










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The term Autism Spectrum Disorder (onwards, ASD) refers to a childhood-onset neurodevelopmental disorder characterized by deficits in communication and social interaction and restrictive and repetitive behaviors frequently associated with alterations in sensory processing. ASD is diagnosed in almost 62/10,000 people, causing clinical significant difficulties in almost all areas of life (APA, 2013; Elsabbagh et al., 2012). Current diagnostic criteria recognize various levels of severity within the ASD, being necessary to specify the person's verbal and non-verbal intellectual level, their concurrent medical and psychological pathologies and other factors. In this context, two issues are of interest about people with ASD without intellectual disability (onwards, ASD-noID; also referred in literature as Asperger Syndrome and High-Functioning Autism). The first one refers to the frequent co-occurring clinical disorders they suffer across their lifespan. The second one refers to the tools that would help professionals to detect and address those disorders more adequately.
Regarding the first issue, anxiety, depression, obsessive-compulsive disorder, deficits of attention and sensory disturbances have been indicated in the literature as the most prevalent comorbidities of people with ASD-noID (Catino et al., 2019; Guerrera et al., 2019; Paula & Martos, 2009; Prosperi et al., 2021). Addictions, personality disorders, tics, disruptive impulse control disorders, disorders related to eating, weight and body image have also been described, not being uncommon for a person to receive two or more of these diagnoses (Lugo-Marín et al., 2019; Matson, 2016). Clinical comorbidities significantly predict poorer adult outcome, lower occupational functioning, and impaired quality of life (onwards, QoL) (Oakley et al., 2021). They generate for people with ASD-noID difficulties equal to or greater than those caused by the ASD itself (Adams et al., 2014). However, and related to the second issue, it is known that: (a) sensory and communicative peculiarities of people with ASD-noID condition limit the perception that they have of their own discomfort, also making it difficult for other people to detect it; (b) people with ASD-noID usually avoid going to mental health services on their own initiative to communicate their problems; and (c) concurrent psychopathological symptoms are easily confused with some core features of ASD (e.g., social avoidance or attachment to routines), hindering both their identification and their professional handling. All of these circumstances result in the vulnerability and singularities of them due to their mental health continues under detected, making it difficult to design and implement support strategies well-targeted (Sindermann et al., 2019).
Even for adolescents and adults with ASD-noID, it is usually parents or teachers who report their behaviors and difficulties through interviews and questionnaires in both clinical and research contexts (e.g., Ben-Sasson et al., 2019). Clinicians consider parents to be the most accurate informants due to their accessibility to different contexts and more examples of their kids' behavior (Storch et al., 2012a, 2012b). However, previous research findings are inconsistent. Some studies report a bias in parents that amplifies or overestimates the severity of their children's clinical problems and underestimates both their Social skills and QoL (Knot et al., 2006). However, other studies showed a trend in the opposite direction (Guerrera et al., 2019). Restricted to only some of the anxiety disorders and using the “Structured Clinical Interview for DSM-IV Childhood Diagnoses/KID-SCID”, Bitsika and Sharpley (2014) and Blakeley-Smith et al. (2012) verified that parents reported their sons' specific phobia, obsessive compulsive disorder, generalized anxiety disorder and social phobia symptoms significantly more often than the kids themselves did. However, the differences between ASD and their parents' ratings on the “Cognitive Abilities Screening Instrument/CASI)” were minimal and statistically no significant, suggesting an interaction between domain assessed, informant and measuring tool.
Otherwise, it is a common assumption that the sensory, proprioceptive and communicative difficulties derived from an ASD, and particularly alexithymia (the impaired ability to identify and describe emotional states -Kinnaird et al., 2019; Vaiouli & Panayiotou, 2021) radically prevent people with ASD-noID from providing reliable and valid self-reports (or at least, reports as reliable and valid as those provided by their parents and teachers). That assumption is also far from having been empirically confirmed. However, it is a fact that the use of self-reports referred to co-occurring clinical disorders with people with this diagnosis is still almost anecdotal, despite this methodology is particularly useful when direct assessments by specialists are difficult to carry out. Leaving aside other advantages, in clinical settings self-reports are preferable to other measurement tools since they both give easy access to reasonably reliable information and correlate satisfactorily with other types of measures (Andrés et al., 2003).
