










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAnales de Psicología
versão On-line ISSN 1695-2294versão impressa ISSN 0212-9728
Anal. Psicol. vol.29 no.2 Murcia Mai. 2013
https://dx.doi.org/10.6018/analesps.29.2.130681
Validation of the short posttraumatic stress disorder rating interview (SPRINT-E) in a sample of people affected by F-27 Chilean earthquake and tsunami
Validación de la escala breve para diagnosticar estrés post-traumático (SPRINT-E) en una muestra de personas afectadas por el terremoto y tsunami del 27-F en Chile
Marcelo C. Leiva-Bianchi and Ismael Gallardo
Faculty of Psychology, University of Talca, Chile
ABSTRACT
On February 27, 2010 (F-27) there was an earthquake and a tsunami m Chile that has caused a great impact on the mental health of the population of this country, specifically in the increase of cases of posttraumatic stress disorder (PTSD). In view of count better instruments to measure PTSD was applied for the first time since it was created, the SPRINTE scale in a population other than the U.S., specifically in 291 people who experienced the F-27.
The analysis of reliability (α=. 916), concurrent validity (all items significantly correlated with the scale used as a criterion DTS) and construct validity (CMIN=2.237, RMSEA=.092, NFI=.901, CFI=.942 and PNFI=.704 for two-factor model) indicate that SPRINT-E is a valid and reliable scale to measure PTSD in this population.
Finally, some reflections about new factor structure discovered in this analysis, which is consistent with the meaning of items and with theoretical models such as covert stimuli. It also reflects on the usefulness of a brief scale, proven valid and very good psychometric characteristics in a Spanish-speaking population prone to natural disasters such as Chilean F-27, Japan (March 11, 2011) or Spain (May 11, 2011).
Key words: Posttraumatic stress disorder; exploratory factor analysis; confirmatory factor analysis; screening scale; earthquake; tsunami.
RESUMEN
El 27 de febrero de 2010 (27-F) se produjo un terremoto y un tsunami que ha causado alto impacto en la salud mental de la población chilena, específicamente en el aumento de los casos de estrés post-traumático (TEPT). Para contar con mejores instrumentos que midan el TEPT se aplicó, por primera vez desde que fue creada, la escala SPRINT-E en una población distinta a la estadounidense, específicamente en 291 personas que experimentaron el 27-F.
Los análisis de fiabilidad (α=.916), validez concurrente (todos los ítems correlacionan significativamente con la escala DTS utilizada como criterio) y validez de constructo (CMIN=2.237, RMSEA=.092, NFJ=.901, CFJ=.942 y PNFJ=.704 para el modelo de dos factores) indican que el SPRINT-E es una escala fiable y válida para medir TEPT en esa población.
Finalmente, se reflexiona respecto de la nueva estructura factorial descubierta en este análisis, la cual concuerda con el significado de los ítems y con modelos teóricos explicativos (estímulos encubiertos). También se reflexiona respecto de la utilidad de una escala breve, válida y de probadas muy buenas características psicométricas en una población de habla hispana propensa a catástrofes naturales como la chilena del 27-F, la japonesa del 11 de marzo de 2011, o la española del 11 de mayo de 2011.
Palabras clave: Trastorno por estés post-traumático; análisis factorial exploratorio; análisis factorial confirmatorio; escala de diagnóstico breve; terremoto; tsunami.
Introduction
On Saturday February 27th (F-27) at 03:34 (Chilean continental hour), an 8.8 Richter scale earthquake occurred. Its epicenter was located 35.909o south latitude and 72.733o west longitude, 335 kilometers to the southwest of Santiago de Chile (USGS, 2010). After the shake, a major tsunami devastated several cities and towns of at least 300 kilometers at central coast, such as Constitucion or Talcahuano (Riquelme, 2010a).
This earthquake was one of the largest and intense in the history of the planet, being one of the six most powerful movements recorded since 1900 around the world (USGS, 2011). In Chile, the sum of the consequences from the earthquake and tsunami affected nearly 80% of the population (INE, 2003), five hundred thousand homes had severe damage and left about 2 million people affected (Riquelme, 2010b). The victims were 521 people and there are 56 persons still missing (Ministerio del Interior-Gobierno de Chile, 2010a, 2010b).
