










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Stroke is currently the second leading cause of human death, and motor dysfunction after stroke is the third leading cause of disability. Stroke affects approximately 25 % of the world's population, and patients often suffer from limb dysfunction, cognitive impairment, aphasia, sensory dysfunction, dysphagia, and other complications (1). The prevalence of dysphagia in stroke patients is approximately 8.1-80 % (2). Dysphagia often leads to serious complications. Studies have found that stroke patients with dysphagia have a 4- to 13-fold increased risk of death during hospitalization (2,3). Low serum albumin level is often considered as a marker of malnutrition. Low albumin is also strongly associated with adverse outcomes and death, and is widely recognized as a strong prognostic marker for health and/or disease states (4-6). The correlation between dysphagia and serum albumin levels has not been reported. Understanding the prognostic factors affecting stroke is of great significance for determining the rehabilitation goals of patients with stroke and formulating the best treatment plan. Therefore, we aimed to conduct a retrospective analysis of 1,370 patients with stroke and explore the complex relationship between dysphagia, serum albumin levels, and prognosis during hospitalization.
MATERIAL AND METHODS
RESEARCH OBJECTIVE AND DESIGN
Our study was designed retrospectively and included stroke patients diagnosed at the Rehabilitation Department of Weifang People's Hospital, Affiliated Hospital of Weifang Medical University, and Weifang Brain Hospital from June 1, 2018, to June 1, 2022. All patients met the diagnostic criteria of the “Chinese Guidelines for Diagnosis and Treatment of Acute Ischemic stroke 2018” (7). Patients were diagnosed with stroke using computed tomography (CT) or magnetic resonance imaging (MRI), with International Classification of Diseases codes I69 or I63. The inclusion criteria were as follows: no history of dysphagia or health conditions affecting swallowing and stable vital signs. Patients with a history of transient ischemic attack and subarachnoid hemorrhage were excluded because the hemorrhage in the subarachnoid space did not result in parenchymal hemorrhage. Patients hospitalized for > 180 days and those with missing data were excluded.
RESEARCH METHOD
Data collection was conducted by five researchers who underwent unified training and pre-collection. The hospital database was searched to obtain baseline patient data, including age, sex, type of health insurance (basic medical insurance for urban residents, urban employee basic medical insurance, or self-paying), type of stroke (supratentorial, infratentorial, or supratentorial + infratentorial), site of lesion, and Charlson Comorbidity Index (CCI). The CCI is a comorbidity scoring system based on the number and severity of diseases in patients that can effectively predict the risk of death from disease and is widely used in clinical practice (8).
OUTCOME
Given that previous studies used questionnaire screening or clinical bedside swallowing assessments, the actual incidence of dysphagia may have been underestimated. Video fluoroscopic swallowing study (VFSS), the gold standard for determining dysphagia, was used in this study to ensure the accuracy of the incidence of dysphagia. Dysphagia was diagnosed when patients had difficulty swallowing fluids or food, and a VFSS confirmed dysphagia in conscious patients with stable vital signs (9).
Serum total protein concentration 24 hours after admission to the Rehabilitation Department was the primary measurement used in this study. Blood samples were collected via brachial venipuncture, centrifuged, and sent to the laboratory for analysis.
Serum albumin concentration was measured once a week, and the mean value of serum albumin during hospitalization was recorded.
Modified Rankin Scale (mRS), activities of daily living (ADL), and length of hospital stay (LOS) were recorded at discharge. The mRS measures patients' neurological recovery following stroke, with a total score of 0-5, and an mRS score ≥ 3 indicates poor functional recovery (10). ADL was assessed using a modified Barthel index (MBI) scale to assess patients' ability to perform ADL. ADL < 60 indicates that patients cannot live independently and need to rely on others (11).
STATISTICAL ANALYSIS
We built the database using Microsoft Excel (version 17.0; Microsoft, Redmond, WA), and SPSS (version 16.0; IBM, Armonk, NY, USA) was used for data analysis. If measurement data conformed to normal distribution and homogeneity of variance, the t-test was used for comparison; if there was no accordance with normal distribution, the Mann-Whitney U test was used. Enumeration data were represented by the number of cases and percentages, and preliminary crosstabs were evaluated using the Chi-squared test or Fisher's exact test. Logistic regression and multiple linear regression models were employed to analyze the correlation between dysphagia and mRS, ADL, LOS, and hypoproteinemia. Odds ratios (ORs) and corresponding 95 % confidence intervals (CIs) were calculated. To avoid the influence of insignificant independent variables on the regression equation, the stepped-multiple linear regression method was used to analyze the correlation between measurement data and dysphagia.
