










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAnales de Psicología
versión On-line ISSN 1695-2294versión impresa ISSN 0212-9728
Anal. Psicol. vol.30 no.3 Murcia oct. 2014
https://dx.doi.org/10.6018/analesps.30.3.154691
Social support and psychological well-being as possible predictors of complicated grief in a cross-section of people in mourning
Apoyo social y bienestar psicológico como posibles predictores de estado de duelo complicado en población de personas en duelo
Marta Villacieros, Inés Serrano, José-Carlos Bermejo, Marisa Magaña and Rosa Carabias
Research Center, Health Humanisation Center (Madrid, Spain)
ABSTRACT
Objective: To analyze variations in complicated grief (CG) across sociodemographic variables and variables of optimal functioning: psychological well-being (PWB), available social support (ASS) and satisfaction with available social support (SASS).
Method: A cross-sectional study was done with N = 110 people going to a free bereavement listening center (LC). They were given a questionnaire that included sociodemographic aspects. The Inventory of Complicated Grief by Prigerson (ICG), a Spanish language adaptation of Ryff's Psychological Well-Being Questionnaire and the abbreviated version of Sarason's Social Support Questionnaire (SSQSR) were used. A descriptive and correlational (Pearson) analysis was carried out. Multiple linear regression was done by using a method of a step-by-step backwards elimination.
Results: The average CG 40.91 (SD = 11.89), PWB 119.23 (SD = 18.75), ASS 10.56 (SD = 6.31) people and SASS 13.48 (SD = 4.17). The predictive variables of CG level were: PWB, ASS, SASS, months since loss, receiving pharmacological assistance and parental relationship. The adjusted R-squared was 42.4%.
Conclusions: We can consider PWB and SASS predictors of CG. It would be appropriate to clarify the effect of depressive symptoms on the perception of ASS. This study contributes to increasing efficiency of resources, to be able to partially predict CG through variables that do not involve the worsening of a mourning relative's state.
Key words: complicated Grief; bereaved; social support; satisfaction; psychological well-being.
RESUMEN
Objetivo: Analizar las variaciones en estado de duelo complicado (DC) a través de variables sociodemográficas y de funcionamiento óptimo: bienestar psicológico (BP), apoyo social disponible (ASD) y satisfacción con el apoyo social disponible (SASD).
Método: Estudio transversal, N = 110 personas que acuden a un centro gratuito de escucha de duelo (CE), a través de cuestionario que incluía aspectos sociodemográficos Inventario de Duelo Complicado de Prigerson (IDC), adaptación española del Cuestionario de Bienestar Psicológico de Ryff y versión abreviada del Cuestionario Sarason de Apoyo Social (SSQSR). Se realizó análisis descriptivo y correlacional con Pearson. Se utilizó regresión lineal múltiple por método paso a paso de eliminación hacia atrás.
Resultados: El estado medio DC 40.91 (DT = 11.89), de BP 119.23 (DT = 18.75), de ASD 10.56 (DT = 6.31) personas y SASD 13.48 (DT = 4.17). Las variables predictivas del nivel de DC fueron: BP, ASD, SASD, meses desde la pérdida, recibir ayuda farmacológica previa y parentesco progenitor. El R- cuadrado ajustado resultó de 42.4%.
Conclusiones: Podemos considerar BP y el SASD predictores del estado de DC. Sería adecuado esclarecer el efecto de sintomatología depresiva en la percepción de ASD. Este estudio contribuye a aumentar eficiencia del recurso, al poder predecir en parte el DC mediante variables que no implican deterioro del deudo.
Palabras clave: duelo Complicado; deudo; apoyo social; satisfacción; bienestar psicológico.
Introduction
The loss of a loved one is always accompanied by a subsequent period of adjustment. This is normal and is called mourning (Bermejo, 2005; Howarth, 2011). Sometimes the intensity or the course of the grieving process is altered. In this case we speak of complicated grief (Horowitz, Wilner, Marmar, & Krupnick, 1980; Simon et al., 2011; Vargas, 2003).
The process of working through grief, according to Worden (1997; 2009), includes four main tasks: I.) Accepting the reality of the loss. During the first few weeks, the prevailing emotions are confusion and bewilderment, along with denial of what has happened. One must accept that the death is real and cannot be changed. II.) Working through emotions and associated pain, i.e., feeling, expressing and talking about all of the emotions and pain that accompany the loss. III.) Adapting to changes in the environment, especially when the bereaved previously lived with the deceased on a day-to-day basis and there was a division of responsibilities / tasks and consequently, an increase in demands upon the bereaved. At this time social support is especially important. IV.) Emotionally relocating the loved one, and continuing to live, that is, accept that memories do not disappear but that the person will not return and recognize the need to redirect affection and to love again. Failure to complete these steps increases the risk of suffering from complicated grief.