Referred to people with ASD-noID, a few previous studies concluded that they are capable of interpreting and making attributions about their social situation and internal experiences despite their difficulties to mentalize (Mazefsky et al., 2011; Park et al., 2019). Self-reports have also been successfully used both as a source of information to detect and diagnose ASD (Posserud et al., 2013), to evaluate clinical (Ozsivadjian et al., 2014) and to identify needs of support that would improve their QoL (Belinchón et al., 2008; Jennes-Coussens et al., 2006; Renty & Roeyers, 2006).
Some studies showed that the scores provided by parents and their children with ASD-noID significantly differ (Bergman et al., 2020; Fortea-Sevilla et al., 2016; Pisula et al., 2017) while other studies found no differences (Bergman et al., 2020; Chalfant et al., 2007; Ozsivadjian et al., 2014). Therefore, a key preliminary question to elucidate is whether their self-reports match the reports provided by their parents to the point of being able to replace them either in special circumstances (e.g., those derived from pandemics) or with specific goals (e.g. clinical screening prior to a face-to-face consultation in mental health services). This question, to our knowledge, has not yet been previously reviewed in a systematic way, although its implications for both clinical practice and research are vast.
The general objective of the present meta-analysis was to synthesize the empirical evidence available about the level of agreement between the evaluations provided by ASD-noID people and by their parents. To identify potential moderating variables on these evaluations was the second one of our aims.
Method
Information sources and search strategy
For the development of this work, the PRISMA expanded checklist for systematic reviews and meta-analyses was used. We conducted a search for studies on self-report in individuals with ASD-no ID in the following databases: PsycINFO, Google Scholar and MEDLINE. The principal descriptors used in English and Spanish were self-report tool, parent-child agreement, multi-informant, self-perception, comorbid symptoms, and psychiatric comorbidity in ASD/HF-ASD population. The keywords of the selected articles related to the subject of the study were added as descriptors and the references of these articles were also analyzed. For more information on the search string, a table with detailed information on the combination of Boolean descriptors and operators used was included in Table 1 of the supplementary material. The search was limited to documents published up until December 2020. To reduce publication bias, both formal sources (in article databases) and informal sources (conference proceedings and doctoral theses) were reviewed. All kind of studies could be part of the meta-analysis.
Eligibility criteria
The study selection process is presented in the PRISMA flowchart (Figure 1). After entering the descriptors presented in Table 1 of the supplementary material, the inclusion and exclusion criteria were established. We selected studies that met the following inclusion criteria: (a) studies of individuals with ASD-noID, with at least one comparison group that would be the parents; (b) studies published in English or Spanish; (c) studies using self-report tools; (d) studies that provided statistical data that allows the calculation of effect size; (e) at least 4 studies measuring the same domain. The exclusion criteria were: (a) studies in which it was uncertain the individuals or the tools involved; (b) narrative reviews and empirical articles that subjectively evaluated ASD self-reports; (c) studies of individuals with ASD plus ID; (d) only evaluations provided by parents or professionals.

Table 1. Studies that provide evidence on the correlations and details of their estimates.
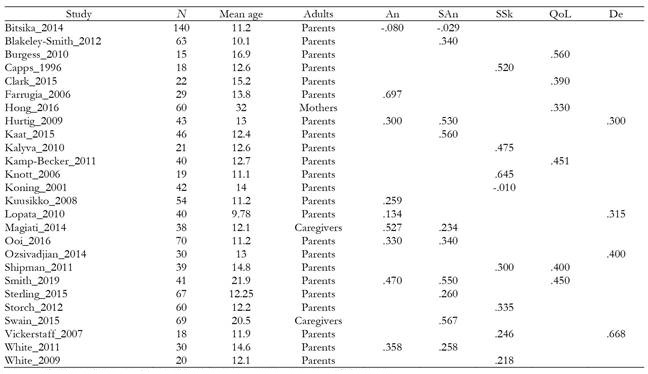
*An= Anxiety; San= Social anxiety; SSk= Social skills; QoL= Quality of life; De= Depression.
*The values of the five columns to the right are the Pearson's correlation coefficients.
*See in supplemental material all the references.
Figure 1 shows a flow diagram with the studies included in the meta-analysis. First, 158 records were identified through database searching (abstract and keywords), then they were selected after analyzing papers with ASD-noID population and inter-parental/cross-informant report. From these 67 records, only 42 fulfilled the conditions and only 32 were finally included in the meta-analysis (data, domains and measure tools).
Studies which met the exclusion and inclusion criteria were reviewed by two of the researchers (JB and MD), who established whether the papers should be part of the systematic review or not. Data from studies were extracted by one reviewer (MD), while the other assessed the integrity and quality of this data extraction (JB).