STANDARD PROTOCOL APPROVAL, REGISTRATION, AND PATIENT CONSENT
This study was approved by the Ethics Committee of the Weifang Medical University (2022YX056). Because the study was retrospective and the extracted data did not involve patient privacy or sensitive information, the requirement for informed consent was waived.
RESULTS
A total of 1,370 patients were included in the study after excluding those with missing data and those who did not meet the inclusion criteria. The included patients had a mean age of 59.08 ± 2.121 years and comprised 903 men (65.91 %) and 467 women (34.09 %). Among them, 610 (44.52 %) and 760 (55.48 %) had hemorrhagic stroke and ischemic stroke, respectively. Of the 1,370 patients included in the study, 499 (36.42 %) had dysphagia. There were significant differences in age, lesion location, and CCI between the patients with and without dysphagia (p < 0.05). The median length of hospitalization was 26 days. Patient characteristics are presented in table I. Figure 1 shows the distribution of serum albumin, mRS, ADL, and length of hospital stay data between the two groups.
Table I. Comparison of baseline characteristics of patients.
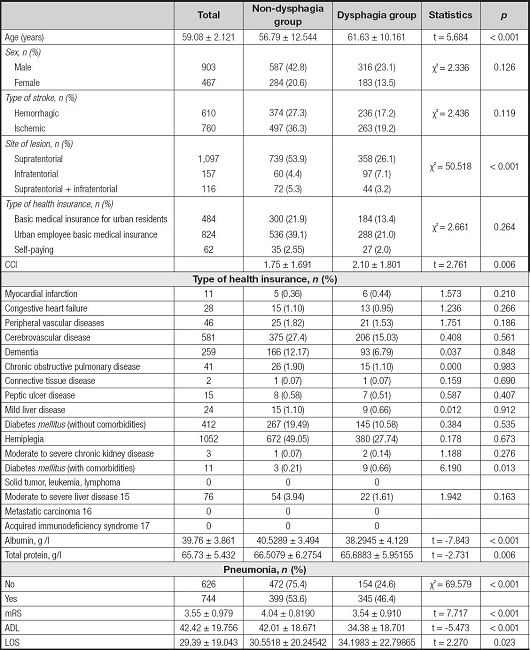
CCI: Charlson Comorbidity Index; mRS: modified Rankin scale; ADL: activities of daily living; LOS: length of stay.

Figure 1. Data distribution of serum albumin, mRS, ADL, and LOS in the dysphagia and non-dysphagia groups.
MULTIPLE LOGISTIC REGRESSION OF DYSPHAGIA WITH PNEUMONIA, PROGNOSIS, AND HYPOPROTEINEMIA
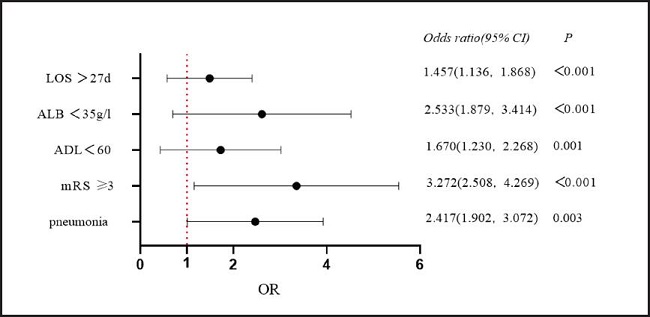
After adjusting for confounding factors, the results of the Hosmer-Lemeshow test demonstrated that the model fit well with the actual situation and accurately reflects the relationships between variables. The dysphagia group exhibited a 2.417-fold higher risk of pneumonia compared to the non-dysphagia group (OR = 2.417, 95 % CI: 1.902-3.072, p = 0.000). Moreover, at discharge, patients with dysphagia had a 3.272-fold higher risk of mRS Score ≥ 3 (OR = 3.272, 95 % CI: 2.508-4.269, p < 0.001) and a 1.670-fold higher risk of MBI < 60 (OR = 1.670, 95 % CI: 1.230-2.268, respectively; p < 0.001). Additionally, the risk of hypoproteinemia was 2.533 times higher (OR = 2.533, 95 % CI: 1.879-3.414, p = 0.000]. Furthermore, the OR for hospitalization duration > 26 days was 1.457, with a 95 % CI of 1.136-1.868 and a p-value of 0.003.
The relevant variables and their assignments in the logistic regression are outlined in table II, while specific data can be found in table III. The forest plot illustrating the OR is depicted in figure 2.
Table II. Logistic regression main variables and assignment.

