










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Childhood and adolescent obesity is increasing in our country as well as in the world, and growing day by day (1). The last American National Health and Nutrition Examination Survey reported the prevalence of childhood-adolescent obesity between the ages of 2-19 as 16.3 % (2). Recently, the World Health Organization (WHO) European Regional Obesity Report 2022 showed that Turkey has a higher rate of obesity in relation to European countries (3).
Nutrition, which is among the modifiable risk factors, has an important role in the prevention of obesity in adolescents. Different dietary factors contribute negatively or positively to the development and prevention of obesity (4). Decreased adherence to the Mediterranean diet (MD), especially due to the spread of the Western style diet, is related to childhood obesity and an increase in the incidence of adult obesity and other chronic non-communicable diseases in the following years (5).
MD is frequently used to describe the traditional eating habits of societies living around the Mediterranean (6). It is a sustainable diet model in which olive oil is used as the main source of fat, and fruits, vegetables, whole grain foods, legumes and oil seeds are consumed frequently. In this diet, milk and its products, fish, poultry, and wine are moderately consumed, while red meat and its products and sugar are consumed at low levels (7). MD emphasizes the consumption of local and traditional foods suitable for lifestyle and sustainability by ensuring seasonal and nutritional diversity (8).
Consumption of plant foods, especially vegetables, fruits, and legumes, which are among the nutritional behaviors of those adopting the MD, and reducing the consumption of energy-dense foods are important dietary factors in the prevention of obesity (9). It is emphasized that increasing adherence to Mediterranean-style nutrition, especially from childhood, may reduce the risk of non-communicable chronic diseases (10). It has been reported that the MD has positive effects on body weight and health protection (11). A study conducted with adolescents on the relationship between body mass index (BMI) and MD compliance found a negative relationship (11). Also, one multicenter study covering eight European countries revealed that waist circumference was negatively associated with MD compliance (12). In addition, adherence to the Mediterranean diet is positively related to physical activity status in adolescents (13). For these reasons, evaluation of MD and adherence to the determinants of this nutritional model in earlier years of life is significant for lifestyle changes and nutritional recommendations to be developed for the implementation of a healthy nutrition model (14).
The evaluation of adherence to the MD is important in the prevention of adolescent obesity. However, it is also recommended to focus on demographic characteristics, anthropometric measurements, body composition, lifestyle habits (especially physical activity), and food and nutrient consumption that may be associated with MD compliance (15). This study aimed to evaluate the relationship between adherence to the MD and anthropometric measurements and nutritional status in adolescents.
MATERIAL AND METHODS
STUDY SETTING AND POPULATION
This cross-sectional study was conducted between November 2021 and May 2022 with middle school and high school students (mean age 14.0 ± 1.37 years) in Turkey. Children who did not have a chronic problem that affects their diet or that requires a special diet, who did not have psychological problems, who were not diagnosed with eating disorders, and who agreed to participate in the study were included in the sample. As a result of the power analysis, it was aimed to reach 1,070 individuals at 5 % type 1 error level and a confidence interval of 80 %. The data were collected through face-to-face interviews using the survey method.
Ethical permission was obtained from Erzurum Technical University Ethics Committee (20.10.2021) and Erzurum Provincial Directorate of National Education (05.11.2021). The study was carried out in accordance with the principles outlined in the Helsinki Declaration. Informed consent in written form was obtained from the parents and child assent was obtained.
MEASURES
The data collection forms included sociodemographic characteristics (age, gender, educational status of students and educational status of parents), nutritional habits, health information, physical activity status, anthropometric measurements and body composition, and 24-hour dietary recall. Energy and nutrient intakes of adolescents were evaluated using the Nutrition Information System (BeBiS) program (version 7) (16). The Mediterranean-Style Dietary Pattern Score was used to determine the degree of adherence to the Mediterranean Diet (17).