Procedure
Result of the selection process
After applying the inclusion and exclusion criteria and removing papers with duplicated participants, a total of 32 primary studies remained to be included in this meta-analysis. The supplemental material includes the references of these studies and the instruments that were used (Table 2 and 3).
Table 2. Summary of results on correlations, for the five domains.

*p < .05;
**p < .01;
***p < .001
aAll but one of the fail-safe numbers in this table are higher than the Rosenthal's criterion (5k + 10).

Data extraction
To avoid biases, prior to the search and selection of articles, the quantitative and categorical variables potentially moderating the results were analyzed. Following Lipsey (2009), these variables were classified as substantive, methodological and extrinsic. Our substantive moderating variables were age (and its standard deviation), distribution by hetero-informant, correlations and average results (and their standard deviations) of kids and their parents' evaluations. The categorical methodological variables were between-group comparison mode, dependent variable used and type of task/report. The quantitative methodological moderating variables were differences between average ages, differences between the percentages of the distribution by gender, groups of informants, type of the tasks, evaluated domain, quality index (Sanduvete, 2008) and the statistical data. Finally, the extrinsic variables were year of publication, source, and professional background of the first author.
The papers were distributed according to the evaluated domain by statistics results on the test: correlation index in Anxiety (k = 9), Social anxiety (k = 10), Social skills (k = 8), QoL (k = 6) and Depression (k = 4); and average and standards deviations in Anxiety (k = 12), Social anxiety (k = 10), Social skills (k = 8), QoL (k = 9) and Depression (k = 6).
Correlation, means and standard deviation values between ASD population and those given when evaluated by their reference adults were analyzed due to the possibility of a linear correlation between them.
Data analysis
As advanced above, to achieve our objectives it was necessary to analyze two types of data. On the one hand, the data reflecting the degree of correspondence between the assessments made through self-report by the ASD-noID participants themselves and the assessments made by their reference adults. On the other hand, the differences between the average values measured in those same evaluations. For the first case, the effect size index is Pearson's correlation and for the second, the standardized mean difference for correlated measures (Botella & Sánchez-Meca, 2015; Morris & DeShon, 2002). Statistical analyses assumed a random-effects model, that is generally preferred because it is more conservative than a fixed-effect model and allows generalizing conclusions beyond the specific set of studies included (Borenstein, Hedges, Higgins, & Rothstein, 2010). The combined estimates were calculated weighting the studies by the inverse of their variances, and the specific or between-studies variances that were estimated through the REML method (Viechtbauer, 2010).
For the analysis of the correlations, they were first transformed to Fisher's Z to have a more symmetrical distribution, and finally the combined statistics were transformed back to r for the reports. For the analysis of the means, the standardized mean difference (Cohens d) was obtained by subtracting the mean of the ASD from the mean of the reference adults, so that positive values indicate that the mean is higher in adults and negative values that the mean is higher in the ASD. The values were corrected for small sample bias (Botella & Sánchez-Meca, 2015; Hedges & Olkin, 1985). To calculate the variance of d for dependent samples, it is necessary to know the correlation between the scores. In some studies, this correlation was not reported, so it was estimated using the sample size-weighted average of the correlations of the studies that did report it. Table 4 includes the values used as estimates of the studies missing it, in each domain. Several studies report enough information to calculate d for several outcomes related to the same domain. In those cases, the d value entered in the meta-analysis is the simple mean of those estimates, since their sample sizes are equal by design.
Heterogeneity was assessed through the Q statistics (Huedo-Medina et al, 2006). No moderator analysis was performed since the corresponding tests are very low powered with so few studies. Publication bias was not tested as such, again because of the low number of studies involved. However, we obtained the funnel plots for visual inspection and the fail-safe numbers (Botella & Sánchez-Meca, 2015; Rosenthal, 1979). When the number of studies involved is small and the fail-safe number reveals that the existence of any effect is threatened by publication bias, the result is inconclusive. However, when the fail-safe number is high, the conclusion about the existence of the effect is reinforced because it is obtained with few studies. The threat was assessed by comparing the fail-safe number with Rosenthal's (1979) criterion. Statistical analysis and figures were obtained through metafor R package (Viechtbauer, 2010).
Results
Meta-analysis of correlations
Table 1 details the estimates involved in the study of the correlations between the self-reported scores by the ASD-noID participants and those given when evaluated by their reference adults. Additional information at the study level is also included, such as the sample sizes, the mean ages of the ASD groups and the relationship of the people involved in children and adolescent's assessment. Most studies provide estimates in one or two domains. Only two studies provide estimates for three domains.