CCI: Charlson Comorbidity Index; mRS: modified Rankin scale; MBI: modified Barthel index.
Table III. Multiple logistic regression of dysphagia with pneumonia, prognosis, and hypoproteinemia.
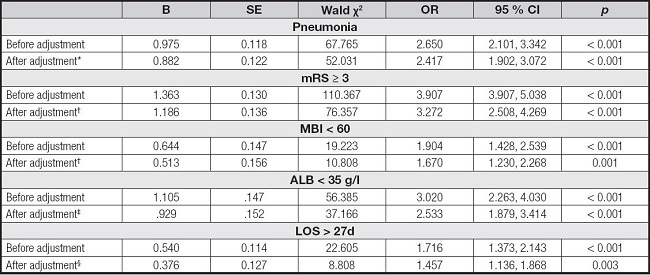
CCI: Charlson Comorbidity Index; mRS: modified Rankin scale; MBI: modified Barthel index; LOS: length of stay; ALB: albumin.
*Adjusted for confounding factors including type of stroke (hemorrhagic) and age (380~89; ≥ 90).
†Adjusted for confounding factors including type of stroke (hemorrhagic), age (80-89 years), and site of lesion (supratentorial, supratentorial + infratentorial).
‡Adjusted for confounding factors including pneumonia, age, and CCI (mild liver disease, moderate to severe chronic kidney disease, moderate to severe liver disease).
§Adjusted for confounding factors including type of stroke (hemorrhagic), age (≤ 59), and type of health insurance (self-paying).
MULTIPLE STEP LINEAR REGRESSION ANALYSIS OF DYSPHAGIA, PROGNOSIS, AND SERUM ALBUMIN
mRS, MBI, LOS, and serum albumin levels were utilized as dependent variables in the multiple stepwise regression analysis. The inclusion criteria for variables was set at p < 0.05, while the exclusion criterion was p > 0.10. Categorical variables were incorporated into the model as dummy variables. A multiple stepwise linear regression model was constructed, ensuring the absence of multicollinearity among the variables, and confirming that the residuals followed a normal distribution. Importantly, each model's multiple linear regression equations exhibited statistical significance (p < 0.001). Our results showed that dysphagia was significantly associated with a higher mRS (β = 0.265), lower ADL (β = -0.210), and longer LOS (β = 0.147, p < 0.001) (p < 0.05). When considering serum albumin as the dependent variable, the correlation coefficient was R = 0.576. Further, the coefficient of determination was R2 = 0.386, exceeding the threshold of 0.3, indicating a good fit of the model. Approximately 38.64 % of the variability in serum albumin levels could be accounted for by the variables included in the model. In addition, our results showed that dysphagia was significantly associated with lower serum albumin levels (β = -0.221, p < 0.001). In addition to dysphagia, several other factors, namely age, pneumonia, mild liver disease, moderate to severe chronic kidney disease, and moderate to severe liver disease, were identified as contributors to the variation in serum albumin levels among stroke patients. Further details are provided in table IV.
Table IV. Stepwise multiple linear regression to analyze the associations between dysphagia and mRS, ADL, and LOS in patients with stroke.
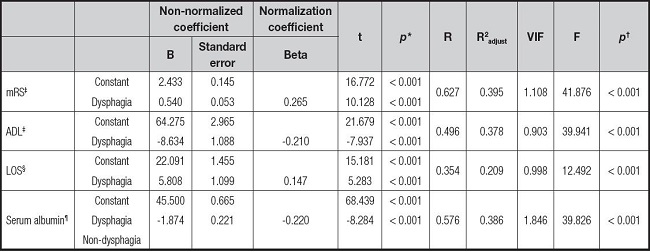
CCI: Charlson Comorbidity Index; mRS: modified Rankin scale; LOS: length of stay; ADL: activities of daily living.
*The independent variable (dysphagia) had a significant effect on the dependent variable.
†The regression equation has statistical significance.
‡Adjusted for confounding factors including type of stroke (hemorrhagic) and age (80-89; ≥ 90 years).
§Adjusted for confounding factors including type of stroke (hemorrhagic), age (80-89 years), and site of lesion (supratentorial, supratentorial + infratentorial).
¶Adjusted for confounding factors including pneumonia, age, and CCI (mild liver disease, moderate to severe chronic kidney disease, and moderate to severe liver disease).
DISCUSSION
In this retrospective study, we reported the effects of dysphagia on serum albumin levels and the prognosis of patients with stroke. Dysphagia was associated with reduced serum albumin levels, higher mRS, lower ADL, and longer LOS.
