










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.23 no.2 Zaragoza abr./jun. 2009
Prevalence rates of at risk, problematic and pathological gambling in Switzerland
Jeannette Brodbeck, Sara Duerrenberger, Hansjoerg Znoj
Department of Psychology, University of Berne. Switzerland
ABSTRACT
Background and Objectives: Few studies have assessed pathological gambling in Switzerland. We employed the National Opinion Research Center DSM Screen for Gambling Problems (NODS) to assess prevalence of gambling problems in German- and Italian-speaking Switzerland.
Methods: A random sample of 4997 individuals participated in a computer-assisted telephone interview in 2007 and 1388 of the individuals who refused to participate on the telephone interview completed a paper questionnaire. The total sample included 6385 participants (52% women); the return rate was 52.2%.
Results: Among the general population over 18 years of age, 2% engaged in lifetime at-risk gambling, 0.5% in problematic and 0.3% in pathological gambling. We found past-year prevalence rates of 0.7% of at-risk gambling, 0.1% for problematic and 0.02% for pathological gambling.
Conclusions: These rates are at the lower end of international statistics and are lower than rates in previous Swiss studies. This may be due to measures to reduce false positive diagnoses in our study. Large differences between lifetime and past-year prevalence rates indicate that problematic and pathological gambling are not necessarily progressive and chronic disorders.
Key words: Gambling; Prevalence; Switzerland.
Introduction
Problematic and pathological gambling are considered worldwide problems with potentially disastrous psychological, social and economic consequences for gamblers and people close to them. The current clinical definition of pathological gambling in the DSM-IV-TR includes three symptom clusters: disruption of the individual's life, loss of control and dependence with symptoms such as withdrawal and increased tolerance. Five of 10 criteria must be reached to qualify for pathological gambling and for problem gambling less than five criteria. However, some researchers consider a cut-off score of four criteria as more adequate for a diagnosis of pathological gambling1,2. In addition to person-based cognitive, personality and biological factors, structural characteristics of the games and social factors such as cultural attitudes towards gambling, structural preventive measures and the accessibility of gambling activities have an impact on the development of gambling problems3,4. Slot-machines especially have great potential for addiction5. In Switzerland, gambling is legally regulated by a governmental monopoly. The most popular gambling activities are lotteries. Casinos were prohibited until 2002. Today, Switzerland has a very high 'density' of casinos (19 for a population of 7,459,000 inhabitants). Casinos are legally obliged to implement prevention measures to detect at-risk gamblers early and harm reduction measures to reduce problematic and pathological gambling, such as (self-)exclusion at casinos. In addition, proper training of casino staff and provision of data for research are required. Counselling facilities and public campaigns to increase community awareness of problematic gambling have been established during the last years. Slot-machines, other than in casinos, have been prohibited since 2005; before that they had to make a submission for authorization.
To assess prevalence of problematic and pathological gambling, two instruments have been established and frequently used: The South Oaks Gambling Screen (SOGS)6 and DSM-IV-based instruments such as the National Opinion Research Center DSM Screen for Gambling Problems (NODS)7. The NODS is designed to be more restrictive than the SOGS and relates more closely to the DSM-IV-TR criteria of pathological gambling. About half of the SOGS items focus on sources of borrowed money and no items regard tolerance and withdrawal. Since, to date, there is no gold standard for the definition of pathological gambling, we rely on the current clinical definition of the DSM-IV-TR and the NODS.