It is assumed that the congruency and the reliability must be always statistically significant, so the issue is how large they are. At the study level the Anxiety domain reached the highest correlation (.697 value in Farrugia (2006)) followed by Depression (.668 value in Vickerstaff (2007)), Social Anxiety (.567 value in Swain (2015)) and QoL (.560 value in Burgess (2010)); and the lower value is found in the Social skills domain, specifically the study by Koning (2001) with a coefficient of -.01. Left column of Figure 2 shows the forest plot for each domain.

Table 2 shows the pooled estimates of the correlations in the five domains, and a summary of the results. In general, the combined correlations are within a short range. The domain with the highest pooled correlation is QoL (.409) followed by Depression (.383), Social Anxiety (.364), Anxiety (.330) and, finally, the lowest is Social skills (.322). Anxiety and Social anxiety reach significant levels of heterogeneity, as reflected in the column with the Q values. All but one of the fail-safe numbers are higher than the Rosenthal's Criterion. The latter is lower, but very close to that criterion. So, the existence of a nonzero correlation is not threatened by publication bias.
Meta-analysis of means differences
Table 3 details the estimates involved in the study of the means difference between the self-reported scores by the ASD participants and the scores given when evaluated by their reference adults. Additional information at the study level is also included, as well as the sample sizes and the mean ages of the ASD samples and the relationship of informants. Most studies provide estimates in one or two domains. Only three studies provide estimates for three domains.
The Depression domain reached the highest value (1.20 value in Nicpon (2010) and the Social skills domain the lowest, in Vickerstaff's (2007) paper with -1.33. On one hand, close to the highest value are 1.02 (Meyer, 2006) and 1.01 (Vickerstaff, 2007). On the other hand, nearby the lowest is Nicpon's (2010) paper with -1.31. Right column of Figure 2 shows the forest plot for each domain.
Table 4 shows the pooled estimates of the standardized mean difference in the five domains, and a summary of the results. The third column shows the value of the correlation employed for the imputation when needed (see the Method section). The Anxiety and Social anxiety domains do not show significant differences between informants, but they do in the other three domains. Specifically, adults attribute higher levels of depression to ASD-noID people than that people attribute it to themselves in their self-reports. Besides adults' attribute lower levels of Social skills and of QoL than those that people with ASD self-attribute (significant negative difference). All but one domain (Depression) shows significant levels of heterogeneity, as reflected in the column with the Q values. All calculated fail-safe numbers are higher than the Rosenthal's Criterion. So, the existence of a nonzero mean difference is not threatened by publication bias.
Table 4. Summary of results on the standardized mean difference, for the five domains.

*p < .05;
**p < .01;
***p < .001
bThe Nfs is not calculated for the domains where the effect is not statistically significant; all the values in this column are higher than the Rosenthal's criterion (5k + 10).
cAll studies on depression reported the correlation.
Discussion
This meta-analysis selected 32 studies that provide relevant information to evaluate the degree of concordance between the assessments given by people with ASD-noID and their reference adults (mainly parents) on various domains of the former's functioning. As far as we know, this is the first meta-analysis in which a combined effect size is obtained indicating the degree of agreement between the reports of these two groups. The studies we analyzed provided enough information on Depression, Anxiety, Social anxiety, QoL and Social skills.
In order to evaluate the results, three aspects of this meta-analysis must be taken into account from the outset.
First, the correlations between two evaluative sources reflect the degree to which those sources are based on the same cues. Only if the cues taken into account and their subjective weighting are similar, can there be a high correspondence between the two sources. As in the evaluation of other constructs (e.g., reliability), the important thing here is not whether the correlation is significant (different from 0), but whether its magnitude is relevant. In the case of ASD-noID individuals and their parents, we lack enough quantitative re ferences in previous literature. Therefore, the most that we can expect for, if these individuals are able for self-evaluation, is that these correlations are of a similar magnitude to those obtained with TD individuals. But we also don't have many previous estimates on that, reason why a main contribution of this meta-analysis is to provide a pooled estimate that can serve as a reference for future studies. In the context of research on the TD youth-parent agreement on the “Child Behavior Checklist (CBCL)” and other measures like those we meta-analyzed, the average level of correlation found was around .25 (Achenbach et al., 1987). In the present meta-analysis, the mean of ASD-noID group correlations was .40, a value also higher than those obtained in some studies on autism (e.g., Lopata et al., 2010; Ozsivadjian et al., 2014).