In this way, the work of processing grief is directed not at the reduction of pain associated with the loss but rather, in line with what Worden suggests, to achieve an optimal level of well-being. In the literature on well-being, there is a distinction between two traditions or approaches to the concept of wellness: hedonic well-being, which includes positive feelings and emotions associated with satisfaction and pleasure, and eudaimonic well-being, focusing on optimal functioning on both the individual and social levels (Ryan & Deci, 2001). The concept of eudaimonia goes back to Aristotle, for whom the good life not so much about achieving pleasant feelings but rather realizing one's own potential (Keyes & Annas, 2009).
Ryff subscribed to this view and called it psychological well-being. He found 6 basic elements for development and empowerment of the individual: self-acceptance, positive relationships, autonomy, mastery of one's environment, having a purpose in life and experiencing personal growth (Ryff & Singer, 2008).
Self-acceptance is one of the main criteria of well-being. People should try to feel good about themselves while being aware of their own limitations. Having a positive attitude toward oneself and making a positive assessment of one's own history itself is a fundamental characteristic of positive psychological functioning (Keyes, Ryff & Shmotkin, 2002). The ability to maintain positive relationships with others is another criteria (Ryff & Singer, 1998). People need to have close, loving relationships with others, the ability to empathize, express affection and experience intimacy, they need friends whom they can trust and with whom they can work with towards achieving well-being. The ability to love is a fundamental component of well-being (Allardt, 1996) and consequently mental health (Ryff, 1989). Another key dimension is autonomy. In order to sustain their own individuality in different social settings, people need to settle into their own convictions (self-determination), and maintain independence and personal authority (Ryff and Keyes, 1995). Autonomous people can better withstand social pressure and are better at self-regulation of their behavior (Ryff & Singer, 2002). Having control of one's environment, i.e., the ability to choose or create enabling environments to meet one's own needs and desires, with the consequent sense of competence and control that it generates, is another feature of healthy functioning. People with a high mastery of their environment have a greater sense of control over the world and are able to influence the things that surround them. Finally, people need to set goals and define a set of objectives that will allow them to give their lives some meaning. They need, therefore, to have a purpose in life. Positive optimal functioning requires not only the above-mentioned traits, but one also the strength and endurance to develop one's potential, to continue growing as a person and to maximize one's capabilities (Keyes, 2003). This dimension is called personal growth.
The sphere of social relationships is presented as a relevant dimension, both in the 3rd and 4th tasks of working through grief (Worden, 1997), as is the concept of psychological well-being through positive relationships (Ryff & Keyes, 1995). Thus, social support (SS) counted on by a person in mourning, may be a matter of much importance in the early stages, of softening and cushioning the impact of the death of a loved one (damping effect), as well as in the final stages of assisting the improvement and recovery of the bereaved (recovery effect) (Lobb et al., 2010; Mancini, Prati & Bonanno, 2011; Stroebe, Wech, Stroebe & Abakoumkin, 2005).
It proves difficult to find a uniform definition of SS (Sarason, Sarason, Potter & Antoni, 1985; Sarason & Sara-son, 2009) and therefore multiple measuring instruments exist (Sarason, Sarason, Shearin & Pierce, 1987; Sherbourne & Stewart, 1991). Based on the definition of social support (SS) that Sarason (1985) offers, it consists of two basic elements: the number of people available to contact in case of need (ASS) and the degree of satisfaction with the ASS (SASS). Also from the perspective of attachment theory, SS focused on the availability of support (or available SS) despite special circumstances (Bowlby, 1982). Larger studies collect what has been defined as negative SS, or number of people who could (or who in fact do) make the bereaved angry or upset, from the size of the social network, represented in the number of people who have provided support in the past month (Burke, Neimeyer & McDevitt-Murphy, 2010; Groot & Kollen, 2013).
Scientific evidence points in different directions (Cohen & Mc.Kay, 1984) due to the different perspectives from which we have studied the relationship between SS and grief such as gender (Bankoff, 1983; Goodkin et al., 1998; Riley, LaMontagne, Hepworth & Murphy, 2007), relationship to the deceased (Bankoff, 1983; Murphy, Johnson, Chung & Beaton, 2003; Ott, 2003; Ott, Kelber & Blaylock, 2010; Riley et al., 2007;. Somhlaba & Wait, 2008; Stroebe et al., 2005), cause of death (Burke et al., 2010;. Kristensen, Weisaeth & Heir, 2010; Weder, García-Nieto & Canneti-Nisim, 2010) and symptoms present (Somhlaba & Wait, 2008; Vanderwerker & Prigerson, 2003), which have generated a wide variability in results and conclusions.
One of the first attempts to clarify the relationship between SS and psychological well-being in a sample of people in mourning was a study in the early eighties performed on a group of widows during which it was concluded that SS was helpful, harmful or neutral in terms of: 1.) the time at which it occurs during the grieving process, 2.) the type of support and 3.) the source of support (Bankoff, 1983). In this way, we distinguish three areas within the scientific literature:
The first includes studies that support the contribution of SS in decreasing the symptoms of grief: reduction of depression (Burke et al., 2010), anxiety (Somhlaba & Wait, 2008) and/or post-traumatic stress (Murphy et al., 2003; Vanderwerker & Prigerson, 2003). For example, people bereaved because of homicide (Burke et al., 2010), and bereaved mothers (Riley et al., 2007) both showed fewer symptoms associated with grief.