Until now, few gambling prevalence surveys have been conducted in European countries. Different or even not specified timeframes, selection or sampling biases and different assessment measures complicate comparison of the existing studies8. Replications of results are often missing. Thus it is difficult to formulate well-founded statements about the frequency of excessive gambling in European countries. Excessive gambling seems to be more prevalent in the US, Canada and countries of Asia than in Europe3,8. A recent British study found one-year prevalence rates of 0.6% of problematic (including pathological) gambling in 20079. In Scandinavian countries recent one-year prevalence rates were around 0.4% for problem gambling and 0.1-0.2% for pathological gambling. An Italian study found one-year prevalence rates of 0.7% for problem gambling and 0.4% for pathological gambling8. In Switzerland only three prevalence studies of gambling problems exist. Bondolfi and colleagues10,11 found lifetime prevalence rates of 2.2% for problematic and 0.8% for pathological gambling in 1998 and of 2.2% for problematic and 1.1% for pathological gambling in 2005. Participants of the German-speaking part of Switzerland are however under-represented in these studies (32 and 36% in the study samples compared with 71% Swiss inhabitants in the German-speaking part of Switzerland). Therefore the database for this region is small and the generalizability is questionable. This is relevant because in the French-speaking part of Switzerland, the availability of gambling activities such as electronic gambling machines outside of casinos differs from the rest of Switzerland. A study by Zangerl and colleagues12 found five-year prevalence rates in the year 2004 of 1.9% for probable pathological gamblers and 1.8% for potential pathological gamblers or problem gamblers. One other study covering the Italian-speaking part of Switzerland found lifetime prevalence rates of 0.6% for both problematic and pathological gambling13.
Methods
Selection of respondents was done in two phases. First, a household was randomly selected from the Swiss telephone directory. This sample was designed to represent proportionally all regions of German- and Italian-speaking Switzerland according to the number of inhabitants. Then, one household resident over 14 years old, whose birthday followed most closely the date of the telephone call, was selected for the interview. These selection procedures helped to ensure that every household with a telephone had an equal chance to be included in the survey, and that each person of at least 14 years old present in the household had an equal chance of being selected. Data were collected by computer-assisted telephone interview (CATI). After excluding invalid telephone numbers, persons with insufficient mastery of the German or Italian language and individuals with serious health problems that precluded participation in the interview, we interviewed 4997 persons. The response rate was 40.4%. A paper version of the questionnaire was sent to all household residents who refused to participate in the telephone interview. Data were collected from December 2006 to June 2007. The response rate of the paper version was 19.2% (n = 1388). The overall response rate was 52.2%. In order to be comparable with other studies, the following analyses were only conducted with participants aged 18 or older (n= 6047).
The sample included 51.7% women and 48.3% men. Mean age was 48 years (X = 48.00, SD = 17.12, range 18-100). Half of the sample was married (52.4%), 30.4% were single, 12.0% were separated or divorced and 7.2% were widowed. With regard to education, 42.4% had completed a professional training, 25.9% had a university degree, 17.8% had completed a comprehensive or a specialized secondary or a business school and 11.1% had completed primary school.
Measures
For the month prior to the interview, respondents reported how often they had participated in a) lotteries, b) TV or SMS games, c) gambled in casinos, d) gambled on slot-machines outside of casinos, e) gambled on the Internet or f) participated in other games such as dice or cards for money (0 = never, 1 = 1-3 times a month, 2 = 1-2 times a week, 3 = 3-6 times a week, 4 = daily).
To assess DSM-IV criteria for pathological gambling, the National Opinion Research Center DSM Screen for Gambling Problems (NODS) was employed. The NODS includes lifetime and corresponding past-year items, each scored yes or no. The NODS labels a total score of 1 or 2 as 'at risk gamblers', 3 or 4 as a 'problem gambler' and a score of 5 to 10 represents a pathological gambler according to the DSM-IV definition.
A three-stage approach was chosen to exclude false positive diagnoses. First, respondents were asked if they had gambled in the past month, if they had ever controlled or tried to reduce gambling and if they ever spent more than 500 CHF (about 400 USD) a month on gambling. If each question was answered by no, respondents skipped to the demographic variables at the end of the interview. If one of these questions was answered by yes, we assessed gambling behavior for the month prior to the interview as a second stage. In the third stage the NODS was administered to participants who gambled at least weekly, who ever tried to control gambling, who ever spent more than 500 CHF, who regularly spent more than 300 CHF (about 250 USD) for gambling or who regularly gambled for at least two hours a day.
Data analyses: For the prevalence rates, the data for gender and age to represent the population in German- and Italian-speaking Switzerland was weighted proportionally. Confidence intervals for weighted data were computed with STATA, for all other analyses SPSS was used. Non-weighted data were used for inferential statistics.