Adherence to Mediterranean diet
Adherence to the Mediterranean diet was assessed using the MSDPS and the score calculated based on the food consumption information obtained from the 24-hour dietary recall. Children's food consumption record was obtained with the help of their parents by the researchers. The MSDPS, a useful score for measuring overall diet quality according to Mediterranean diet, was developed by Rumawas et al. (2009) (17). The MSDPS was developed based on adherence to recommended intakes of 13 food groups (dairy products, fruits, vegetables, wine, whole-grain cereals, olives/legumes/nuts, fish and other seafood, poultry, meat, potatoes and other starchy roots, sweets, eggs, and olive oil) in the Mediterranean diet pyramid. In the present study, scores from only 12 groups were obtained since alcohol consumption was not asked due to adolescents' age, cultural, and religious beliefs. The score was calculated based on the recommended amounts of foods in the Mediterranean pyramid to be consumed daily or weekly. The score evaluates the negative effects of excessive consumption as well as insufficient consumption, and takes into account the foods that are not included in the Mediterranean pyramid. Except for olive oil, other MSDPS components were scored on a scale from 0 to 10. For participants whose number of consumed servings was over the recommended number, a penalty score was assigned. The aim of applying a penalty was to prevent one from attaining higher scores solely by overconsumption. Exclusive olive oil intake was scored as 10, olive oil intake besides the intake of other vegetable oils was scored as 5, and no olive oil intake was scored as 0 (17). Total MSDPS was determined by summing the 12 components of MSDPS, which were weighted in accordance with the ratio of total energy intake from the Mediterranean dietary pyramid and standardized on a 0-100 scale. All components of the MSDPS were evaluated according to intake recommendations as below the recommended intake (BRI), met the recommended intake (MRI), and exceeded the recommended intake (ERI). The calculation of the MSDPS is explained in Rumawas et al. (2009) in detail (17).
Anthropometric measurements
The researchers performed the measurements of weight and body fat (%) using a Tanita BC532 device. Waist circumference was measured at the approximate midpoint between the lower margin of the last palpable rib and the top of the iliac crest at minimum respiration with an inelastic flexible tape in a standing position (18). A stadiometer was used to measure height (18). The BMI (kg/m2) value was evaluated according to the WHO growth standards (19). BMI-for-age Z-scores were computed using the WHO AnthroPlus software (version 1.0.4, February 2011). Z-score junctions were used to categorize the measurements (19).
Physical activity
The Turkish validity and reliability study of the International Physical Activity Questionnaire-Short Form (IPAQ-SF) was conducted by Saglam et al. (2010) (20). Individuals are classified according to their physical activity level as low (< 600 MET- min/week), moderate (600-3,000 MET-min/week), and high (> 3,000 MET-min/week) (20).
STATISTICAL ANALYSIS
The Statistical Package for the Social Sciences (version 22.0) software was used for all analyses. Descriptive statistical variables (median, interquartile range [IQR] 5th-95th percentile values, mean, and standard deviation) were used to analyze the data, which was divided into four tertiles according to the MSDPS. Intergroup differences were assessed using the t-test, Mann-Whitney U test, one-way ANOVA or Kruskal-Wallis test. The relationship between the variables was evaluated using the correlation coefficient. In addition, linear regression analysis was performed for MSDPS prediction. The level of statistical significance was set at p < 0.05.
RESULTS
A total of 1,137 adolescents (45.2 % boys; 54.8 % girls; 14.0 ± 1.37 years) were included in the study. The frequency of those whose mother and father had an education period of eight years or more was found to be 58.0 %. It was revealed that 83.0 % of the adolescents skipped at least one main meal or snack (data not shown). More than half of the male students (55.1 %) were categorized as normal according to the BMI classification based on age, while 30.2 % were categorized as overweight/obese. As regards female adolescents, 46.9 % had normal BMI, while 39.5 % were considered to be overweight/obese according to the BMI classification. In addition, 20.4 % of the male students and 21.0 % of the female students were found to have low physical activity (< 600 MET-min/week). The rate of those with moderate physical activity was 55.1 % for the male students and 55.8 % for the female students (data not shown).
The median MSDPS of the adolescents was found to be 10.7 (7.7) out of a maximum possible score of 100. This score was 11.0 (7.6) for the male students and 10.6 (7.4) for the female students (p > 0.05). Among the 12 Mediterranean food groups, the median component score was the highest for olive oil consumption, followed by fruit intake. The score for fruits, vegetables, eggs, potatoes, and other starchy roots was higher in girls than boys (p < 0.05). The correlation between the total MSDPS and its components was the lowest for the consumption of fish and other seafood (correlation coefficients [r] = 0.031) and the highest for the whole grain group (correlation coefficients [r] = 0.368). The consumption of foods that are part of the Mediterranean-style dietary pattern contributed to 53.4 % of the total energy intake (Table I).
Table I. Evaluation of Mediterranean-Style Dietary Pattern Score and intake amount of its components according to gender.