The second, studies that support the idea of SS and grief being independent of one another: Burke et al. (2010), while evaluating different dimensions of SS, found that neither the perceived SS in general nor the specific SS during mourning had any relation to complicated grief, nor to post-traumatic stress or depression. In the same vein, in a study of spousal bereavement of retirees, although SS was associated with a decrease in depressive symptoms, no effect or buffer was found (that decreases CG) nor recovery (an increase in well-being) by means of SS in the grieving process (Stroebe et al., 2005).
The third, those who collect evidence of the negative relationship between SS and higher levels of complicated grief: Burke et al. (2010) also found major depression and post-traumatic stress. In addition, depression was associated with the anticipation of negative SS. In this regard, two independent studies have linked a higher state of grief to a lower perception of SS (Kristensen et al., 2010; Ott, 2003).
Considering how important it is to address the functional aspects of people in vulnerable situations, the main objective of this study is to analyze the variations in the state of mourning in a sample of people grieving the loss of a loved one and try to determine whether variables such as psychological well-being and social support, essential to explaining optimal functioning, and others related to the loss, predict individual differences.
Method
Design
A correlational study with data collected between March 2010 and March 2011 through a self-reported questionnaire in a listening center (LC) or grief counseling.
The main variables of the study were state of mourning, psychological well-being and social support. State of mourning encompasses the extent to which changes could occur in the course or intensity of grief (Limonero, Lacasta, García, Maté & Prigerson, 2009). Psychological well-being, expresses the level of optimal and healthy functioning (Ryff, 1989). Social support, expressed by the available social support (ASS) and satisfaction with available social support (SASS), meaning the number of ASS people you know, excluding yourself and whom you can count on to help or support you and by SASS or the satisfaction you feel with the support you have (Sarason, 1999).
In addition, demographic variables (age and gender) were added as well as others related to the loss of the loved one (months since loss, relationship to the deceased and type of emotional bond, and assistance previously received, both psychological and pharmacological).
Participants
Participation in the questionnaires was offered to 182 grief counseling and listening center users. The center offers free help to those experiencing difficulty due to loss or for other reasons. The first contact is made via telephone by the person who wants to receive help. The LC is known as a center for all types of grief support (migratory, separation or divorce and unemployment among others) through its website, informational brochures, or word-of-mouth and is connected to a religious order. The usual format is approximately 20 sessions. It is carried out by a team of 100 volunteers with university degrees and specific qualifications obtained through courses in helping relationships, basic counseling skills, guidance and intervention in processes of grief and counseling training practices. There is evidence of similar initiatives elsewhere with satisfactory results (Altmaier, 2011; Gallagher, Tracey & Millar, 2005; Ober, Granello & Wheaton, 2012).
Of the 182 persons in mourning who had not yet started support, 130 responded, therefore the response rate was 71.42%. Males comprised 23.8% (31) and females comprised 76.2% (99). The average age was 55 years (standard deviation of 15.59, with a range of 64 years. Minimum 19, maximum 83).
Inclusion criteria were: having suffered the loss of a loved one (whether family or not), being at least 18 years of age, living in Madrid and wanting to start counseling sessions.
Instruments used
The state of grief variable was measured with the Spanish language adaptation of Prigerson's Inventory of Complicated Grief (ICG). The questionnaire consists of 19 items with good internal consistency (Cronbach's alpha coefficient = .94) and temporal stability (test - retest reliability at 6 months = 0.80). The results range from 0 to 76 points, with the highest scores corresponding to an increased likelihood of developing complicated grief (Limonero et al., 2009).
For the psychological well-being (PWB) variable the Spanish language adaptation of the Ryff Psychological Well-Being Questionnaire (Diaz et al., 2006) was used. This questionnaire consists of 29 items divided into the following Likert-type scales with response options from 1 to 6: self-acceptance, positive relationships with others, autonomy, control over one's environment, purpose in life and personal growth. The minimum total score is 29 and the highest is 174. All of the scales have good internal consistency, with Cronbach alpha values greater than or equal to .70.
To collect variables relating to social support a revised short version of the Sarason Questionnaire (Sarason, 1999) (SSQSR) was used. It assesses two dimensions of social support: first, the available support (ASS), i.e., the number of people they know and with whom they could expect to receive help or support on a scale of 0 to 9, and the other, satisfaction with available support (SASS), i.e., the degree of satisfaction felt towards the ASS with a scale of 0 to 6. The ASS score is calculated by adding the number of guests in each item, the total ranging from 3 to 27. The SASS score results from adding the scores relating to the degree of satisfaction for each of the items, the total ranging from 3 to 18. Higher scores indicate greater social support received and satisfaction with it.