Based on information giving before, we can say that an earthquake and tsunami like the F-27 are events that cause a very high impact on people, regardless their ethnicity or social income. Several studies had been showed that these events have important negative effects on health of the inhabitants of central Chile (Figueroa, Gonzalez,& Torres, 2010; Leiva, 2010; Leiva,& Quintana, 2010; Mendez, Leiva, Bustos, Ramos,& Moyano, 2010; MIDEPLAN, 2011; ONEMI, 2010). It is clear, for instance, the need for valid diagnostic tools and effective methods to quantify these effects, especially with the most important disorder after a disaster: the post-traumatic stress disorder (PTSD; Rodriguez, Zaccarelli,& Perez, 2006; Solvason, Ernst,& Roth, 2003).
Specifically the PTSD is defined by the DSM IV as a kind of anxiety disorder characterized by symptoms following exposure either directly or indirectly (hear stories, see pictures or movies) to an extremely stressful and traumatic events (in this case, the F-27). The person responds with fear, helplessness or intense horror. The traumatic event is re-experienced through rumination, uncontrollable and distressing memories or dreams, accompanied by images, thoughts or perceptions. This produces an intense psychological distress associated with continual avoidance of the experienced, dullness (reluctantly), behavioral activation and physiological responses. These responses appear especially when the person is exposed to internal or external cues that symbolize or resemble an aspect of the traumatic event. Some of the symptoms of a PTSD are related to difficulties to falling or staying asleep, to focus attention, irritability, angry outbursts, hypervigilance and exaggerated startle response. These changes may last longer than 1 month and cause clinically significant distress or impairment in social, occupational or other important areas of functioning (Lopez-Ibor, &Valdes, 2008). Note that these symptoms do not always occur immediately after a disaster. Some people affected by PTSD improve their health with time, while others may maintain the disorder for 4 years or more (Goenjian et al., 2000). In fact, in PTSD, the symptoms may appear after 6 months (Priebe et al., 2009).
In a disaster like F-27, the prevalence of the disorder in the population could be between 10% and 30% approximately (Bland et al., 2005; Bulut, 2006; Cairo, Dutta,& Nawaz, 2010; Lai, Chang, Connor, Lee,& Davidson, 2004; Sharan, Chaudhary, Kavathekar, & Saxena, 1996), same as after a political violence event (Goenjian et al., 2000). In Chile, after the F-27 the prevalence of PTSD is 12%, 6.4% for men and 14.8% for women (MIDEPLAN, 2011). In cities affected directly for the earthquake and tsunami the prevalence is around 35% (Leiva-Bianchi, 2011). Furthermore, it is expected that between 10% and 20% of health care personnel will have symptoms of PTSD and between 30% and 40% in camps of people that lost their homes after F-27 (Figueroa, Gonzalez, et al., 2010).
Davidson and colleagues (Davidson et al., 1997) proposed a scale to measure the prevalence of PTSD called "Davidson Trauma Scale" (DTS). The DTS has 17 items, related to groups of symptoms collected in the DSM-IV. For each item, people have to give two types of responses regarding frequency and intensity of these symptoms in two 5 option Likert scales. Although the DTS is widely used after traumatic events (Chen, Lin, Tang, Shen,& Lu, 2001; Davidson et al., 1997; Villafane, Milanesio, Marcellino,& Amodei, 2003), there are some problems related to the extension of the scale and the two forms of answer to each items, which could cause confusion and fatigue in people who could present PTSD.
In order to give a solution to this problem, there are screening scales that have less items and with direct method of answer. That is the case of the "Short Posttraumatic Stress Disorder Rating Interview" (SPRINTE) an instrument with 12 items, which measures the 3 groups of DSM-IV symptoms (items 1 to 4), reactions related to PTSD (5 to 11, depression, healthy behavior, stress tolerance, performance in their daily work and social functioning), the perception that each person has on needed help and suicidal intention (item 12). This last item is not included in the score but was included as a precaution: when this question is answered affirmatively, the health professionals may call for immediate referral to psychiatric services (Norris, Hamblen, Brown,& Schinka, 2008).