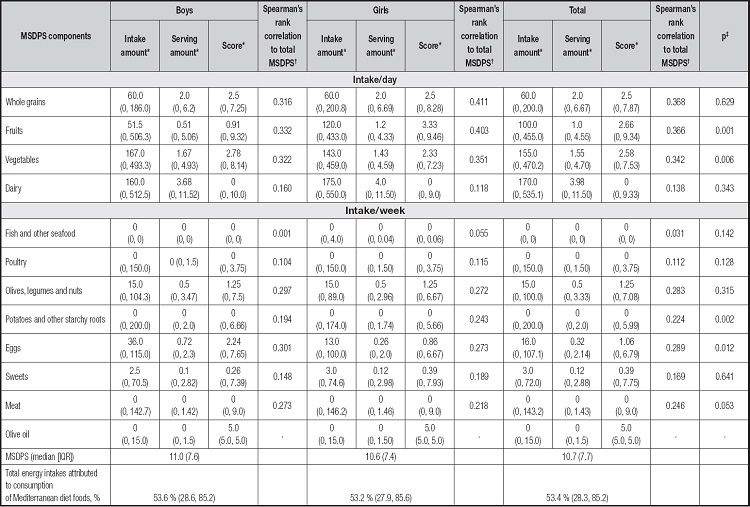
MSDPS: Mediterranean-Style Dietary Pattern Score; IQR: interquartile range.
*Data are median (5th, 95th percentiles).
†Spearman's rank correlation to total MSDPS, correlation coefficients.
‡Score differences between genders.
The "met the recommended intake" (MRI) score obtained from the MSDPS for each component was very low, and among the 12 food groups, the highest MRI score was achieved in the dairy group (male 5.8 %; female 3.5 %). For the other eleven components, the rate of "below the recommended intake" (BRI) was found to be over 80 %. The highest "exceeded the recommended intake" (ERI) score was dairy products (male 65.4 %; female 67.7 %) (Table II).
Table II. Distribution of MSDPS components according to the recommended intake.
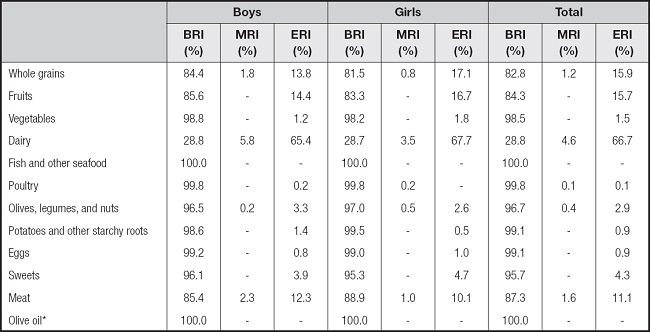
BRI: below the recommended intake; MRI: met the recommended intakes; ERI: exceeded the recommended intake.
*All participants used olive and other vegetable oils. Therefore, all participants score were "5".
Table III shows the median daily intakes of macro and micronutrients across the quartile categories of the MSDPS. While there was no difference between quartiles in terms of dietary energy, carbohydrates (CHO) and fat intakes, and vitamin E and calcium intakes in both boys and girls, the level of protein, fiber, vitamin A, vitamin C, folate, vitamin B12, iron, magnesium, zinc, and potassium intake increased with adherence to MD (p < 0.001) (Table III). A difference was observed in waist circumference in both boys and girls according to the MSDPS quartiles (p < 0.05). The majority of the underweight and overweight girls (31.5 % and 34.7 %, respectively) were in Q1 (Table IV).
Table III. Daily intakes of macro and micronutrients associated with the Mediterranean diet according to quartile categories of the MSDPS.
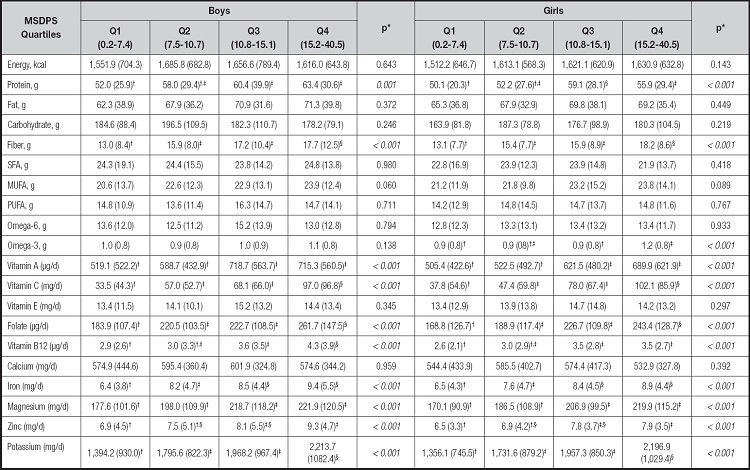
MSDPS: Mediterranean-Style Dietary Pattern Score; SFA: saturated fatty acid; MUFA: monounsaturated fatty acid; PUFA: polyunsaturated fatty acid.