Results
Frequency of participation in gambling activities
A third of the participants engaged in at least one gambling activity in the month prior to the interview (35.0%, n = 2116). The most prevalent gambling activities were lotteries (87.9% of the gambling population, which is defined as having gambled in the month prior to the interview, 30.8% of the general population, see Table I). Very few participants reported going to casinos or gambling at illegal slot-machines outside of casinos.

Prevalence rates of at-risk, problematic and pathological gambling
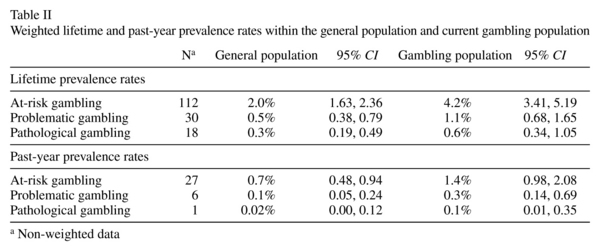
Lifetime prevalence rates
Lifetime prevalence rates of 2.0% of at-risk gambling, 0.5% of problematic gambling and 0.3% of pathological gambling were found within the general population (see Table II). Few participants reported gambling problems during the previous year. Past-year prevalence rates were 0.7% for at-risk gambling, 0.1% for problematic gambling and 0.02% for pathological gambling. Prevalence rates were considerably lower among women (see Table III).

Demographic characteristics of lifetime at-risk, problematic and pathological gamblers
Table IV gives an overview of the demographic characteristics of gamblers without problems, lifetime at-risk gamblers, and problematic and pathological gamblers. For statistical analyses problematic and pathological gamblers were designated excessive gamblers. Men were over-represented among at-risk gamblers and excessive gamblers (Chi - square (2, 2156) = 18.37, p < 0.0001, V = 0.09). Gamblers without gambling problems were older than excessive and at-risk gamblers (F (2) = 9.36, p < 0.001). At-risk gamblers and excessive gamblers did not differ in age. At-risk gamblers and excessive gamblers did not differ significantly in marital status or education. The prevalence estimates of gambling problems in German-speaking and Italian-speaking Switzerland did not differ (Chi - square (3, 625) = 5.21, p < 0.05).

Discussion
Compared with other countries, lifetime prevalence rates in German- and Italian-speaking Switzerland are at the lower end of the international statistics. Among the general population over 18 years of age, 2% (CI: 1.63, 2.36) engaged in at-risk gambling, 0.5% (CI: 0.38, 0.79) in problematic and 0.3% (CI: 0.19, 0.49) in pathological gambling. We found past-year prevalence rates of 0.7% (CI: 0.48, 0.94) for at-risk gambling, 0.1% (CI: 0.05, 0.24) for problematic and 0.02% (CI: 0.0001, 0.12) for pathological gambling. The prevalence rates for past-year gambling problems could -due to the very small number- be regarded as possibly too low. However, the rate for lifetime prevalence indicated that pathological gambling in Switzerland is relatively rare.
These low prevalence rates may be explained by regulative prevention and harm reduction measures in casinos, the short history of casinos in Switzerland and the restricted availability of gambling opportunities such as slot-machines outside of casinos. Also, rather negative cultural attitudes towards gambling and a high standard of living with good social security including counseling and psychotherapy may be reasons for the low prevalence rates of gambling problems. Scandinavian countries with a similar standard of living are also at the lower end of the statistics14. However, Scandinavian countries have a longer history of casinos and other gambling opportunities.
Lower prevalence rates were found than in previous Swiss studies. This may be due to several reasons: We employed the NODS instead of the SOGS, which was used in previous Swiss studies. In a treatment study, the percent agreement between the NODS and the SOGS was 52% and the SOGS categorized more participants as pathological gamblers than did the NODS15. Additionally, in previous Swiss studies, the German-speaking part of Switzerland, which has a different availability of gambling activities than the French-speaking part, was underrepresented and the weighted results might not be generalizable.
The major reason for this difference is the pre-screening process prior to the administration of the NODS. The NODS was administered only by subsample of 11% of the participants who gambled at least weekly in the month prior to the interview, who ever tried to control or reduce gambling, who ever spent more than 500 CHF (about 400 USD), who regularly spent more than 300 CHF (about 250 USD) for gambling or who regularly gambled for at least two hours a day filled out the NODS. This measure works to minimize false positive diagnoses.