The Spanish version has good internal consistency for both ASS (Cronbach's alpha = .90) and for SASS (Cronbach's alpha = .93). Temporal stability is also good with ASS (stability coefficient = .90) and SASS (stability coefficient = .83).
In addition, questions to collect information regarding age, gender, months since loss, relationship and type of bond were included. Questions such as: How long has it been since you lost your loved one? (in months), What was your relationship to the deceased? (Response options: spouse, son / daughter, father / mother, other), How wouldyou rate your relationship with your relative before he/she died? (Response options: positive, normal and negative). They were also asked about prior assistance received, both psychological and pharmacological using the following questions: Have you received counseling before now? (therapy with a psychologist or psychiatrist) (Yes / No) and Are you receiving pharmacological help? (antidepressant, ansiolytic) (Yes / no).
Procedure
Upon receiving a call from the bereaved person requesting assistance, the person in charge of making appointments assigned an identification number so that in the case of participation in the study, data collection would be anonymous.
After the first interview the person was assigned to a volunteer who had been trained in data collection. The volunteer then explained to the user the possibility of participating in the study and in the case of acceptance, the user completed the questionnaire, preferably in that first session. When the anxiety level was very high, they waited until the second or third session. When finished, the volunteer handed it to the person responsible for making appointments.
Data analysis
A descriptive analysis was used for the following variables: state of complicated grief, psychological well-being, social support, satisfaction with social support, variables related to the loss and demographic variables. The correlation between variables was examined using the Pearson correlation coefficient. For variables with more than two levels (such as relationship with the deceased and emotional bond) mean differences between groups were compared using one way Anova and after verifying homoscedasticity, multiple DHS Tukey comparisons. For two-level variables (such as gender, pharmacological and psychological assistance) Student T test for independent samples was used, establishing a confidence interval of 95%.
The possible prediction of complicated grief by the main study variables was explored using step-by-step backwards elimination multiple linear regression analysis. Using the method of least significant difference (confidence interval 95%) through mean diagrams it was analyzed which non quantitative variables were statistically significant. Prior to the multiple linear regression analysis, the hypothesis of linearity, homoscedasticity and independence were tested, being confirmed the assumption of normality a posteriori by analyzing the residuals (QQ Plot).
Having analyzed the relationships between variables and having performed simple regressions (with state of mourning as the dependent variable), it was deemed necessary to use the logarithmic transformation of the variable "months since loss" in order to meet the assumption of linearity. The SPSS version 20.0 was used.
Ethics
On the first page of the questionnaire, participants were explained who was conducting the research, the purpose of the study and how to respond. Confidentiality and adequate data protection were guaranteed as well as an explanation of usage, which was limited to research. Prior to data collection, the layout of the study was approved by the Ethics Committee of the Center.
Results
The average of the months since loss was 12.36 (SD = 19.53) in 85% of the sample (N = 110), so of the 130 participants, 20 were removed from the analysis because more than 2 years had passed since they had lost their loved ones. From the total of the selected sample (N = 110), 77.2% were women with a mean age of 54.3 years and the remaining 22.8% were men with a mean age of 55.1 years, yielding a sample mean of 55 years (SD = 15.5).
Regarding the state of complicated grief (CG) the mean was 40.91 (SD = 11.89, with a range of 59, minimum 9 and maximum 68). The internal consistency obtained through Cronbach's alpha was .794.
The average of psychological well-being (PWB) was 119.23 (SD = 18.75, range of 88, minimum 78, maximum 166). The internal consistency of the scale of psychological well-being, as measured by Cronbach's alpha was .847.
With regards to social support variables, the mean of the ASS variable was 10.56 (SD = 6.31, range 27, minimum 0 and maximum 27). With respect to satisfaction with help offered (SASS) the mean was 13.48 (SD = 4.17, range 16, minimum 2 and maximum 18). Using Cronbach's alpha an internal consistency of .796 was obtained for the scale of support received and .818 for satisfaction with support received.
The most common relationship to the deceased was spouse with 35.5% (39), second, child with 33.6% (37), then those who lost a parent with 17.3% (10) and finally 12.7% (14) lost another (brother, friend, or other).
Regarding the type of emotional bond with the deceased, 67.3% (74) reported having had a positive relationship, 26.4% (29) had a normal relationship and 5.5% (6) had a negative relationship.
Finally, in relation to prior aid received, 46.4% (51) had received counseling and 55.5% (61) had received pharmacological assistance.
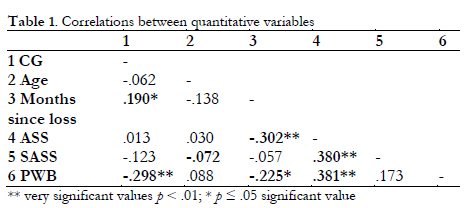
Correlations
Regarding the state of CG, we can say that there is a statistically significant inverse and moderate association between state of CG and PWB (r = - .298, p = .007), meaning that the higher the psychological well-being of the patient, the lower the level of complicated grief. There is also a slight, direct connection which is statistically significant (r = .190, p < .05) between CG and months since loss.
