










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkThe European Journal of Psychiatry
versão impressa ISSN 0213-6163
Eur. J. Psychiat. vol.25 no.2 Zaragoza Abr./Jun. 2011
https://dx.doi.org/10.4321/S0213-61632011000200001
Haloperidol and risperidone in the treatment of delirium and its subtypes
Soenke Boettger*; William Breitbart**; Steven Passik**
* Department of Consultation Liaison Psychiatry and Medical Psychiatry, Bellevue Hospital Center, New York University Langone Medical Center, New York
** Department of Psychiatry and Behavioral Sciences, Memorial Sloan Kettering Cancer Center, New York. USA
ABSTRACT
Background and Objectives: To compare the safety and efficacy of haloperidol and risperidone in the treatment of delirium and its subtypes
Methods: We collected sociodemographic data and medical variables in addition to systematically rating all patients with delirium with the Memorial Delirium Assessment Scale (MDAS), Karnofsky Performance Status Scale (KPS) and abbreviated Udvalg for Kliniske Undersogelser (UKU) at baseline (T1), 2-3 days (T2) and 4-7 days (T3) and created an IRB-approved delirium database. For this secondary analysis we extracted all data containing haloperidol (HAL) and risperidone (RIS).
Results: We were able to retrieve 32 patients treated with haloperidol (HAL) and risperidone (RIS) each. Both samples did not significantly differ in respect to age, cancer diagnoses or etiologies. The MDAS scores at baseline were higher in HAL treated subjects (20.2) compared to RIS treated subjects (17.7). The treatment results between HAL and RIS were not significantly different: Over the course of treatment MDAS scores improved from 20.2 to 8.3 (HAL) and 17.7 to 7.5 in (RIS), delirium resolution rates were 68.8% (HAL) and 84.4% (RIS). In hypoactive delirium the MDAS scores improved from 18.5 to 9.3 (HAL) and from 15.3 to 6.6 (RIS), delirium resolution rates were 64.3% (HAL) and 91.3% (RIS). In hyperactive delirium the MDAS scores improved from 22.5 to 6.6 (HAL) and 20.1 to 8.4 (RIS), delirium resolution rates were 72.2% (HAL) and 75% (RIS). There were no significant differences in KPS scores at all observation times. Treatment with HAL caused more EPS.
Conclusions: Both haloperidol and risperidone may be equally effective in the treatment of delirium and its subtypes. Treatment with haloperidol resulted in more side effects.
Key words: Delirium; Treatment; Haloperidol; Risperidone; Antipsychotics.
Background
Delirium is a neuropsychiatric disorder characterized by disturbances of consciousness, attention, cognition, and perception with an abrupt onset and fluctuating course. Delirium usually has an underlying physiological etiology1.
Delirium is a common event in the course of hospitalization depending on the age of the patient and the severity of the illness. In a general hospital setting the occurrence of delirium in medically ill patients can be up to 30%, in the hospitalized elderly between up to 40%2,3, in cancer patients between up to 85% and in terminal illness the incidence of delirium can reach 85%4-6. On admission 14 to 24% of older patients may be delirious and 6 to 56% will go on to develop delirium in their course of hospitalization2,3. Delirium is associated with poor functional outcome, increased morbidity and mortality and prolonged hospitalization7.
The standard approach to the pharmacological treatment of delirium involves the use of antipsychotics, in particular, haloperidol1. Atypical Antipsychotics, although used off-label, have been the first choice for treatment of delirium due to a lower rate of side effects8. Several studies have suggested the safety and efficacy of risperidone in the treatment of delirium9.
In the existing studies of haloperidol and risperidone both have shown similar efficacy in the management of delirium: Liu10 was not able to find differences between haloperidol and risperidone in a retrospective chart review. Han11 could not find differences in efficacy between both medications: In the haloperidol group there was an MDAS improvement from 21.8 to less than 13, the resolution rate was 58.3% on day 3 and 75% at the end of the study on a regimen of 1.71 mg haloperidol; one patient (8%) on haloperidol experienced akathisia. The risperidone group contained 12 patients, the baseline MDAS score was 23.5, the mean risperidone dose was 1.0 mg; the delirium resolution rate was 33.3% at day three and 42% at the end of the study. No side effects were observed in the risperidone group11.