Some researchers have discussed the appropriateness of applying clinical screening tests to a population-based sample to establish prevalence rates of low base rate disorders16. Clinical screening instruments are most capable of identifying a problem when the phenomenon is common among the sample population. For low base rate behaviors screening instruments have a low predictive value and may inflate the rate of gambling problems. In this case a pre-screening is an effective measure to reduce the risk of false positive diagnoses. However the use of a pre-screening bears the risk of an underestimation of gambling problems, whereas the use of a screening instrument without pre-screening may lead to an overestimation of gambling problems due to false positive results. The decision to protect against false negative or false positive errors depends on the goals of the study and the severity of the consequences of these errors. Gambino17 and Dickerson et al.18 argued that if the goal is to estimate the number of pathological gamblers in the community, a strict criterion to protect against false positive errors makes more sense. They assumed that the level of help-seeking gamblers is low and that policy-makers should plan for a conservative number of pathological gamblers expected to seek treatment. Interval estimates instead of point estimates, however, are a more reasonable measure of prevalence estimates of gambling problems17.
Large differences in lifetime and past-year prevalence rates also found by Bondolfi et al.11 indicate that problematic and pathological gambling are not chronic disorders and that psychotherapy or natural recovery significantly reduce gambling problems. Although there is a lack of prospective studies of the course gambling problems take, research to date suggests that gambling problems do not necessarily progressively grow worse once symptoms appear16. Slutske19 found that among individuals with a lifetime history of pathological gambling, 36-39% had not experienced any gambling-related problems in the past year and that about one-third were characterized by natural recovery. However, tendencies to minimize the negative consequences of gambling may be higher when reporting recent problems.
Compared with other addictive or affective disorders, the prevalence rates of problematic and pathological gambling are considerably lower. The past-year prevalence rate for a major depression is 6.9%, for an alcohol dependency 2.4% and for a dependency of illicit drugs 0.5%20. However, because of the short-term tradition of casinos in Switzerland, tendencies towards a deregulation of gambling and the rapid development of Internet gambling, further development of gambling activities and problematic and pathological gambling should be observed and epidemiological monitoring remains an important public health issue. Regulative prevention and harm reduction measures should be maintained and strictly controlled. Although problematic and pathological gambling is not a frequent disorder, psychological and social consequences for involved individuals and their families are severe. Sufficient opportunities for counselling and therapy are important and should be supported by the governmental gambling tax.
Limitations
An important strength of this study was the use of a large random sample of households in the German- and Italian-speaking parts of Switzerland, the random selection of a household member with the last-birthday method and the paper questionnaire for individuals who refused to participate in the telephone interview. Weighting procedures were used for further generalization purposes. However, telephone surveys exclude individuals in institutions, such as psychiatric hospitals or prisons, who have more gambling problems16 and ethnic or cultural subgroups who could not be interviewed because of language difficulties. Also, individuals who only use cell phones and who are not registered in the Swiss telephone directory could not be contacted. Finally, as a limitation in all telephone surveys, problem and pathological gamblers may more often refuse to participate in telephone interviews on gambling or may minimize the negative consequences of gambling. This and the use of the pre-screening measure might lead to an underestimation of the real prevalence rates. Past-year prevalence rates should be considered with caution since despite the large sample size only one person with pathological gambling was found.
Acknowledgements
We thank the German speaking cantons of Switzerland and the Canton of Tessin for supporting this study.