Respect of the measuring scale, each SPRINTE item is evaluated as experienced by the person during the last month, through a Likert scale from 0 (none) to 4 (very much) points. It is considered that a symptom is intense if this has a score of 3 or 4 (Norris et al., 2008). With the total of intense symptoms, it is used the "rule of 3/7" which states that 3 or more intense symptoms by person is very probably that he or she suffers PTSD; but with 7 or more responses the probability of a false positive (to diagnose PTSD when a person have not this disease) is very low (Norris et al., 2008).
Regarding the reliability and validity of the SPRINT-E, has been proven its predictive validity (it predicts the decrease of PTSD symptoms after treatment), concurrent validity (it is strongly correlated with the scales of Posttraumatic Stress Disorder Checklist -PCL- and the total score of the Iowa Depression Inventory) and construct validity (has only one general factor for PTSD that includes all items, except item 12; Norris et al., 2006; Norris et al., 2008). However, never before the validity of this scale (in any of its forms) has been tested in a Latin American sample, in Spanish language version, nor in people who experienced an earthquake and a tsunami. These three features constitute the main relevance of this work.
Method
Sample and procedure
The sample included 291 people, all adults of both sexes from eight different populations that lived through the F-27: 16 teachers of primary school of Constitucion city (city affected by earthquake and tsunami), 107 attorneys from the same school, 77 family health attention center workers of Constitucion city; 10 teachers of a high school of Santiago city (capitol of Chile, city affected by earthquake), 29 Education university students of a private university, 22 Education university students of a public university (both from Santiago city), and 30 Psychology university students of a University of Talca (city affected by earthquake). All these people were selected through a non-probabilistic and convenience sampling (Leon,& Montero, 2004). This is because the interest was to choose groups of people belonging to three cities affected by the F-27, although in different degrees. In addition, samples of teachers, attorneys and university students represent the general population and CESFAM staff represents a vulnerable group (Figueroa, Marin et al., 2010; Figueroa, Marin & Gonzalez, 2010).
Instruments
Short Posttraumatic Stress Disorder Rating Interview (SPRINTE): is composed by 12 items. Items 1 to 4 refer to each of the 3 groups of DSM-IV symptoms: item 1 measure the Criterion B "intrusive re-experiencing"; items 2 and 3 measure the Criterion C "Avoidance and numbing"; and item 4 measure the Criterion D "Hyperactivity". Items 5 and 7 assess other important reactions related to PTSD, such as depression and healthy behavior. Items 6, 9 and 10 refer to the functional impairment of the person, resulting in questions about stress tolerance, performance in their daily work and social functioning, respectively. Items 8 and 11 assess that each person has on need help (Norris et al., 2008) and item 12 which assess suicidal intention.
Respect of the measuring scale, each item of SPRINT-E is evaluated using a Likert scale from 0 (none) to 4 (very much) points, with the exception of item 12 (intention suicide) which is dichotomous (0 is "no" and 1 is "yes"); for this reason, item 12 was removed to the analysis. As mentioned before, the authors use it only as a criterion of gravity for the diagnosis (Norris et al., 2008).
Davidson Trauma Scale (DTS): to check concurrent validity of the SPRINT-E, DTS was applied to the same sample and at the same time as SPRINT-E. It was used an adaptation of the DTS validated for Spanish population which has good reliability index (Cronbach's Alpha over .7) and a good convergent validity (Bobes et al., 2000).
Data analysis
First, the reliability of the instrument was tested by Cronbach's Alpha for the 11 items of the SPRINT-E measured with Likert scale. For this test, a value above .9 is considered excellent (Pardo & San Martin, 1998).
Second, to determine concurrent validity Pearson correlations were conducted between the 11 items of the SPRINT-E and the 17 items of the DTS. While more items of a scale are related to each other, better will be the criterion validity of the SPRINT-E. All this correlations must be significant statistically (p<.05).