In relation to PWB, there is also a significant association with the number of months since loss (r = - .225, p = .045) in reverse and to a mild degree. PWB also maintains substantial direct and moderate association with ASS (r = .381, p < .000).
In turn, ASS is also associated with the variable months since loss in reverse and moderately (r = - .302, p < .001), and finally, there is a substantial direct and moderate association between ASS and SASS (r = .380, p < .000).
Predictors of Complicated Grief
The mean of CG between groups of variables was contrasted and statistically significant differences were found (p = .003) between the mean of the group who had lost a parent (M = 45.34, SD = 12.264 found) compared to those who had lost a child (M = 35.23, SD = 9.676) and between pharmacological support (p = .009) received (M = 43.59, SD = 11,805) compared to none received (M = 38.02, SD = 11,621). In all cases the assumption of variance homogeneity was met.
The rest of the categorical variables (relationship) and di-chotomous variables (gender and psychological support) did not show statistically significant differences in any of the cases to explain complicated grief.
Thus the qualitative variables that were significant in explaining differences in state of grief were the death of a parent in respect to that of a child and having received pharmacological help.
Predictive variables that ultimately became part of the equation were as follows: PWB (t = 3400, p < .01), ASS (t = 3.928,p < .000), SASS (t = 2136, p = .36), months since loss (MSL) (t = 1.975, p = .052), after receiving pharmacological assistance (PA) (t = 2419, p = .018), and parental relationship (PR) (t = - 4.176, p < .000).
The R-squared statistic indicates that the model explains 65.1% of the variability of complicated grief, adjusted R-squared (more suitable for comparing models with different numbers of independent variables) is 42.4% with an explanation of (F (6,72) = 8.845, p < .000). Finally, the following multiple linear regression model was extracted:

The analysis of these revealed that they are in accordance with normal distribution.
Discussion
The descriptive results can be translated as follows: The person asking for help in the grieving process is a woman who lost her husband or a child about a year ago. She maintained a positive bond with them and can count to least 10 people when she needs help, but the important things is that satisfaction with the people she goes to is 13.48 out of a possible 18.00 or put another way, out of a score of 100, she would be satisfied 75% of the time (75% satisfaction).
The average ASS (10.56 people) is similar to that found in Burke's study (2010) (average of 9.04), despite using a different measurement instrument, SSQSR (Sarason et al., 1987.) against ASSIS (Barrera, 1981), yet the results are comparable since both counted the number of people who provide support. The partial overlapping with Burke's et al. (2010) findings (similar mean ASS and no influence of SS on the lowering of CG) is a strong point of this study, given the rigorousness and strength of the findings in this study, which also uses a complete non-clinical sample population all mourning the death of a loved one.
Regarding the regression model, it becomes clear that the study variables which help to explain CG are: ASS, SASS, PWB, months since loss and previous pharmacological assistance received, while at the same time it is noted from the available sample that the death of a parent has relatively less impact than the death of a child or spouse. This model explains 42.4% of the variability in scores of CG. The variables which did not explain CG are: age, gender, having received previous counseling and type of emotional bond with the deceased. These are discussed below.
An inverse relationship between PWB and CG is observed. The Pearson correlation reinforces that. It is a fact fully justified by the circumstances of the study: participants were all newcomers to the LC and had not yet started the counseling sessions to help them through the mourning process, therefore, it is reasonable that having not yet completed Worden proposed tasks, they maintained high levels of grief with low PWB, especially considering that the PWB is a score that quantifies the optimal functioning of the individual dimensions of autonomy, control over one's environment, purpose in life, personal growth, etc., areas that deteriorate during bereavement, and where it is possible to recover previous levels through a proper process of working through grief.
The variables of prior pharmacological assistance received and parental relationship obtained a negative value in the regression equation, which means that if we kept all other variables fixed, by means of any of them, we get a decrease in CG. That is, we can predict that people who have had previous pharmacological help (assuming the level of the rest of the explanatory variables is constant) obtained lower scores in CG, thus the loss of the parent also predicts lower scores on the CG level compared to other relationships. In relation to pharmacological assistance and in view of the support that is provided at the LC, we recommend looking at this with caution because taking psychotropic drugs in the absence of developmental work may constitute avoidance behavior, which will decrease the symptoms but will leave the emotional work and readjustment undone (Naranjo-Vila, Gallardo-Salce & Zepeda-Santibanez, 2010).
The relationship between ASS and CG is something that stands out. As already mentioned in the introduction, the relationship of ASS regarding CG is difficult to qualify and the evidence points in different directions. In our study, holding the other explanatory variables constant, an increase in one unit of ASS predicts an increase of 0.73 units of CG. This result would place it within the third group of scientific evidence linking CG and SS, in particular the data supporting that it is negative SS which predicts an increase in CG (Burke et al., 2010). However, the measurement taken of SS, as opposed to that used by Burke to achieve that result, at any time includes negatives. Furthermore, this study highlights the direct association between ASS and SASS, which means that those who are still grieving and have a greater number of people who support them are more satisfied and those who have fewer people are less satisfied. Also, ASS and PWB maintained a direct and positive association, ie the higher the ASS, the greater the well-being. Therefore, it seems appropriate to think that despite agreement upon the end result (greater ASS predicts greater CG), ASS works differently in either study.