*Kruskal-Wallis test.
†,‡,§The groups with the same letters within a row are not significantly different according to pairwise comparisons.
Table IV. Evaluation of adolescents demographic characteristics, obesity and physical activity status according to quartile categories of the MSDPS.
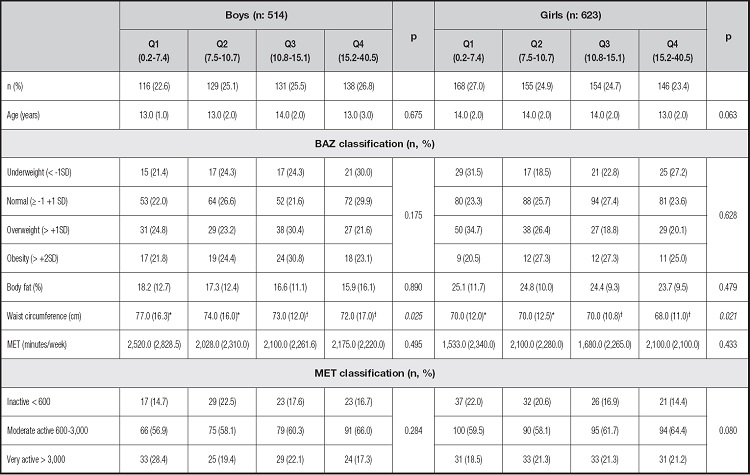
MSDPS: Mediterranean-Style Dietary Pattern Score; BAZ: BMI-for-age Z score.
*†The groups with the same letters within a row are not significantly different according to pairwise comparisons.
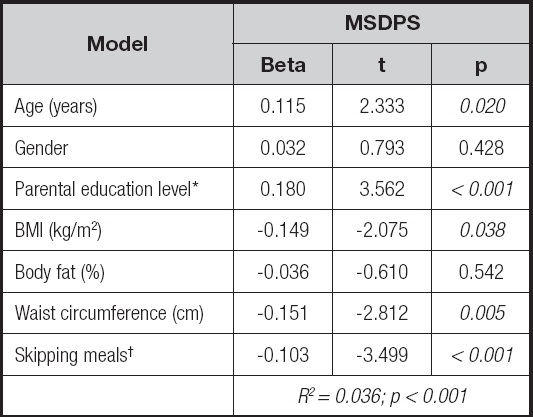
When the factors that could affect the MSDPS (age, parental education level, gender, BMI, body fat, waist circumference, skipping meals) were evaluated with regression analysis, the model was important (R2: 0.036, p < .001). It was determined that gender and body fat did not affect the MSDPS (p > 0.05), while age, parental education level, BMI, waist circumference, and skipping meals had an effect on the model (p < .05) (Table V).
DISCUSSION
In this study, the participants showed low adherence to the Mediterranean diet. The findings revealed that the older adolescents and those whose mothers had higher education and who did not skip meals were more likely to adhere to the Mediterranean diet. Also, BMI and waist circumference had a negative effect on MSDPS in regression model. Adolescents with high adherence to MD (Q4) had higher macro-micro nutrients intake levels.
MD has been accepted as a nutritional model with protective effects for childhood and adolescent obesity and related chronic diseases (10). However, the positive effects of MD on health have mostly been studied in adult population, and studies on children and adolescents are limited. In a study evaluating adherence to MD in adults in the United States, the mean MSDPS score was 24.8 (3.1-60.7) (17). The contribution of the nutrients in the MD to total energy was found to be 73.1 % (54.5-85.8), higher than the finding of our study (10.7 [7.7]) and 53.4 %, respectively (Table I). This difference may be attributed to the age difference of the sample of two studies.
One study conducted with school-aged children and adolescents in European countries with a high tendency to the MD, such as Spain, Greece, and Cyprus, found that adherence to the MD was low (21). In one study conducted with adolescents in Iran, the MSDPS score was found to be low (15.9 ± 5.6) (22). The reasons for the low MSDPS score were listed as preference for refined product consumption in the society instead of whole grain products, low levels of consumption of olive oil and fish, and fruit consumption exceeding the recommended amount (22). In this study, alcohol consumption was not evaluated in the MSDPS score due to age group, similar to the study in Iran. The low score in our study is due to the fact that whole grains, fruits, vegetables, olives, legumes and nuts, and eggs are consumed below and dairy products consumption exceeding the recommended amounts (Table II). Turkey is a Mediterranean country. However, it has undergone significant demographic and socio-economic changes in recent years, which affected dietary habits and adherence to the MD. Globalization and food advertisements also lead to changes in eating behaviors. In particular, the media and advertising sector can affect young individuals more and lead to the formation of unhealthy eating habits. Interactions between peers, especially the increasing popularity of fast-food restaurants, have a significant impact on food preferences (23).