To assess construct validity, we performed an exploratory factor analysis (EFA) by the method of ungeneralized least squares extraction, varimax rotation and free numbers of factors. The EFA was performed among 144 randomly selected participants from the 291 original sample. The model has a good fit and it is relevant to perform the analysis if the following tests show values within the limits: KMO.51; Bartlett Sphericity Test with p<.01, X2 with p>.05 (Ximenez & San Martin, 2004).
Finally, to confirm the existence of the pattern obtained from the EFA, we conducted a confirmatory factor analysis (CFA) through a structural equation model with the 11 items of the SPRINT-E. CFA was performed in the sample of participants that were not used in the EFA (n=147). A model has an appropriate adjustment if the following indicators have values within the limits: CMIN<3, RMSEA<.05, NFI>.9,CFI>.9 and PNF>.05 (Barret, 2007; Hair, Anderson, Tatham,& Black, 2004).
Both, the analysis of reliability and EFA, were performed using SPSS version 15. CFA was performed using AMOS version 16.
Results
Reliability and concurrent validity
Regarding the reliability of the SPRINT-E, the test had a Cronbach Alpha value of .916 for the 11 items measured with Likert scale. Furthermore, when analyzing the values of this test if any item is deleted, the Cronbach Alpha decreases.
In relation with the concurrent validity, Pearson correlations between DTS and SPRINT-E items show that they are all highly and significantly correlated (p<.01, Table 1).
Construct validity: exploratory factor analysis
To analyze the construct validity of the instrument was performed the exploratory factor analysis (EFA). The first step was to analyze the relevance of the factor solution and if there is a structure of relations among the items suitable for extracting factors. In this regard, the Kaisser-Meyer-Olkin (KMO =.917) and Bartlett's sphericity (X2=830.455, p<.01) tests indicate that the structure of correlations was adequate and that it is appropriate to continue with the analysis.
The factor structure of the founded solution was analyzed. In this regard, we obtained a solution of 2 factors that explained 56.79% of the total variance. But this structure is different to that found by the authors of SPRINT-E above (Norris et al., 2006; Norris et al., 2008). For this reason, an EFA was performed with a single factor solution. This solution explained 48.53% of the total variance. In consequence, the evidence indicates that there are two possible models: the single general factor (Model 1) and the 2 factors model (Model 2).
Rotated factor matrix to identify which items should load on which factors was analyze, to elucidate in part this dilemma. Performing a reading of items, it is possible to group them at the same form that EFA do it: the first 4 items were related with the numbing, irritability and intrusive memories, while items 5 through 11, were related with the worry, stress and despair typical of PTSD reactions. This is consistent theoretically because is similar with the organization given by the authors of the scale (Norris et at., 2008). Therefore, the SPRINT-E would be measuring the intensity of PTSD symptoms grouped into two factors: first, related to DSM-IV symptoms of PTSD (intrusive memories, avoidance, emotional numbing and hyperarousal) and the second regarding reactions of PTSD and other health problems associated with this disorder (depression, impaired stress tolerance, impaired health behavior, bothered, impaired role functioning and impaired social functioning; see Table 2).
Construct validity: confirmatory factor analysis (CFA)
Given the above results, we conducted a CFA to specify the adjustment of Model 2 (two factors) and compare the fit with Model 1 (single factor). In both cases, maximum likelihood estimation method was used. To begin, in Model 1, all factor loadings were significant (p<.001). However, it has a regular overall fit (CMIN=2.535 and RMSEA=.103) and incremental fit (NFI=.885 and CFI=.926), although it provided a good fit of parsimony (PNFI=.708; see Figure 1).