Serum albumin is a multifunctional protein with several important physiological functions. A serum albumin level < 35 mg/l has long been considered as a strong prognostic marker of health and/or disease status, and is strongly associated with short-term death in patients (12). However, little is known about the correlation between dysphagia and serum albumin levels. In this study, albumin was used as an observational indicator, and dysphagia was found to be significantly associated with decreased albumin levels. Charlson comorbidities include a total of 17 diseases. The quantification of comorbidities based on the number and severity of the disease in the patient can be used to predict the risk of death from the disease (13). Patients' CCI scores were recorded along with their comorbidities, including 17 diseases, which were incorporated into the regression analysis as dummy variables. In order to ensure the meaningfulness of each variable in the regression model and to establish the independence of the association between dysphagia and serum albumin levels from other potential factors, a stepwise multiple near linear regression method was employed.
This method involved the gradual introduction of variables one by one into the model. After introducing a new variable, the previously selected variables in the regression model were individually tested, and those found to be insignificant were eliminated. This iterative process continued until no new variables were introduced, and no existing variables were deleted, thereby ensuring the meaningful inclusion of every variable in the regression model (14).
The regression coefficient R2 in this study was 0.386, indicating that 38.6 % of the variability in serum albumin levels could be explained by the selected variables within the model. Notably, it was observed that dysphagia, age, pneumonia, mild liver disease, moderate to severe chronic kidney disease, and moderate to severe liver disease all influenced serum albumin levels in stroke patients. These factors impact albumin concentration through various mechanisms, including the absolute albumin synthesis rate, partial catabolic rate, albumin infiltration into extravascular ventricle, and exogenous albumin loss (15).
Stroke patients with dysphagia often have symptoms of choking, coughing, drooling, swallowing difficulty, and pain owing to the reduced safety and effectiveness of eating. Patients' willingness to eat is reduced, resulting in insufficient food intake. Stroke patients with swallowing disorders have a 2.425-fold increased risk of malnutrition (OR = 2.425, 95 % CI: 1.264-4.649, p < 0.05) (16-18). Albumin synthesis is associated with nutritional intake (19). When dysphagia results in a low intake of total calories and specific amino-acid reduction, liver parenchymal cells cannot obtain the required nutrients for albumin synthesis, thereby reducing albumin content in the body (4). Meanwhile, people with dysphagia can experience accidental aspiration of fluid, food, and saliva into the lungs, which increases the risk of developing pneumonia. Several studies have shown that inflammation is an important determinant of albumin concentration. When inflammation occurs, IL-6 activates C-reactive protein (CRP) and inhibits albumin synthesis, and CRP is negatively correlated with albumin levels (20,21). It is suggested that decreased serum albumin levels occur due to changes in vascular permeability induced by cytokines, leading to the diffusion of albumin into the extravascular fluid space. The above are two possible causes of reduced serum albumin caused by dysphagia.
Dysphagia also affects the prognosis of stroke patients. The MBI and mRS have been widely used in large-scale clinical trials and long-term prognostic studies of patients with stroke, and the MBI is scored based on the ability of patients to complete specific tasks in daily life (22,23). The score is positively correlated with independent ability, which can quantitatively assess the level of disability and degree of recovery of neurological function in patients with stroke (23). mRS was strongly correlated with the pathological indicators of stroke, and could reflect the differences in functional disability among patients with stroke (24). After adjusting for various confounding factors, it was observed that stroke patients with dysphagia faced a higher risk of poor functioning and dependence for ADL upon discharge from the hospital. Swallowing disorders in stroke patients can lead to inadequate food intake and increase the risk of malnutrition (16-18). Subsequently, poor nutritional status can further exacerbate the neuroinflammatory response and impede the recovery of brain injury by suppressing the expression of axonal terminal proteins (25). Furthermore, dysphagia-induced dehydration and malnutrition can contribute to muscle atrophy, compromised immune function, and overall decline in systemic function among patients. This, in turn, perpetuates a worsening cycle of patient functionality and negatively impacts prognosis (26,27).
The results of this study suggest that dysphagia and malnutrition are associated with decreased serum albumin levels and a poor prognosis. Despite the limitations and small study size, these findings further shed light on the link between dysphagia and poor prognosis. Thus, dysphagia can be used as a reference item for poor prognosis in patients with stroke. Reduced albumin levels may occur in stroke patients with dysphagia.
Several limitations of our study should be considered when interpreting our findings. A multicenter retrospective study design was not adopted, and the number of observational hospitals was insufficient. Further studies with a larger sample size should be conducted using a strict study design to improve the accuracy of the results. Therefore, our findings, especially with respect to serum albumin levels, should be carefully interpreted and treated as exploratory data.

