










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Early Intervention (EI) in Spain is a relatively young discipline. EI started its activities in the 70s, as a purely rehabilitative intervention focused on the child (Giné, García-Dié, Gràcia & Vilaseca, 2005). In the year 2000, a group of professionals from different disciplines and regions of Spain published, with institutional support, the White Book of the EI (GAT, 2000). This book contains basic principles and unifies criteria in order to facilitate higher quality care. The document assumes the importance of the family and defends that all actions and interventions must consider not only the child, but also the family and its environment. It advocates for close collaboration of social, health and educational services and for the implementation of primary, secondary and tertiary prevention actions in relation to the care of children with EI needs (GAT, 2000). However, it defends the importance of Child Development Centres and EI, to which the child should go on an outpatient basis to receive treatments.
The work philosophy proposed by the White Book of the EI is applied in different ways in each Autonomic Community of the country. This is due to the lack of specific and unique state regulations of the Spanish government. According to the study carried out by the same group that published the White Book, ten years after its publication, important differences are observed in the implementation of EI at national level. There are big differences in the professionals that are part of the teams; times of intervention directed to the child, family and environment, or they are not even always contemplated; differences in the compartmentalization of resources; autonomy of the centres; and availability of resources, especially in rural areas (GAT, 2011). In most of the services the intervention continues focused on the child, organized as outpatient sessions, although there may be a greater or lesser effort on orienting the families. Statistics of this study show, that, in average, 65.88 % of the intervention time is dedicated to the child; only 13 % is directed to the family and even less than 4.83 % to other environments.
This organization of the EI in Spain is in accordance with what we found in other European countries. A study about the situation of the EI in 19 European countries, reflected differences conditioned by the socioeconomic and cultural characteristics of the different countries. (European Agency for Development in Special Needs Education, 2005). For example, EI was offered to children up to 3 or 6 years old, depending on the age of beginning of the compulsory education. In most of the countries, direct attention was given to the child. Support for the family was an intervention on a secondary level, with the exception of Portugal and England, which declared prioritizing work with the family. Similarities were also found in some aspects. For example, all countries highlighted that parents could choose the centre to attend. However, in practice, the possibility of choice ended up being very limited due to the limited availability of vacancies and the tendency to centralize services in metropolitan areas, in decrement of rural ones.
Professional teams are of a multidisciplinary nature in all countries and the coordination and participation of health and education services usually fails.
The same European agency, five years later, conducted a follow-up study of EI practices (European Agency for Development in Special Needs Education, 2010). Advances were found in the implementation of family-centred practices in some countries such as Germany, England or Norway. In these countries, it was appreciated that work with parents had become more active. Families were involved in making decisions related with their children, observing improvements in information and counselling practices for families, training of the parents, participation in sessions focused on children, consensus on intervention objectives, etc. However, the report also reflects that in many countries, it is still necessary to continue raising awareness among professionals in order to involve parents more actively in the EI process (European Agency for Development in Special Needs Education, 2010). Spain is one of those countries where it is still necessary to improve in this aspect. An appreciation in which publications both inside and outside of Spain coincide (Castellanos, García Sánchez, Mendieta, Gómez López & Rico, 2003, García-Sánchez, 2002, García-Sánchez, Escorcia-Mora, Sánchez-López, Orcajada & Hernández-Pérez , 2014, Gine, Gràcia, Vilaseca & García-Díe, 2006, Giné, Balcells & Mas, 2010, Gutiez, 2010, Perpiñan, 2009).
Nowadays, international organizations such as the World Health Organization (WHO, 2012), the United Nations Educational, Scientific and Cultural Organization (UNESCO, 2015), the Division for Early Childhood of the Council for Exceptional Children (DEC, 2014), as specialized professional associations such as the European Association on Early Childhood Intervention (http://www.eurlyaid.eu) and the International Society on Early Intervention (http://depts.washington.edu/isei/), make a unanimously call to incorporate evidence-based and family-focused practices in EI. Practices that help improve the quality of life of families with children with disabilities. They consider that it is necessary to provide integrated interventions, supports and special services, always using models of consultation and collaboration between professionals and families (Jayaraman, Marvin, Knoche & Bainter, 2015).