In turn, the SASS has a negative weight in the regression equation, which means that keeping the other variables constant, an increase in one unit of the SASS predicts a decrease of .54 units of CG. In line with the above, it would reinforce what has been said: results depend on ASS with a different valuations (positive vs. negative), and leads to the conclusion that the SS participants received was considered neither harmful nor bothersome, as was in the study of Burke et al. (2010), but rather the opposite.
This leads us to a new group of three different results already discussed in the introduction. Perhaps in our study, elevated symptoms that have been associated with grief and which are obvious to others in the form of behaviors such as crying, comments about hopelessness, etc., could be something that generates an increase in supportive behaviors and therefore greater ASS. This would have special significance to those in mourning who have already accepted the reality of their loss (Worden's 1st task) and are now dealing with the associated pain and changes in their lives that this involves (Worden's 2nd task), and above all be consistent given the study sample: people who have lost a loved one and after some time ask for outside help to work through their grief.
But there is one fact that could be interfering and which a partly similar study notes (Somhlaba & Wait, 2008): depressive symptoms caused an increased awareness of SS. Keeping this in mind, we must be cautious in our interpretation, because with this data we cannot distinguish whether a higher level of CG causes the grieving person to receive more SS, or if the person notices it because they are under the influence of depressive symptoms. It would be a question to clarify in the future for two reasons. First, because there are at least two independent studies that had the opposite result: a heightened state of CG was associated with lower perceived SS (Kristensen et al., 2010; Ott, 2003.). Second, in light of grief counseling, the overall score of the bereaved may be helped be better by knowing the real SS that they count on or if they rate it higher as a consequence of associated depressive symptomatology
Taking all of these results into account, and especially the relationship found between SS and CG, the first step in the evidence for the damping effect that SS would have on CG (Stroebe et al., 2005) could be: at first they are expressions of pain which increase social support and later on, social support influences the lowering of CG. Due to the cross-sectional design used we can only state what could be happening first. One could verify the latter using a longitudinal study.
From a broader perspective, this understanding fits the model proposed by Shah & Meeks (2012), which gives the social SS a mediating role between the above contextual factors to the loss and the end result is a resilience-CG continuum.
In relation to time since the loss of a loved one, it is noteworthy that a positive proportion in relation to CG is maintained, i.e., a positive percentage variation in the number of months since loss (logarithmic scale) predicts greater variation of CG. Intuitively, one would expect that as time passes, the discomfort decreases, a fact that even some publications support (Meert et al., 2011.); however, bearing in mind that denial is a mechanism that happens naturally and which initially is a functional aspect in the face of the progressive assimilation of the loss (Worden, 1997), it may also be an attitude that continues in some people and that could impede healthy processing of grief (Cabodevilla, 2007). From another point of view, and in line with what Worden (1997) proposes, initiating the grieving process often involves guilt, because it implies leaving the loved one behind, being aware of the disappearance of that person, and sometimes in a way that is not correctly understood, it is considered disloyal to the deceased. The guilt associated with what they are doing could cause the bereaved to halt the grieving process, and what happens is that with the passage time there is no improvement. In any case, it should be noted that the mere passage of time does not only act in favor of overcoming the loss, but rather acts against it when it does not go hand in hand with properly completing the tasks of working through one's grief.
Looking to future studies and given that there is still a significant percentage of CG to explain, it would be appropriate to include measures to collect more aspects of SS, and negative SS, and assess their differential influence as the possible moderating role of symptoms, especially the depressive type, in the perception of ASS. In addition, because the study center is linked to a religious order and helps relatives experiencing problems with processing their grief, the sample may be biased in its selection and it would be desirable to establish a comparison group with another center where grieving relatives also go and / or try to replicate the study in another center.
However, this research provides interesting suggestions in the field of grief counseling for those who have lost a loved one, especially in respect to the role of psychological well-being and social support received (valued as satisfactory) as predictors of complicated grief, and that the information provided by maintained optimal functioning and the social network that is counted on respectively open the possibility of preventing complicated grief through variables that do not involve suffering or impairment of the person, which is a desirable objective for an efficient use of the resources offered at the grief counseling center.