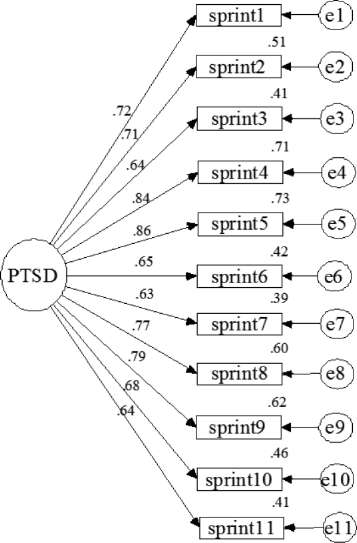
Figure 1. Standardized version of CFA for a single factor model (Model 1)
Regarding the two-factor model, all factor loadings were significant to (p<.001). This model also had a regular general fit, although slightly better than Model 1 (CMIN=2.237 and RMSEA=.092). However, both the incremental fit (NFI=.901 and CFI=.942) and the parsimony fit (PNFI=.704) are good and better than Model 1 (See Figure 2).
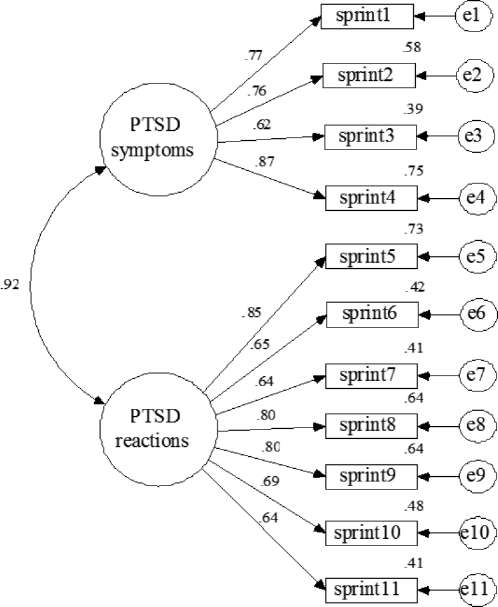
Figure 2. Standardized version of CFA for a two factors model (Model 2).
Discussion
Overall the SPRINT-E is a reliable and valid instrument for measuring the PTSD symptoms intensity. It has a very good index of internal consistency, high concurrent validity (high correlations with the DTS used as a criterion), and it has a factor structure that matches with the previous theory. It is also a brief and rapid scale that has fewer items than other scales such as the DTS. Therefore, the SPRINT-E is highly recommended to measure symptoms of PTSD in people who have experienced traumatic events as was the earthquake and tsunami of F-27 after which it was tested.
Regarding the construct validity of the SPRINT-E, the CFA shows that, although the original structure of a single factor is good, the fit is better for the two-factor model. This new model is consistent with the definition given by the authors (Norris et al., 2008) and items in this order have semantic coherence. Thus, the first 4 items are related with the PTSD symptoms (numbness, irritability and intrusive memories), while items 5 to 11 are related with responses or reactions linked to this disorder (discourage, difficulty in family and social relationships, substance abuse, difficulty solving problems and worry).
This new model can be explained from the theoretical perspective of covert conditioning, base of the therapeutic procedure known as systematic desensitization (Cautela & Kearney, 1986; Wolpe, 1958). From this perspective, PTSD is explained by covert stimulus (symptoms) that cause mal-adaptive responses (reactions). Therefore, the SPRINT-E is reproducing in its factor structure this fundamental theoretical organization. This increases its relevance as a diagnostic tool and complementary to the therapy of PTSD which, as in the case of systematic desensitization should be based on cognitive-behavioral model to be effective (Figueroa et al., 2010).
A limitation of the results just presented might be the use of maximum likelihood as a method of extraction. While this method is the most used in the CFA and provides statistical tests for the estimated parameters of the model (Martinez, Hernandez,& Hernandez, 2006), may not be the most appropriate when variables are ordinal or when they do not meet normality assumption (Brown, 2006), such as the SPRINT-E items (see Table 3). Therefore, it is best to perform the analysis with another method, such as unweighted least square (Brown, 2006). Complementary to presented results, we performed the analysis of model 2 by the latter method. The procedure gives results that confirm the good fit of model: RMR close to 0 (0.073), GFI and NFI close to 1 (.994 and .992 respectively).