There is no doubt that in order to develop an EI family-centred practices, a close relationship should be established between the members of the child-family-professional triad. The quality of the intervention will be clearly affected by the quality of the relationships that are established. Meta-analysis carried out by Dunst, Triviette & Hamby (2007), in which presence of two types of indicators in the EI professional practices, was evaluated: a) relational, which include behaviours associated with good clinical practice (compassion, empathy and active listening, etc.) and with the functions of the professional in the acquisition of competences, strengths and capabilities of the members of the family and b) participatory, where practices aimed at encouraging participation of family members in decision-making are contemplated; the use of their own skills and the development of new skills to obtain the desired resources; and collaboration with the professional as basis to enable skills and capabilities in the family. These two indicators will undoubtedly mark the whole process of intervention and its success.
In the same way, numerous studies have highlighted the importance of the relationships established between parents and professionals (Bailey, Raspa & Fox, 2012, Blue-Banning, Summer, Frankland, Nelson & Beegle, 2004, Dunst, 2000, 2005, 2006, Dunst & Triviette, 2009, Guralnick, 2005, 2011, MacKean Thurston & Scott, 2005, Mahoney & Nam, 2011, Pretis, 2005, 2012, Turnbull, Turnbull & Kyzar, 2009, among others). All of them highlight a series of aspects and principles that must be taken into account, when establishing positive relationships that facilitate intervention processes. Turnbull et al. (2009), for example, taking up results from the Blue-Banning et al. (2004) study, summarizes a series of elements that should be present in the cooperation agreements between parents and professionals: professional skills, communication, respect, commitment, equity and trust.
It is appropriate to highlight that communication plays a fundamental role in the construction of effective collaboration and the establishment of relationships between professionals and families. This communication is characterized by openness, relevance, effective use of silence and an ability to adapt to meet the needs of the other (Friend & Cook, 2010). The way in which information is transmitted also influences it. According to McWilliam (2012), communication is a reciprocal and transactional process, of conversational interaction, in which both the speaker and the listener send and receive messages through verbal and non-verbal means.
In Spain, in the last five years, actions are being initiated to incorporate practices centered on the family in EI. Thus, it is interesting to know how the different agents involved are really interacting, to what extent relational and participatory practices are being carried out, and how the information is being transmitted to the family. Answering these questions will help us to understand how professional practices are developing and to identify possibilities for improvement.
Recently, a questionnaire on styles of interaction between parents and professionals in EI (EIPPAT) (Escorcia-Mora, García-Sánchez, Sánchez-López and Hernández-Pérez, 2016) has been developed in Spain. It is an instrument designed to identify the degree of implementation of different actions, practices and interaction styles, carried out by the EI professional to guide families (relational and participatory practices). In the present study, we present the results of its application in the southeastern regions of Spain
Methods
Participants
A total of 504 families and 187 professionals participated in the study, voluntarily and anonymously. Both groups came from 28 EI centers in the Autonomous Communities of Valencia and Murcia, located in the SE of Spain.
The 504 main caregivers had an average age of 36.46 years (SD = 5.72), 100 were men (19.8%) and 404 women (80.2%). The majority were mothers 392, (77.8%), although 100 parents (19.8%) and 8 grandmothers (1.6%) also participated. Its sociodemographic characteristics are detailed in Table 1. The characteristics of the children with TA needs that these primary caregivers were in charge of are summarized in Table 2.


187 EI professionals participated in the study. They had an average age of 36.9 years and a professional experience range between 2 and 12 years in 68.5% of the cases. 74.3% of these professionals were women and 70.7% had master studies or specialization in EI. Other sociodemographic details of these professionals are summarized in Table 3.

Procedure
We contacted by postal mail with the Technical Direction of each service, asking their collaboration for the study. The objectives of the study were informed; questionnaires and instructions for their completion were presented. After that, a follow-up was done by mail and telephone to solve doubts and facilitate participation.
The directors of each centre were in charge of delivering questionnaires to service professionals, centralizing the collection of questionnaires and sending them to the research team. On their behalf, each professional offered families the opportunity to participate in the study. Families that wanted to participate filled in the questionnaire and returned it in a sealed envelope.
Data analysis
The data were analysed both descriptively, through the analysis of means and standard deviations, and inferential. For the analysis of differences between means the t-Student test was used for independent samples, the Cohen d statistic was calculated to determine the size of the effect. The SPSS program, version 20.0, was used for the statistical analysis of the data.