Among the MSDPS score components, olive oil has the highest score, followed by whole-grain products. It can be said that olive oil is widely used in diets in Turkey (24). In addition, milk consumption was found to be above the recommended levels in adolescents, which negatively affected the MSDPS score. Milk consumption is encouraged within our country's scope of the School Milk Program.
The MD is rich in vitamins and minerals because it contains vegetables and fruits, whole grains, nuts, olive oil and fish, and it is stated that the risk of insufficient micronutrient intake is quite rare (25). In our study, consumption of foods that are part of the Mediterranean-style dietary pattern contributes to 53.4 % of total energy intake. The increase in adherence to MD contributes to the intake of recommended food groups and nutrients in recommended amounts. Our study revealed that the components of the MSDPS could not meet the reference intake recommendations, and among the 12 components, the consumption of dairy products was found to have the highest rate of consumption, meeting the intake recommendations. In addition, adolescents with high adherence to MD had higher protein, fiber, vitamin A, vitamin C, folate, vitamin B12, iron, magnesium, zinc, and potassium intake levels (p < 0.001). Therefore, it is important to popularize the Mediterranean-style diet model in order to meet the nutrient requirements and food group intake recommendations in the adolescence period and to ensure adequate and balanced nutrition.
Generally, young individuals are more prone to unhealthy food consumption, and as they age, they attach more importance to choosing healthier foods in order to lead a healthy life and maintain body weight (22). Some studies showed that the MSDPS score is positively associated with age (26). Similarly, our study revealed a positive relationship between age and MSDPS. People have started to eat out and tended to skip breakfast, lunch or dinner. In addition, intense and long working hours of parents, and therefore less frequent family meal times, have a significant impact on adolescents' nutritional transitions, especially on meal skipping (27). Our study also revealed that skipping meals had a negative effect on adherence to MD. The availability of healthy foods at home and habits such as eating with parents are thought to play an important role in improving the diet quality of adolescents.
MD has positive effects on body weight and health protection (28,29). Some studies conducted with adolescents on the relationship between BMI and MD compliance found a negative or no relationship (11,30). Similarly, studies investigating the relationship between MD compliance and waist circumference, which is an indicator of abdominal obesity, found different results (22,29). One multicenter study covering eight European countries revealed that waist circumference was negatively associated with MD compliance (12). Our study found that the waist circumference of girls in Q4 was lower than that of the girls in Q1 and Q2, and there was no difference between tertiles in terms of physical activity (Table IV). The majority of underweight and overweight girls had low adherence to MD. Another finding was that both BMI and waist circumference had a negative effect on the MSDPS score in the regression model (Table V). These results support that adherence to MD may contribute to the maintenance of healthy body weight. Higher adherence to the MD is generally associated with healthier food choices and healthier lifestyles, namely being physically active. Although a previous study has shown that physical activity is associated with high adherence to the MD, no effect of physical activity was found in our study (11). This may be due to the fact that the majority of the sample had moderate physical activity.
It is generally thought that individuals with a high level of education are more conscious about healthy nutrition and therefore will have a healthier diet. In addition to the environment in which people live (friends, family and school environment), easy access to information about healthy nutrition through mass media can affect nutritional behavior (26). Families also play a major role in the development of eating behaviors. It should be noted that a family member's eating behaviors are not independent of the influence of other members. As the family systems theory suggests, familial factors influence children's behaviors (31). A study shows that children of parents with a high level of education have higher adherence to the MD (32). Similar to the literature, our study revealed that high educational status of parents contributes positively to adherence to MD (Table V).
The limitation of this study was to exclude assessment alcohol due to adolescents' age, cultural, and religious beliefs.
CONCLUSION
In conclusion, adherence to MD was found to be low in adolescents. Adherence to the MD may contribute significantly to the prevention of obesity and adequate and balanced nutrition in adolescents. Since healthy eating behaviors start in childhood and adolescence, it is very important to provide healthy nutrition education for this group and to encourage adherence to MD within the scope of early intervention in obesity. Increasing adherence to MD and extending physical activity in adolescents are important for body weight maintenance and a healthier and better-quality life as well as sustainability.