Finally, the fact that the SPRINT-E has been validated for the first time in a different cultural context and after an earthquake and tsunami, is very important to implement improvements in diagnostic procedures of PTSD. Spanish version of the SPRINT-E will allow to mental health teams of the Spanish-speaking regions to have a useful and brief tool to mitigate the effects of traumatic events. For example, the SPRINT-E benefits directly to people that living in the American Pacific coast from California to Chile, susceptible population to suffer these catastrophic events, as was demonstrated after the earthquake and tsunami of Japan on March 11, 2011.The last catastrophic event not only affected the Japanese population, but also in countries such as Colombia, Ecuador, Peru and specially Chile, that suffered the effects of a massive tsunami again after just 13 months (USGS, 2011). In the Chilean case, the SPRINT-E might help to generate preventive and promotions actions for people's health, especially in coast cities, considering that the effects of a major catastrophe such as F-27 last even more than two years before occurred. Considering the situation after the earthquake of Lorca-Murcia (May 11, 2011) or others that might eventually happen in other Spanish-speaking places, can be used this scale for diagnoses and preventive purposes.
References
1. Barret, P. (2007). Structural equation modelling: Adjudging model fit. Personality and Individual Differences, 42,815-824. [ Links ]
2. Bland, S., Valoroso, L., Stranges, S., Strazzullo, P., Farinaro, E. &, Trevisan, M. (2005). Long-term follow-up of psychological distress following earthquake experiences among working Italian males: a cross-sectional analysis. Journal of Nervous and Mental Disease, 193,420-423. [ Links ]
3. Bobes, J., Calcedo-Barba, A., García, M., Francois, M., Rico-Villademoros, F., González, M.P., Bascarán, M.T., & Bousono, M. (2000). Evaluation of the psychometric properties of the Spanish version of five questionnaries for the assessment of post-traumatic stress disorders (Evaluación de las propiedades psicométricas de la version española de cinco cuestionarios para la evaluación del trastorno de estrés postraumático). Actas Españolas de Psiquiatría, 28, 207-218. [ Links ]
4. Brown, T. A. (2006). Confirmatory Factor Analysis for Applied Research. New York: Guilford Press. [ Links ]
5. Bulut, S. (2006). Comparing the earthquake exposed and non-exposed Turkish children's Post Traumatic Stress Reactions. Anales de Psicología, 22, 29-36. [ Links ]
6. Cairo, J. B., Dutta, S.,& Nawaz, H. (2010). The prevalence of posttraumatic stress disorder among adult earthquake survivors in Perú. Disaster Medicine and Public Health Preparedness, 4, 39-46. [ Links ]
7. Cautela, J.R.,& Kearney, A.J. (1986). The covert conditioning handbook. New York: Springer. [ Links ]
8. Chen, C., Lin, S., Tang, H., Shen, W.,& Lu, M. (2001). The Chinese version of the Davidson Trauma Scale: A practice test for validation. Psychiatry and Clinical Neurosciences, 55, 493-499. [ Links ]
9. Davidson, J. R. T., Book, S.W., Colket, J. T., Tupler, L. A., Roth, S., David, D., Hertzberg, M., Mellman, T., Beckham, J. C., Smith, R. D., Davison, R.M., Katz, R.,& Feldman, M. E. (1997). Assessment of a new self-rating scale for posttraumatic stress disorder. Psychological Medicine, 27, 153-160. [ Links ]
10. Figueroa, R., Gonzalez, M.,& Torres, R. (2010). Psychological response after the earthquake in Chile, on February 28, 2010 (Plan de Reconstrucción Psicológica Post Terremoto). Revista Médica de Chile, 138, 920-921. [ Links ]