Instrument
The Styles Questionnaire of Interaction between Parents and Professionals in Early Intervention (SIPPEI), in both versions (primary caregiver and professional), was designed specifically for research. For its design, a rigorous process was followed in which focal discussion groups, expert judgment and a pilot application of the instrument were used. All this, for the preparation of different items, its purification and content validation. (Escorcia et al., 2016).
It consists of 42 items with five response options linked to a time criterion (1-Never, 2-Almost never, 3-Sometimes, 4-Almost always, 5-Always) and two open items. These items assess four dimensions on the relationships established between professionals and family in EI: (I) Actions carried out to give orientations (8 items plus 1 open); (II) Difficulties to follow the guidelines (7 items plus 1 open); (III) Personal style of the professional when giving orientations (14 items); and (IV) Orientations for training (11 items).
It also collects sociodemographic identification data of the main caregiver (sex, age, kinship with the child, level of studies, occupation, marital status, nationality and mother tongue), of the child (age, gender, number of siblings, place that occupies in the family, treatments that receives, difficulties and time that has been attending the centre), and about the professional (sex, specialty that exercises in the EI centre, years of experience, completion of specialization studies, performance of some position of responsibility, management or organization).
Results
We present the results of the SIPPEI Questionnaire comparing the responses of the two agents involved: families and professionals of EI.
Table 4 shows the means and standard deviations of the items in Dimension I (actions taken to give orientations), according to the opinions of families and professionals. It also shows results of the student's t test for differences between independent means and Cohen's d statistic to assess the size of.effect. The exact wording of the items in the two versions of the SIPPEI questionnaire can be found in Escorcia et al. (2016).
Table 4: Descriptive statistics, test t and d of Cohen in the items of the dimension I (actions carried out to give orientations) according to opinions of families and professionals surveyed.

According to families and professionals, the most common practices are, in this order, to give oral recommendations (item 2), suggest times of day and routines in which to implement the guidelines (item 7) and give written recommendations (item 1). The least frequent (never or almost never) are home visits (items 5 and 6) and commenting on video recordings (item 8).
We found statistically significant differences in all the items of dimension I between the opinions of professionals and families. Always with higher valuations from professionals. We highlight the differences found in items 3, 4 and 8, where results of moderate and high magnitude are reached in the test for estimating the effect size. Families perceive a lower presence and participation in sessions (items 3 and 4) than that estimated by professionals. Families think that almost never and only sometimes (M = 2.58; SD = 1.50) professionals develop the session while they are present (item 3); whereas the professionals think that this almost always happens (M = 3.93; SD = 0.99). Likewise, professionals indicate that almost always (M = 3.92; SD = 1.07) invite families to do activities with the child within the intervention sessions, while families think that this almost never happens (M = 2.08; SD = 1.28) (item 4).
Something similar happens in item 8, which asks about the use of video as a resource to offer guidance to families. The professionals approach their average answer to the verbal label sometimes (M = 2.65; SD = 1.03), while families indicate that this never or almost never (M = 1.66; SD = 1.24) the professional uses video recordings to offer guidance.
In Table 5, the descriptive statistics, tests t and the Cohen d statistic are presented to assess the effect size of the items that make up the dimension II of the questionnaire, referring to the difficulties that families can encounter in order to follow the guidelines of the professionals.
Table 5: Descriptive statistics, test t and Cohen's d test in the items of dimension II (difficulties to follow the guidelines) according to opinions of families and professionals surveyed.
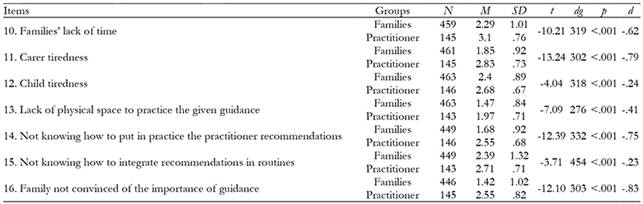
The items of this dimension present average answers that are usually between the verbal labels of never or almost never in the families and reach sometimes label in professionals. The highest scores are reached by the items referred to “not knowing” by families, how to integrate the guidelines given in their daily routines (item 15), lack of time of families (item 10) or problems due to fatigue of the child (item 12).
