: Δ% = 248 (169-738). *Wilcoxon matched-pairs signed-rank test.
DISCUSSION
We have previously shown that an isocaloric supplemented diet (25 g/day of ground chia) in patients with NAFLD leads to regression of fatty liver and VAF reduction (15). The present analysis extends those findings by showing a favorable modification in plasma levels of adiponectin, resistin, and MCP-1, among NAFLD patients with early stages of glucose abnormalities. These RESULTS suggest healthier adipose tissue functionality. Chia intake also promoted a lower glucose AuC and increases in IGI30 and DIO, which suggest a better β-cell function among patients with NAFLD and newly diabetes diagnosis. Finally, the RESULTS indicate that chia supplementation could promote a better endothelial function since NAFLD patients had a higher number of EPC.
Adiponectin is secreted by healthy adipocytes and is inversely correlated to BMI, insulin sensitivity, and diabetes development (25). In prospective studies, high basal adiponectin concentrations are independently associated with preserved β-cell function (4,25), even after body weight gain and insulin resistance adjustments. Cellular and animal models have shown that adiponectin directly reduces β-cells apoptosis, lipotoxicity and inflammation, maintaining β-cell mass and function, and even promoting β-cell expansion (25).
Although controversial, a recent meta-analysis found a direct association between resistin concentrations and insulin resistance in patients with obesity and diabetes (26). In addition, a prospective study recently proposed resistin as an early independent predictor of diabetes development (5). Although the deleterious mechanism of resistin has not been completely elucidated in humans, rodent models suggest an impairment of the insulin receptor phosphorylation (27). In humans, resistin is produced by monocytes and macrophages, which could explain the link between adipose tissue inflammation and diabetes (27). Consistently, Al-Salam et al. found resistin-positive cells in normal human Langerhans islets, founding that these cells were three-times higher among patients with diabetes, suggesting that resistin may play a role in the regulation of pancreatic β-cell function (28). This evidence supports the RESULTS of the present study showing a modest reduction in BMI, along with significant reductions in resistin, MCP-1 and visceral adiposity (VAF and liver to spleen attenuation ratio), as well as an increase in adiponectin plasma levels, particularly among subjects with impaired glucose metabolism. These findings suggest that chia's beneficial effects promote a healthier adipose tissue, and ameliorate systemic inflammation in patients with NAFLD, by improving their β-cell environment and function, which consequently corrects early glucose metabolism abnormalities, as suggested by the IGI30 and DIO values.
The progressive loss of β-cell function and chronic states of insulin resistance consequently leads to the onset of type 2 diabetes. Likewise, prospective studies have shown that β-cell function impairment could be the primary determinant of incident diabetes, with a higher predictive value for diabetes progression than insulin resistance itself (6,7). Hence, health strategies to prevent diabetes should be focused on improving or delaying the impairment of β-cell function. In line with our RESULTS, a recent study in patients with obesity showed that a whole-grain enriched diet improved β-cell function and insulin secretion by increasing IGI and DIO (24). These data support the ADA recommendations (29), implying that viscous fiber intake could delay or even prevent diabetes and progression of NAFLD.
The mechanism behind viscous fiber metabolic protection is not completely understood. Vuksan et al. have shown that chia flattens glucose response by reducing glucose absorption in the first 30 minutes, delaying the maximum peak of plasma glucose and lowering glucose AUC (30).
This short-time effect is extended by this study by showing a flattened glucose response after eight weeks of chia supplementation. Rheological studies endorse chia as an excellent source of viscous fiber, by having high-water holding capacity, solubility and viscosity, and lower vulnerability to gastric acidic conditions (30). These can modify nutrient kinetics and flatten glucose response, as the present and previous studies have found.
The effect of omega 3-fatty acids on glycemic control, insulin resistance, and β-cell function is controversial (31,32). Flax is the most studied vegetal source of omega 3-fatty acids, being ALA its main fatty acid component. Although flax oil supplementation does not show an effect on plasma glucose, insulin, or hemoglobin A1c, in patients with or without diabetes, a modest improvement in β-cell function has been found in pre-diabetes after flax ingestion (33,34). The present study is in line whit the ALA protective role, since patients with diabetes had the highest increase in plasma ALA and the major reductions in glucose AuC, IGI30, and DIO, suggesting a beneficial effect of ALA on these variables. Along with previous studies, these subjects also had the higher increase in plasma adiponectin (33). These findings support that omega-3 improvements could be associated with an adiponectin increase, which in turns reflect a better adipose tissue function.
Functional foods can prevent or delay the development of diabetes and its complications. Since Mediterranean diet has shown to reduce the incidence of diabetes and mortality, the ADA recommends its use for diabetes prevention and treatment (29). The beneficial effect of this diet has been attributed to some bioactive compounds such as PuFA, flavonoids, antioxidants, and fiber (11). It is possible that chia's beneficial effect is mediated by the synergic effect of its bioactive compounds, as those proposed for the Mediterranean diet pattern (11,12).
Endothelial progenitor cells are circulating bone marrow-derived cells involved in endothelial repair (10). However, circulating levels of EPC are lower in patients with diabetes (9). Mediterranean diet has shown to significantly increase EPC number and regress atherosclerosis in patients with diabetes (10,12). Consistently, this study showed improvements in EPC after chia intake, suggesting that even without caloric restriction chia intake could improve metabolic parameters and endothelial function, leading to reduction in cardiometabolic risk.
Limitations of the present study were the small number of subjects with diabetes and the lack of a control group. Organoleptic chia properties, as well as the need to use 25 g of milled seed to have significant plasma ALA increases (15) make difficult to have an adequate placebo. Controlled studies have used a fiber source as placebo, despite that it has not been elucidated whether ALA and fiber exert independent or synergistic beneficial effects.
Chia is an accessible vegetal source of omega-3 fatty acids, antioxidants, and viscous fiber. These phytochemicals may decrease glucose AuC among patients with recent diagnosis of diabetes, decrease inflammation, and ameliorate NAFLD. Functional foods have been suggested as part of innovative therapies for the prevention of diabetes and advanced liver disease. Although findings of the present study expand this information, more studies are needed to consolidate these nutriments as a therapeutic alternative.