11. Figueroa, R., Marin, H.,& Gonzalez, M. (2010). Psychological support for disaster victims: An evidence-based care model (Apoyo psicológico en desastres: Propuesta de un modelo de atención basado en revisiones sistemáticas y metaanálisis). Revista Médica de Chile, 138, 143-151. [ Links ]
12. Goenjian, A. K., Steinberg, A. M., Najarian, L. M., Fairbanks, L. A., Tash-jian, M.,& Pynoos, R. S. (2000). Prospective study of posttraumatic stress, anxiety, and depressive reactions after earthquake and political violence. American Journal of Psychiatry, 157,911-916. [ Links ]
13. Hair, J.F., Anderson, R.E., Tatham, R.L.,& Black, W.C. (2004). Multivariate data analysis. New Jersey: Prentice Hall International Inc. [ Links ]
14. INE-Instituto Nacional de Estadisticas (2003). Census 2002: Summary of Results (Censo 2002: Síntesis de Resultados). Santiago de Chile: La Nación S.A. [ Links ]
15. Lai, T.J., Chang, C.M., Connor, K.M., Lee, L.C.,& Davidson, J.R. (2004). Fulland partial PTSD among earthquake survivors in rural Taiwan. Journal of Psychiatric Research, 38, 313-322. [ Links ]
16. Leiva, M. (2010). Creation of an indicator of the impact of earthquake data collected from people who lived in the 27-F (Creación de un indicador de impacto de terremotos a partir de datos recogidos en personas que vivieron el 27-F). Salud & Sociedad, 1, 178-185. [ Links ]
17. Leiva, M.,& Quintana, G. (2010). Environmental and psychosocial factors associated with panic attack symptoms after the february 27, 2010 earthquake and tsunami in the central zone of Chile (Factores ambientales y psicosociales vinculados a síntomas de ataque de pánico después del terremoto y tsunami del 27 de febrero de 2010 en la zona central de Chile). Terapia Psicológica, 28, 161-167. [ Links ]
18. Leiva-Bianchi, M. (2011). The relevance and prevalence of post-traumatic stress after an earthquake: Public health problem in Constitución, Chile (Relevancia y prevalencia del estrés post-traumático post-terremoto como problema de salud pública en Constitución, Chile). Revista de Salud Pública, 13,551-559. [ Links ]
19. León, O.,& Montero, I. (2004). Research methods in psychology and education(Métodos de investigación en psicología y educación). Madrid: Mc Graw Hill. [ Links ]
20. Lopez-Ibor, J. J.,& Valdes, M. (2008). DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (DSM-IV. Manual diagnóstico y estadístico de los trastornos mentales). Madrid: Masson. [ Links ]
21. Martinez M., Hernandez, M.,& Hernandez M. (2006). Psychometrics (Psicometría). Madrid: Alianza Editorial. [ Links ]
22. McIntosh, C. (2007) Rethinking fit assessment in structural equation modelling: A commentary and elaboration on Barrett (2007). Personality and Individual Differences, 42, 859-867. [ Links ]
23. Mendez, M.D., Leiva, M., Bustos, C., Ramos, N.,& Moyano-Diaz, E. (2010). Exploratory Map of Psychosocial Interventions after the February 27 2010 Earthquake in the South-Central Zone of Chile (Mapa Exploratorio de Intervenciones Psicosociales frente al Terremoto del 27 de Febrero de 2010 en la Zona Centro-Sur de Chile.).Terapia Psicológica, 28,193-202. [ Links ]
24. Ministerio de Planificación, MIDEPLAN (2011). Post earthquake survey: Main results. Effects on quality of life of people affected by the earthquake/tsunami (Encuesta post terremoto: Principales resultados. Efectos en la calidad de vida de la población afectada por el terremoto/tsunami). Extracted January 25, 2011 from: http://www.mideplan.cl/Encuesta_Post_Terremoto.pdf [ Links ]
25. Ministerio del Interior-Gobierno de Chile (2010a). Deaths confirmed by RUT and death certificate of civil registration (updated to 15/04/2010) (Fallecidos confirmados con RUT y certificado de defunción de registro civil (actualizado al 15/04/2010)). Extracted July 14, 2010 from: http://www.interior.gov.cl/ [ Links ]