Once again, we found statistically significant differences in all the items of this Dimension II of the questionnaire when comparing the values of families and professionals. Professionals are the ones who always score higher in all the items. The differences in the valuation of items 10, 11, 14 and 16 are especially marked, where moderate and high magnitude results were obtained in the effect size estimation test.
Professionals point out that it is the lack of time of the families (item 10) that - sometimes makes difficult to follow the guidelines (M = 3.10; SD = 0.76), while the families think that almost never this is a problem (M = 2.29; SD = 1.01).
The professionals estimate that almost never and sometimes families are not convinced of the importance of following the guidelines (item16) (M = 2.55; SD = 0.82), or lack of knowledge when putting into practice the recommendations of the professional (item 14) (M = 2.55; SD = 0.67). On the other hand, families express that this happens never or almost never in the two cases (M = 1.42; SD = 1.02) (item 16) and (M = 1.68; SD = 0.92) (item 14).
The professionals estimate that sometimes the fatigue of the families can be a difficulty to follow the orientations at home (item 11) (M = 2.83; SD = 0.73). On their behalf, families estimate that this difficulty almost never arises (M = 1.85; SD = 0.92).
Table 6 shows the results of the items in dimension III of the questionnaire, referring to the personal style of the professional to offer guidance to the family.
Table 6: Descriptive statistics, test t and Cohen's d test on items of dimension III (personal style of the professional when giving guidance) according to opinions of families and professionals surveyed.

In this dimension, the valuations that both agents offer in the items are very high (between almost always and always, with a clear tendency toward the verbal label always). The only item lower valued (between almost never and sometimes) is the one referred to the flexibility to organize home visits (item 30). The rest of the items have average scores that always remain above 4 points. Even so, the items with lower scores are those that take into account the needs of families when proposing the intervention (item 31) and to know their concerns (item 24).
Of the 14 items that constitute dimension III, nine are valued significantly higher by families than by professionals (items 19, 20, 21, 23, 24, 25, 26, 28 and 29). In items 19, 23 and 25 the magnitude of the effect size was moderate.
The greatest differences between the assessments of both agents are given in items 19 and 23. Item 19 refers to a specific problem of difficulties in understanding the language in families with a mother tongue different from that of the professional. Item 23 refers to the professional’s time available to care families. Families tend to consider that professionals always have time to dedicate (M = 4.77; SD = 0.52), while professionals perform a somewhat lower assessment (M = 4.34; SD = 0.63).
Table 7 shows the descriptive statistics of the items that make up the IV dimension (guidelines for training), the student's t-test results for independent samples, and the Cohen's d statistic to assess the size effect.
Table 7: Descriptive statistics, test t and Cohen's d test in the items of dimension IV (guidelines for training) according to opinions of families and professionals surveyed.

The items of this dimension also reach high average scores in the two agents surveyed, many of them between the verbal labels of almost always and always. Items with lower scores are referred to involving other members of the family or friends in the intervention (item 33) and to provide families with materials and documentation to learn (item 42).
We found statistically significant differences in the opinions of families and professionals in items 35, 39 and 41. In items 35 and 39, families valued more than professionals the help offered to identify personal supports and the spirit offered to learn strategies that help to improve the development of the child. The estimate of effect size for these items was of low magnitude. However, in item 41 it is the professionals who score higher, stating that almost always the professional helps families to participate in groups and meetings (M = 4.26; SD = 0.63), while families believe that this occurs in less degree (M = 3.63; SD = 1.52). The estimate of effect size for this item was of moderate magnitude.
Finally, it is important to point out the high abstention of the group of professionals when answering the item 36 referred to discuss the objectives of intervention with the family. Only 79 of the 187 professionals surveyed, answered this item, which is 42.3% of the sample.
Discussion
The volume of participants in our study has been very satisfactory and representative of the groups involved. Especially taking into account that the functioning of the EI services of the Autonomous Communities of Valencia and the Region of Murcia is representative of what happens in most of the national territory; that is, an EI organized through autonomous centres that program outpatient interventions for the development of treatment sessions with the child, in which they insert orientations for families, from a position of the professional as an expert (GAT, 2000, 2011).