In a later study on antipsychotics and dopamine transporter gene polymorphisms including 42 cases of delirium, the same authors found a decrease in DRS scores from 22.04 to 8.0 (HAL) and 21.61 (RIS) to 9.72. The dosing was 1.67 mg and 1.19 mg respectively12.
We performed a secondary analysis of our delirium database in respect to all patients treated with haloperidol and risperidone in order to further examine the treatment response in the subtypes of delirium, the effect on functional status and occurrence of side effects.
Methods
Subjects
Subjects in this trial included patients referred for delirium management to the Memorial Sloan Kettering Cancer Center (MSKCC) Psychiatry Service from July 2004 to June 2006. Clinical data, including serial MDAS ratings, etiologies of delirium, medications and dosages utilized, adverse events and co-morbid medications and medical conditions were recorded in an Institutional Review Board (IRB) - approved MSKCC Psychiatry Service clinical database. The delirium database was registered with the Institutional Review Board, and a waiver was obtained for the analysis of the data.
All patients treated for delirium met criteria for diagnosis of delirium according to the Diagnostic and Statistical Manual Mental Disorders, IV. Edition (DSM-IV-TR)13. Inclusion criteria were broad, meeting DSM-IV-TR criteria for delirium and being able to comply with delirium assessment. Patients on previous antipsychotic medication with limited response or side effects were equally assigned to HAL and RIS as patients without any previous treatment with antipsychotic medication for delirium. Exclusion criteria were objections on the side of the patient or family to treatment of delirium with any antipsychotic, severe agitation, critical medical condition and imminent death. All patients and families gave verbal consent to be evaluated and treated for delirium. In patients with limited capacity to provide consent due to delirium, the primary caregiver provided verbal consent with patients' ascent to treatment.
Measurements
Sociodemographic and medical variables such as age, sex, cancer diagnosis, stage of cancer (localized, metastatic, or terminal), psychiatric diagnosis and past psychiatric diagnosis, history of dementia, presence of brain metastases, and delirium etiologies were collected at the baseline assessment.
Delirium severity was measured with the MDAS, a 10-item, four-point clinician-rated scale (range 0-30)14. MDAS score of >10 identified the presence of delirium15. As proposed by Meagher, the subtyping of delirium was characterized by psychomotor behavior (motoric subtype: hypoactive and hyperactive)16-18. Further scales used were the Karnofsky Performance Status Scale (KPS) indicating physical performance ability19 and an abbreviated version of the UKU (Udvalg for Kliniske Undersogelser) Side Effect Rating Scale20.
Procedures
MDAS and KPS, as well as side effect rating were performed at baseline (T1) and repeated at 2-3 days (T2) and 4-7 days (T3). After seven days the trial ended and patients were continued on the medication as necessary. The standard approach was to treat delirium and continue the necessary medical treatment, including risk factors for delirium such as opiates or corticosteroids; reversible underlying causes such as infection were treated. When the patient showed clear signs of worsening of delirium either clinically or by MDAS scores or could not tolerate the antipsychotic medication, treatment was stopped and another antipsychotic medication initiated.
Statistical Analysis
The data analysis was performed with the SPSS 16 statistical software package for Windows. For the analysis of the complete data set (N = 32 in each group) parametric tests were used: For repeated measures of related samples the ANOVA test, and for comparison of independent samples the t-test were used. For analysis of subsets of the data set with smaller N, in which the data did not show normal distribution, nonparametric tests were used: The Friedman test was used for multiple, related measures, pair wise comparison of independent samples was computed with the Mann-Whitney-U test, for independent categorical variables the Chi-Square test was used. Exact tests were used when possible.