References
1. Stinchfield R. Reliability, validity, and classification accuracy of a measure of DSM-IV diagnostic criteria for pathological gambling. Am J Psychiatry 2003; 160(1): 180-182. [ Links ]
2. Lakey CE, Goodie AS, Lance CE, Stinchfield R, Winters KC. Examining DSM-IV criteria for pathological gambling: Psychometric properties and evidence from cognitive biases. J Gambl Stud 2007; 23: 479-498. [ Links ]
3. Shaffer HJ, Hall MN, Vander-Bilt J. Estimating the prevalence of disordered gambling behavior in the United States and Canada: A research synthesis. Am J Public Health 1999; 89: 1369-1376. [ Links ]
4. Treter F. Ökologie der Sucht [Ecology of Addiction]. Göttingen, Germany: Hogrefe; 1998. [ Links ]
5. Griffiths M. Gambling technologies: Prospects for problem gambling. J Gambl Stud 1999;15: 265-283. [ Links ]
6. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. Am J Psychiatry 1987; 144: 1184-1188. [ Links ]
7. Gerstein D, Murphys S, Toce M, Hoffmann J, Palmer A, Johnson R, et al. Gambling impact and behavior study: Report to the national gambling impact study commission. Chicago: National Opinion Research Center; 1999. [ Links ]
8. Stucki S, Rihs-Middel M. Prevalence of adult problem and pathological gambling between 2000 and 2005: An update. J Gambl Stud 2006; 23: 245-257. [ Links ]
9. Wardle S, Sproston K, Orford J, Erens B, Griffiths C, Constantine R, et al. British Gambling Prevalence Survey 2007. [Internet]. London: National Centre for Social Research; 2007. (cited 2008 October 10). Available from: http://www.gamblingcommission.gov.uk/UploadDocs/publications/Document/Prevalence Survey final.pdf [ Links ]
10. Bondolfi G, Osiek C, Ferrero F. Prevalence estimates of pathological gambling in Switzerland. Acta Psychiatr Scand 2000; 101: 473-475. [ Links ]
11. Bondolfi G, Jermann F, Ferrero F, Zullino D, Osiek C. Prevalence of pathological gambling in Switzerland after the opening of casions and the introduction of new preventive legislation. Acta Psychiatr Scand 2008; 117: 236-239. [ Links ]
12. Zangerl M, Munsch S, Meyer A, Margraf J. Prevalence and risk of pathological gambling in Switzerland after the legalization of games of chance and casinos in 2000. Paper presented at the 10th Congress of the Swiss Society of Psychology; 2007 September 13-14, Zurich, Switzerland. [ Links ]
13. Molo Bettelini C, Alippi M, Wernli B. Il gioco patologico in Ticino [Pathological gambling in Tessin.] [Internet]. Centro di documentazione e ricerca OSC; 2000 (cited 2007 October 3). Available from: http://www.ti.ch/DSS/DSP/OrgSC/cdr/temi/ricerca/ricerche.htm. [ Links ]
14. Jonsson J. An overview of prevalence surveys of problem and pathological gambling in the nordic countries. J Gambl Issues [Internet]. 2006; 18: 31-38. [ Links ]
15. Hodgins DC. Using the NORC DSM Screen for Gambling Problems as an outcome measure for pathological gambling: psychometric evaluation. Addict Behav 2004; 29: 1685-1690. [ Links ]
16. Shaffer HJ, Korn DA. Gambling and related mental disorders: A public health analysis. Ann Rev Public Health 2002; 23: 171-212. [ Links ]
17. Gambino B. Interpreting prevalence estimates of pathological gambling: Implications for policy. J Gambl Issues. [Internet]. 2005 (cited 2007 September 16); 14. Available from: URL: http://www.camh.net/egambling/issue14/pdf/jgi_14_gambino.pdf. [ Links ]
18. Dickerson MG, Baron E, Hong SM, Cottell D. Estimating the extent and degree of gambling related problems in the Australian population: A national survey. J Gambl Stud 1996; 12: 161-178. [ Links ]
19. Slutske WS. Natural recovery and treatment-seeking in pathological gambling: Results of two U.S. national surveys. Am J Psychiatry 2006; 163: 297-302. [ Links ]
20. Wittchen HU, Hoyer J. Klinische Psychologie & Psychotherapie [Clinical psychology and psychotherapy]. Heidelberg, Germany: Springer; 2006. [ Links ]
![]() Correspondence:
Correspondence:
Dr. phil. Jeannette Brodbeck
Department of Psychology
Gesellschaftsstrasse 49
CH-3012 Berne.
Switzerland
Tel. +41 31 631 45 81
Fax: +41 31 631 41 55
E-mail: brodbeck@ptp.unibe.ch
Received: 14 March 2008
Revised: 31 October 2008
Accepted: 19 November 2008