When performing an analysis of the results obtained in each dimension, we found coincidences and discrepancies between families and professionals when evaluating the different items. Firstly, regarding information exchange practices (Dimension I), both families and professionals agree that offering therapeutic recommendations orally or written, is the most common practice for transmitting information, while home visits are less common, modelling activities and corrective feedback after viewing videos. According to these results, the exchange of information, which is one of the basic pillars of the EI intervention processes, is perhaps not being addressed in the most appropriate way from the perspective of family-centred practices, that, facilitate participation and involvement of parents and encourage their learning. Taken into account how adults learn, the activities that promote greater learning and favour family training are modeling, including feedback on interactions and using coaching strategies (Knowles, Holton & Swanson, 2005, Rush & Shelden, 2011). The simple transmission of recommendations at the oral level does not ensure that the caregiver understands and will be capable of applying them. More difficult will be to include them in their daily routines, thus professional should help main caregiver to reach them. (McWilliam, 2010).
Within dimension I, professionals rate highly, to suggest to main caregivers, the moments of the day and routines, in which to implement their recommendations. Despite this, there are no visits to the natural environment, that allow the analysis of that environment and its routines: both families and professionals, point out that Never or almost never the professional visits the home, or guides there, or performs activities at home to train the caregiver.
In this dimension I, the analysis of the scores given to items by families and professionals shows opposing experiences. According to professionals, they almost always develop modelling actions with main caregiver (development of session being the caregiver present and showing it so that caregiver can repeat the exercise). So the professionals understand, that they make a correct practice. These results are contrary to the answers in the questionnaire carried out by the families, who affirm that these practices are almost never carried out. This difference of opinion makes us think about a possible overvaluation by professionals of their own practical activities, perhaps due to a need to project a positive image of their work. Being aware of the limits that EI training plans currently have in our country, we can also think that there may be, in some professionals, lack of training in strategies to carry out a different practice.
When assessing the problems encountered by families to follow the guidelines offered (dimension II), professionals are always more pessimistic in their assessments and see more problems than the families themselves. These families consider that difficulties such as lack of time, fatigue of the child and “not knowing” how to integrate the recommendations in the daily routine, are almost never or only sometimes. The professionals, on their side, consider that these problems are more frequent.
Once again, we see here the importance of applying the principles of family-centred services. Recall, for example, McWilliam (2010), when he talks about the importance of routines. If the professionals study family routines in depth, if they have the necessary time to know and help the families to analyse what happens in the house and in child’s environment, together they would be able to plan intervention objectives fully adapted to these routines, so they would not have this kind of sensations. In addition, it would be expected to obtain greater participation of the main caregiver, which would favour their autonomy and an improvement of their competence for the spontaneous use of learning opportunities that occur at different times of the day, which is what is advocated in practices that follow a family-centred approach (Dunst, Raab, Trivette, & Swanson, 2012; Dunst & Swanson, 2006; Trivette, Dunst & Hamby, 2010).
It is striking too, the significant differences found when asking, whether the family’s conviction about the importance of orientations is a problem for following them. Again, professionals show opinions that, on average, are between Sometimes and Almost always. Meanwhile, the answers of the main caregivers leave the average between Never or Almost never. Future investigations may attempt to elucidate whether parents are answering based on what they believe would be the desired response; or if professional’s response is signalling a distrust of the possibilities on main caregivers (McBride, Brotherson, Joanning, Whiddon & Demmitt, 1993).
In our results, families always value the professional's interaction style (dimension III) higher than the professionals themselves. This result is in line with studies such as those of Bailey and Bruder (2005), McWilliam et al., (1995), who comment that scores given by families on satisfaction are usually always high, expressing in this way a great satisfaction with the role of professionals and the support they receive from them. According to McWilliam et al., (1995), parents usually feel indebted to professionals and are reluctant to express what they think, for fear of damaging the image of the service that has ultimate responsibility for the development of their child. In the same sense, Bailey and Bruder (2005) thought that families tend to feel obligated to positively qualify performance of the professional who helps their children.
Now, if this effect exists in our data, it is only observed in that dimension III, referred to the professional interaction style. When assessing specific actions carried out in the information exchange practices (dimension I) or possible problems encountered by main caregivers to follow guidelines from professionals (dimension II), are professionals who present significantly higher mean scores than those reached by families. Professionals value all proposed actions of information exchange practices, as they perform them more intensely or more frequently than the families that are subject of them.