References
1. Allardt, E (1996). Tener, amar, ser: una alternativa al modelo sueco de investigación sobre el bienestar. En M. Nussbaum y A. Sen (comps.), La calidad de vida (pp. 126-134). México: F.C.E. [ Links ]
2. Altmaier, E. M (2011). Best practices in Counseling Grief and Loss: Finding Benefit from Trauma. Journal of Mental Health Counseling, 33(1), 33-45. [ Links ]
3. Bankoff, E. A. (1983). Social support and adaptation to widowhood. Journal of Marriage and the Family, 45(4), 827-840. [ Links ]
4. Barrera, M. (1981). Social support in the adjustment of pregnant adolescents: Assessment issues. En B.H. Gottlieb (Ed.), Social networks and social support (pp. 69-96). Beverly Hills: Sage. [ Links ]
5. Bermejo, J. C. (2005). Estoy en duelo. Madrid: PPC. [ Links ]
6. Bowlby, J. (1982). Attachment and loos: attachment (2aEd). New York: Basic Books. [ Links ]
7. Burke, L. A., Neimeyer, R. A., & McDevitt-Murphy M. E. (2010). African American homicide bereavement: aspects of social support that predict complicated grief, PTSD, and depression. Omega, 61(1), 1-24. [ Links ]
8. Cabodevilla, I. (2007). Las pérdidas y sus duelos. Anales Sistema Sanitario de Navarra, 30(3), 163-176. Recuperado de http://dialnet.unirioja.es/servlet/articulo?codigo=2516405. [ Links ]
9. Cohen, S., & McKay, G. (1984). Social support, stress and the buffering hypothesis: a theoretical analysis. En A. Baum, Taylor S. E, Singer J. E. (Eds.), Handbook of Psychology and Health (pp. 253-267). Hillsdale, NJ: Lawrence Erlbaum. [ Links ]
10. Díaz, D., Rodríguez-Carvajal, R., Blanco, A., Moreno-Jiménez, B., Gallardo, I., Valle, C. & Van Dierendonck, D. (2006). Adaptación española de las escalas de bienestar psicológico de Ryff. Psicothema, 18(3), 572-577. [ Links ]
11. Gallagher, M., Tracey, A., & Millar, R. (2005). Ex clients' evaluation of bereavement couselling in a voluntary sector agency. Psychology and Psychotherapy, 78(1), 59-76. [ Links ]
12. Goodkin, K., Feaster, D. J., Asthana, D., Blaney, N. T., Kumar, M., & Baldewicz, T. (1998). A bereavement support group intervention is longitudinally associated with salutary effects on the CD4 cell count and number of physician visits. Clinical and Diagnostic Laboratory Inmunology, 5(3), 382-91. [ Links ]
13. Groot, M., & Kollen, B. (2013) Course of bereavement over 8-10 years in first degree relatives and spouses of people who committed suicide: longitudinal community based cohort study. British Medical Journal, 347, 1-11. Doi: 10.1136/bmj.f5519. [ Links ]
14. Horowitz, M. J., Wilner, N., Marmar, C., & Krupnick, J. (1980). Pathological grief and the activation of latent self-images. American Journal of Psychiatry, 137(10), 1157-2. [ Links ]
15. Howarth, R. A. (2011). Concepts and controversies in grief and loss. Journal of Mental Health Counseling, 33(1), 4-10. [ Links ]
16. Keyes, C. L. M. (2003). The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior, 43, 207-222. [ Links ]
17. Keyes, C. L. M., & Annas J. (2009). Feeling good and functioning well: distinctive concepts in ancient philosophy and contemporary science. The Journal of Positive Psychology, 4(3), 197-201. [ Links ]
18. Keyes, C., Ryff, C., & Shmotkin, D. (2002). Optimizing well-being: the empirical encounter of two traditions. Journal of Personality and Social Psychology, 82, 1007-1022. [ Links ]
19. Kristensen, P., Weisaeth L., & Heir T. (2010). Predictors of complicated grief after a natural disaster: a population study two years after the 2004 South-East Asian tsunami. Death Studies, 34, 137-150. [ Links ]
20. Limonero, J., Lacasta M., García J., Maté, J., & Prigerson, H. (2009). Adaptación al castellano del inventario de duelo complicado. Medicina Paliativa, 16(5), 291-297. [ Links ]
21. Lobb, E. A., Kristjanson, L. J. & Aoun, S. M., Monterosso, L., Halkett, G. K. B., & Davies A. (2010). Predictors of complicated grief: a systematic review of empirical studies. Death Studies, 34, 673-698. [ Links ]
22. Mancini A. D., Prati G., & Bonanno G. A. (2011). Do shattered worldviews lead to complicated grief? Prospective and longitudinal analyses. Journal of Social and Clinical Psychology, 30 (2), 184-215. [ Links ]
23. Meert, K. L, Shear, K., Newth, C. J. L., Harrison, R., Berger, J., Zimmerman, J., Anand, K J. S., Carcillo, J., Donaldson, M. S., Dean, M., Willson, D. F., Nicholson, C. (2011). Follow-up of Complicated Crief amons Parents Eighteen Months after a Child's Death in the Pediatric Intensive Care Unit. Journal of Palliative Care, 14(2) 207-214. [ Links ]