26. Ministerio del Interior-Gobierno de Chile (2010b). Unfortunately alleged complaints related to the earthquake and tsunami of 27 February (updated to 15/04/2010) (Denuncias por presunta desgracia relacionadas con el terremoto y maremoto del 27 de febrero (actualizado al 15/04/2010). Extracted July 14, 2010 from: http://www.interior.gov.cl/ [ Links ]
27. Mulaik, S. (2007). There is a place for approximate fit in structural equation modeling. Personality and Individual Differences, 42, 883-891. [ Links ]
28. Norris, F., Donahue, S., Felton, C., Watson, P., Hamblen, J.,& Marshall, R. (2006). A psychometric Analysis of Project Liberty's Adult Enhanced Services Referral Tool. Psychiatric Services, 57, 1328-1334. [ Links ]
29. Norris, F., Hamblen, J., Brown, L.,& Schinka, J. (2008). Validation of the Short Posttraumatic Stress Disorder Rating Interview (expanded version, Sprint-E) as a measure of postdisaster distress and treatment need. American Journal of Disaster Medicine, 3, 201-212. [ Links ]
30. ONEMI-Oficina Nacional de Emergencias (2010). Courses of action in response to affected areas (Cursos de acción en atención a zonas afectadas). Extracted 03 March, 2010 from http://www.onemi.cl/index.php?option=com_content&task=view&id=3816&Itemid=1969 [ Links ]
31. Pardo, A., & San Martin, R. (1998). Data analysis in psychology II. (Análisis de datos en psicología II). Madrid: Pirámide. [ Links ]
32. Priebe, S., Grappasonni, I., Mari, M., Dewey, M., Petrelli, F.,& Costa, A. (2009). Posttraumatic stress disorder six months after an earthquake. Social Psychiatry and Psychiatric Epidemiology, 44, 393-397. [ Links ]
33. Riquelme, P. (2010a, 28 de febrero). Three enormous after earthquake sea waves devastated Constitución (Tres enormes olas devastan Constitución tras sismo). La Tercera, 8-9. [ Links ]
34. Riquelme, P. (2010b, 03 de marzo). Chilean earthquake left 795 dead people and two million injured (El terremoto en Chile deja 795 muertos y dos millones de damnificados). Europapress. [ Links ]
35. Rodriguez, J., Zaccarelli, M.,& Pérez, R. (2006). Practical guide to mental health in disasters (Guía práctica de salud mental en situaciones de desastres). Washington D.C.: PAHO. [ Links ]
36. Sharan, P., Chaudhary, G., Kavathekar, S., & Saxena, S. (1996). Preliminary report of psychiatric disorders in survivors of a severe earthquake. American Journal of Psychiatry, 153,556-558. [ Links ]
37. Solvason, H.B., Ernst, H., & Roth, W. (2003). Predictors of response in anxiety disorders. Psychiatric Clinics of North America, 26, 411-433. [ Links ]
38. USGS - United States Geological Survey (2010). Tsunami and earthquake research. Extracted 14 July, 2010 from: http://walrus.wr.usgs.gov/tsunami/ [ Links ]
39. USGS - United States Geological Survey (2011). Surviving a Tsunami-Lessons from Chile, Hawaii, and Japan. Extracted 23 March, 2010 from: http://pubs.usgs.gov/circ/c1187/ [ Links ]
40. Villafañe, A., Milanesio, M.S., Marcellino, C. M.,& Amodei, C. (2003). The assessment of posttraumatic stress disorder: an approximation to the psychometric properties of the Davidson Trauma Scale. (La evaluación del trastorno por estrés postraumàtico: aproximación a las propiedades psicométricas de la escala de trauma de Davidson). Evaluar, 3, 80-93. [ Links ]
41. Wolpe, J. (1958). Reciprocal inhibition theory. Stanford: University Press. [ Links ]
42. Ximenez, C., & San Martin, R. (2004). Bases of multivariate techniques (Fundamentos de las técnicas multivariantes). Madrid: UNED Ediciones. [ Links ]
![]() Correspondence:
Correspondence:
Marcelo C. Leiva-Bianchi
Faculty of Psychology
University of Talca
Campus Lircay s/n, Talca (Chile).
E-mail: marcleiva@utalca.cl
Artículo recibido: 24-05-2011
revisado: 09-05-2012
aceptado: 10-05-2012