Second, even if the correlations were high and we could conclude that these two sources of evaluation are based on the same evidence, the estimates of the general magnitudes could be very different. In that case the mean values of the provided by the two sources could differ in magnitude despite a high correlation. For this reason, it is essential to accompany the analysis of the correlations with a comparison of the means.
And third, the number of studies we have for each domain was small, therefore the power of the tests is moderate and sometimes low (Pigott, 2012).
In our results, the combined estimates of the correlations between the assessments of the two sources in the five domains analyzed are significant (the responses of the ASD-noID individuals are not random or based on bizarre evidence, unrelated to what is intended to be evaluated), being within a narrow range (.322 - .409). We believe that this high convergence of estimates, that is even higher to the one previously obtained with TD individuals, may reveal a window of overall values, providing a reference for domains not studied here. In summary, we cannot conclude that people with ASD-noID are less able for self-assessment than individuals from the general population. The correlations obtained between self- and hetero-reports confirm that they are capable of both expressing their psychological experiences (Farley et al., 2010; Mazefsky, Kao & Oswald, 2011; Nylander & Gillberg, 2001) and providing self-reports aligned with their parents' reports (Chalfant et al., 2007; Ozsivadjian et al., 2014). In the absence of estimates in other populations, we limit ourselves to offering the estimates derived from the analyzed studies, as well as suggesting that ASD parents-child's convergence is no worse than it is in TD and other clinical samples of children and adolescents (Sterling et al., 2015).
Regardless of the value of the correlations, the mean differences offer relevant information regarding the perceived intensity of the cues assessed. A “normalization” of a symptom can lead to the mean values differing, despite a high correlation, by a simple linear shift of the values along the scale. The combined estimates we obtained for the differences in means offer mixed results. Unlike some previous studies (e.g. Nicpon et al., 2010), no significant differences were obtained in two domains: general Anxiety and Social anxiety. In both cases, the point estimates are close to 0, but they are just the two domains with the highest number of studies (12 and 11). We therefore believe that these are relatively robust results that can be interpreted with confidence. These results do not indicate that the two evaluation sources perceive quantitatively different anxiety levels in the means of these two domains. On the contrary, there is a suggestion of these differences in the other three domains. In Depression (k = 9), parents perceive an average symptomatic level higher than that perceived by their children. Conversely, the values in SSk (k = 8) and QoL (k = 6) perceived by the parents are significantly lower than those of the children. These differences globally coincide with previous comparisons showing that parents tend to both overestimate the clinical problems of their kids (Moss et al., 2015; Pearl et al., 2016) and underestimate their level of Social skills and QoL (Knot et al., 2006). Besides, research on perceived needs of support of people with ASD-noID (e.g. Jennes-Coussens et al., 2006; Powell, 2002) reaches similar conclusions, also revealing that their QoL is considered poor by all informants and that having personalized support to improve Social skills is a priority need for them (see also Atwood, 2000).
Our results also lead to the intriguing issue of why in two specific domains there are no differences while in others three there are. This analysis can help us to understand the way in which individuals with ASD-noID perceive themselves and also to calibrate whether self-reports could be used as a reliable source of information (e.g., for screening and diagnostic purposes, or when access to mental health services is difficult). In those three domains differences go in the direction that adults perceive them worse (greater depression, lower skills and worse QoL) than themselves.
The lower scores in Social skills and QoL are probably related to the characteristically impoverished social and community experiences of people with ASD-noID, which impedes common references to compare. However, the fact that clinical problems such as Anxiety and Social anxiety showed a different pattern than Depression deserves other considerations.
From a psychopathological point of view, anxiety and depression are considered as “internalizing behaviors” (versus “externalizing” ones such as rule-breaking and aggressive behaviors). Their severity and frequency increases with age in some cases whereas in others decreases (Orm et al., 2021). But their symptomatic variants are yet scarcely known by both people with ASD-noID and their families, their prevalence also varying depending on gender, age and many other biopsychosocial factors (APA, 2013; Paula, 2015). Anxiety disorders provoke signs (as episodic sweating, trembling, flushing, motor agitation, etc.) easier to detect and objectify than depressive ones (sleep problems, poor appetite, motor slowdown and others). Besides, symptoms associated to Anxiety (and Social anxiety) would be highly disruptive in people with ASD (Paula, 2015). Thus, the physiological, cognitive and/or behavioral correlates of Anxiety could be issues that parents, teachers and people with ASD-noID more often talk about than they do about symptoms of Depression, leading to more shared linguistic descriptions and greater homogeneity between self- and hetero-reports in the first case than in the later.