24. Murphy, S. A., Johnson, L. C., Chung, I. J., & Beaton, R. D. (2003). The prevalence of PTSD following the violent death of a child and predictors of change 5 years later. Journal of Traumatic Stress, 16(1), 17-25. [ Links ]
25. Naranjo-Vila, C., Gallardo-Salce, M., & Zepeda-Santibáñez, M. (2010). Estilo afectivo y estilos de personalidad internamente orientados (Inward) y externamente orientados (Outward): modelo de estilos emocionales de personalidad. Revista Chilena de Neuro-Psiquiatría, 48(4), 344-355. [ Links ]
26. Ober, A. M., Granello, D. H., Wheaton, J. E. (2012). Grief Counseling: An Investigation of Counselors' Training, Experience and Competencies. Journal of Counseling & Development, April 2012 (90). [ Links ]
27. Ott, C. H. (2003). The impact of complicated grief on mental and physical health at various points in the bereavement process. Death Studies, 27, 249- 272. [ Links ]
28. Ott, C. H., Kelber S. T., & Blaylock, M. (2010). "Easing the way" for spouse caregivers of individuals with dementia. Research in Gerontological Nursing, 3(2), 89-99. [ Links ]
29. Riley, L. P., LaMontagne, L. L., Hepworth, J. T., & Murphy, B. A. (2007). Parental grief response and personal growth following the death of a child. Death Studies, 31, 277-299. [ Links ]
30. Ryan, R. M., & Deci E. L. (2001). On happines and human potentials: a review of research on hedonic and eudaimonic well- being. Annual Review of Psychology, 52, 141-166. [ Links ]
31. Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57, 1069-1081. [ Links ]
32. Ryff, C. D., & Keyes, C. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69, 719-727. [ Links ]
33. Ryff, C. D, & Singer, B. (1998). The Contours of Positive Human Health. Psychological Inquiry, 9(1), 1-28. [ Links ]
34. Ryff, C. D., & Singer, B. (2002). From social structure to biology. En C. Snyder y A. López (Eds.), Handbook of positive psychology (pp. 63-73). Londres: Oxford University Press. [ Links ]
35. Ryff, C. D, & Singer, B. (2008). Know thyself and become what you are: A eudaimonic approach to psychological well-being. Journal of Happiness Studies, 9(1), 13-39. [ Links ]
36. Sarason, I. G. (1999). El papel de las relaciones íntimas en los resultados de salud. En J. Buendía (Ed.), Familia y psicología de la salud (pp. 113-131). Madrid: Pirámide. [ Links ]
37. Sarason, I. G., & Sarason, B. R. (2009). Social support: Mapping the construct. Journal of Social and Personal Relationships, 26(1), 113-120. [ Links ]
38. Sarason, I. G., Sarason, B. R., Potter, E. H., & Antoni, M.H. (1985). Life events, social support and illness. Psychosomatic Medicine, 47, 156-163. [ Links ]
39. Sarason, I. G., Sarason, B. R., Shearin, E. N., & Pierce, G.R. (1987). A brief measure of social support: practical and theoretical implications. Journal of Social and Personal Relationships, 4(4), 497-510. [ Links ]
40. Shah, S. N., & Meeks, S. (2012). Late- life bereavement and complicated grief: A proposed comprehensive framework. Aging & Mental Health, 16(1), 39-56. [ Links ]
41. Shebourne, C. D., & Stewart, A. L. (1991). The MOS social support survey. Social Science and Medicine, 32, 705-714. [ Links ]
42. Simon, N. M., Wall, M. M., Keshaviah, A. K., Dryman, M. T., LeBlanc, N. J., & Shear M. K. (2011). Informing the symptom profile of complicated grief. Depression and Anxiety, 28, 118-126. [ Links ]
43. Somhlaba, N. Z., & Wait, J. W. (2008). Psychological adjustment to conyugal bereavement: do social networks aid coping following spousal death?. Omega, 57(4), 341-366. [ Links ]
44. Stroebe, W., Zech, E., Stroebe, M. S., & Abakoumkin, G. (2005). Does social support help in bereavement?. Journal of social and Clinical Psychology, 24(7), 1030-1050. [ Links ]
45. Vanderwerker, L.C., & Prigerson, H. G.(2003). Social support and technological connectedness as protective factors in bereavement. Journal of Loss and Trauma, 9, 45-57. [ Links ]
46. Vargas, R. E. (2003). Duelo y pérdida. Medicina Legal Costa Rica, 20(2), 47-52. [ Links ]
47. Weder, N., García-Nieto, R., & Canneti-Nisim, D. (2010). Peace, reconciliation and tolerance in the Middle East. International Journal of Mental Health, 39(4), 59-81. [ Links ]
48. Worden, W. J. (1997). El tratamiento del duelo: asesoramiento psicológico y terapia. Barcelona: Paidós. [ Links ]
49. Worden, W. J. (2009). Grief counseling and grief therapy: A handbook for the mental health parctitioner. New York, NY: Springer. [ Links ]
![]() Correspondence:
Correspondence:
Marta Villacieros Durban
Research Center
Centro de Humanización de la Salud
Calle Sector Escultores, 39. Tres Cantos
28760 Madrid (Spain)
Email: investigacion@humanizar.es
Article received: 20-6-2012
Revision received: 23-10-2013
Accepted: 4-4-2014