High scores indicated by both agents in dimensions III and IV, referred to styles of interaction of the professional and actions carried out to help the personal growth of the main caregiver, indicate that relationships between Primary Caregivers and professionals are based on respect, trust, listening, availability, etc. These aspects are undoubtedly part of positive relational professional practices (Espe-Sherwindt, 2008, García-Sánchez et al., 2014). These results are in line with what was expressed by authors such as Dunst and Dempsey (2007), McWilliam, Winton and Crais (2003), among others, who consider that these aspects undoubtedly mark relationships and are the basis for a truly coordinated work between parents and professionals.
In dimension IV, the lowest scores obtained by professionals, where those items that refer to involvement of other family members and the invitation of the family to participate in training activities or opinions exchange. Leaving aside these aspects, it makes it difficult to count with: resources from family and social supporting networks and also with the positive implications they have in EI. As Serrano stablished (2007) there are relationships between social support and different aspects of the child’s development and the functioning of parents and family.
It is interesting to note the set of items that have resulted with a greater volume of blank responses. For example, the one related to flexibility for intervention in the environment, which was the one that obtained the lowest score of its dimension. (Dimension III). This item (item 30) was not answered by 35.7 % of the families surveyed or by 28.9 % of the professionals. Quite possibly this was due to understanding that they should not value a practice that was not done. On the whole, this item is the one that more agents surveyed have left without answering.
The following less-answered items are those referred to giving materials to families or documents for personal growth (not answered by 15.9 % of the families surveyed); taking into account the needs of the family to propose interventions (item 42), not answered by 12.9 % of the professionals surveyed; and to discuss objectives of intervention with family (item 36), in this case, not answered by less than 57.7 % of professionals. All this are participatory practices. Precisely the type of practices that contribute most to focus service on family and away from the positioning of expert professional models (Espe-Sherwindt, 2008).
Many of our results have led us to interpretations that find support in results described by Sawyer and Campbell (2009), who show that perception of professionals about their own practices does not seem to coincide with the reality of the EI services. They also coincide with the study conducted by Cañadas (2013), who concludes that family participation is not a usual practice, at least in the centres of the Valencian community. On the other hand, these results are totally opposite to those obtained, with Portuguese samples, by Pinto (2013) or those exposed by Boavida, Aguiar and McWilliam (2014). They show that the use of contextually mediated practices and training for use of individualized family support plans based on routines are widely used in Portuguese contexts. Portugal is a country where by law, the EI is developed following family-centred practices (Pinto et al., 2012, Serrano & Boavida, 2011).
Conclussions
Results obtained show us a clear tendency, on the part of professionals, to use relational rather than participatory practices. Thus, there is a need to promote a change to bring us closer to the international standards of practices centred on the family, which are currently the most recommended.
The interpretation of many of the answers offered by professionals, compared with the interpretation of answers provided by families, show us two different perceptions. The professionals are convinced that they are really trying to involve the family in the intervention and the family doesn’t not know how or can’t put into practice the recommendations made to them. On the other hand, the responses of the families make us see that the concrete actions of these professionals are still far from the usual participatory practices in family-centred services.
Incorporating training programs for professionals could substantially contribute to improving the quality of the intervention and bring it closer to family-centered models. These training programs should include the use of tools such as interview based on routines, in order to use it to establish functional intervention goals and objectives in the child's natural environment as proposed by Boavida et al. (2014). Likewise, they should include other possible strategies, such as the use of contextually mediated practices, as described by Dunst et al. (2012). They could be very valid alternatives, to try to develop more positive and successful interventions, thus achieving greater adherence of the main caregivers to this type of intervention.
Although official documents, such as the White Book of the TA (GAT, 2000), recognize the need to involve the family in the intervention and make them competent and responsible of favouring the development of their child, surely the practices that are being developed by the professionals are not contributing in the best possible way to this. In this sense, our results should lead us, perhaps, to become aware of the need for a conceptual change, which in other countries of our environment already is being carried out for years.
This process of joint reflection will help us to establish improvement proposals aimed at building parent-professional relationships that are more effective, sincere, open and flexible; where everyone can become considered part of the team that seeks a common goal: the physical and emotional well-being of the children and their environment.