On the other hand, and now turning the focus to the skills of the informants, it seems relevant to keep in mind that a high percentage of parents of people diagnosed with autism exhibit a Broad Autism Phenotype (BAP), a sub-clinical group of traits similar to those on which the diagnosis of ASD is based (Piven et al., 1997). One of these traits is alexithymia (that is, the inability to recognize or describe one's own emotions -Szatmari et al., 2008). Having alexithymia with or without concurrent BAP probably modulates parents' ability to detect their children's clinical symptoms in a similar way to how having ASD biases self-reports, favoring greater inter-rater agreement (i.e., higher positive correlations) in disorders that, such as anxiety, are easier to observe. To our knowledge, neither the possible BAP nor the alexithymia of the parent-informants have been controlled in the studies on self-reports included in our meta-analysis. Thus, we cannot rule out that such traits of informants could favor closer self- and hetero-reports on anxiety symptoms than on depressive ones.
Finally, this meta-analysis included studies with children and adolescents with ASD-noID as participants, being more numerous those carried out with children. More studies are needed to test how age could influence their self-reports, especially on clinical co-occurring symptoms with different developmental trajectories (Orm et al., 2021). Previous research reported that parents rated their ASD child's anxiety more severely than the child did themselves (Blakeley-Smith et al., 2012; Gillott et al., 2001; Russell & Sofronoff, 2005; Storch et al., 2012a). However, this effect was reversed for adolescents, who, in some studies, rated their anxiety higher than the scores their parents gave for them (Hurtig et al., 2009; Smith et al., 2019). The differences between parents' and people with ASD' ratings are that the latter's anxiety has also been associated with the type of assessment tool used and the age group (Bitsika & Sharpley, 2014; Kaat & Lecavalier, 2015; Swain et al., 2015). Therefore, no conclusions can yet be drawn about the discrepancies between self-reports and hetero-reports referred to people with ASD as a whole, being necessary more in-deep comparisons from a developmental perspective, including wider ranges of age for participants and analysis of interactions between age, sex, domains assessed and tools.
Limitations and future directions
As we mentioned, the main limitations of this meta-analysis were the small number of published studies and the lack of information on the moderating variables, the latter being due to the low number of available studies and the small number of participants in each one (from 15 to 140 persons).
Despite these limitations, we were able to analyze 32 articles that provided very specific information and good methodological quality. We fitted categorical models with the moderators that had at least four studies within each domain. With papers that did not meet this condition, we calculated a combined estimate of the standard deviation or correlation values. Regarding the rest of the domains, either there are no primary studies of some aspects, or there are none that provide information to carry out an analysis with sufficient evidence.
The limited number of studies also makes it difficult to analyze the publication bias and its role as a potential threat to the conclusions. Given that with so few studies the asymmetry tests (like the Egger's test) are unstable, the conclusions that are derived from them can be considered reliable. However, the small sample of studies has not prevented the fail-safe number from successfully exceeding Rosenthal's criteria. This allows us to conclude with confidence that the very existence of the relationship between the variables is not challenged by that threat. Likewise, a greater number of studies would offer the possibility of studying moderating variables such as cognitive level, severity of ASD symptoms, gender, hetero informants (mothers, fathers, teachers), and others. New studies controlling factors such as alexithymia and BAP of parents-informants could also be necessary.
With respect to future research, using more databases and a greater number of studies providing data that allows knowing the effect of variables such as those previously mentioned could be favoring the use of self-reports for clinical and research purposes and in specific circumstances (e.g., less access to mental health professionals due to the pandemic, adolescents who do not desire parental involvement in their mental health situation, etc.). This, in turn, would facilitate an earlier detection and treatment of clinical comorbidities which can be more disabling than the ASD itself. Nowadays, ASD-noID is infra-diagnosed, being frequently those comorbidities misunderstood or confounded with core symptoms of autism. A better understanding of self-assessment processes in them would enable us to assess the validity of self-reports and design better ones for the fulfilment of the right to have the best possible quality of life for ASD people and their families. This strategy could be used with other populations, inside and outside the neurodevelopmental disorder's category (APA, 2013). However, the assessment tools to be used must take into account linguistic peculiarities of people with ASD-noID such as their extreme literality, something that is unfortunately still unusual in mental health services and research but prevents ensuring that they fully understand the questions about their own mental health (see, as an exception, Graham Holmes et al., 2020).