Results
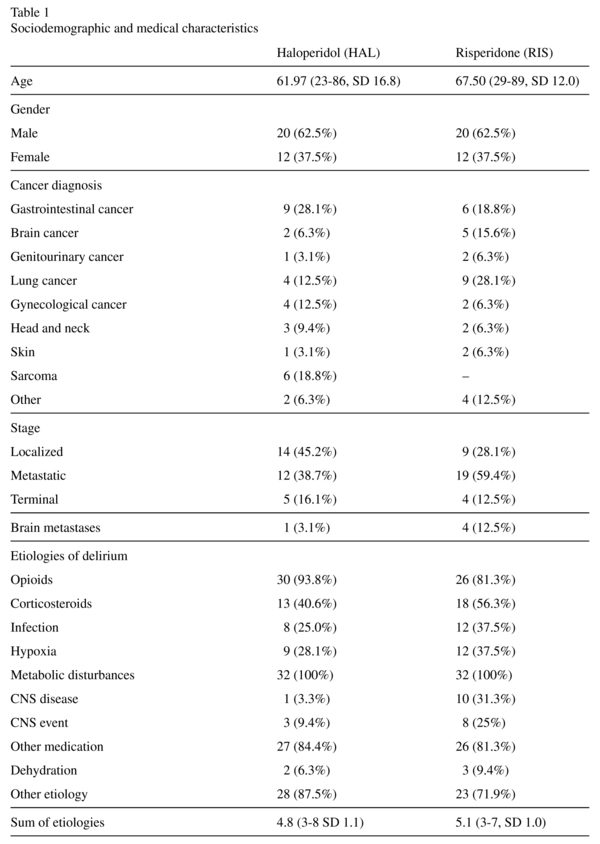
Baseline characteristics of subjects (table 1): We were able to retrieve 32 subjects treated with haloperidol (HAL) and risperidone (RIS) each. There were no significant differences in respect to age, gender, stage of disease, etiologies of delirium and sum of etiologies. The MDAS score at baseline was higher in HAL treated subjects with 20.2 compared to the RIS treated subjects with 17.7 (t-test: t(62) = 2.78, p < 0.05), there was no significant difference in the level of functioning as documented by KPS scores.
Treatment characteristics (table 2): The mean HAL dose at T3 was 4.8 mg (1-16 mg), and 46.9% of patients were treated with HAL until T3. The respective RIS dose was 1.3 mg (0.25-3 mg), and 84.4% of patients received RIS until T3.
Treatment response (table 2): Within each treatment group MDAS scores improved from baseline through T2 to T3 (HAL: 20.2/10.5/7.8, ANOVA: F = 109.69, df = 2, p < 0.001 and RIS: 17.7/11.4/7.5 ANOVA: F = 72.04, df = 2, p < 0.001); at T2 and T3 there were no significant differences between groups. The delirium resolution rates were not significantly different at each measurement point: At T2 the delirium resolution rate was 43.8% in HAL and 37.5% in RIS, at T3 delirium resolution rates were 68.8% and 84.4% respectively.
KPS scores improved within each group from baseline to T2 and T3 (HAL: 22.2/ 27.2/32/2, ANOVA: F = 20.67, df = 2, p < 0.001 and RIS: 24.0/27.5/31.2, ANOVA: F = 23.67, df = 2, p < 0.001); there were no significant differences between HAL and RIS at all observation points.
Side effects: Extrapyramidal side effects (EPS) were the most frequent observed side effect in the HAL treatment group. Parkinsonism was found in 19.0% and dystonia in 9.4%. EPS were usually found at doses of 6 mg and more of HAL. Except for one patient with moderate dystonia, EPS were mild. In the RIS treatment group only one patient (3.1%) experienced EPS in form of mild parkinsonism and mild dystonia.
Treatment in the delirium motoric subtypes (table 2): Subjects with hypoactive delirium received significantly lower doses of HAL throughout all observation points. At T3 they received (3.0 mg (1-6 mg)) compared to 6.5 mg (1.5-16) in subjects with hyperactive delirium (Mann-Whitney U: 52.5, Z = -2.82, p < 0.01). In RIS treated subjects dosing differences existed only at baseline between hypoactive and hyperactive delirium (0.8 mg (0.25-2 mg) and 1.2 mg (0.5-2 mg), Mann-Whitney U: 75.5, Z = -2.12, p < 0.05).
Treatment response in the delirium subtypes (table 2): In subjects with hypoactive delirium MDAS scores improved in both HAL and RIS (HAL: 18.5/11.3/9.3, Friedman: Chi-square 24.12, df = 2, p < 0.001 and RIS: 15.3/10.2/6.6, Friedman: Chi-square 29.12, df = 2, p < 0.001), and there were no significant differences between MDAS scores of HAL and RIS at any observation point. There were no significant differences in respect to delirium resolution rates at T2 or T3: The delirium resolution rates at T2 were 28.6% (HAL) and 43.8% (RIS) and at T3 delirium resolution rates were 64.3% and 91.3% respectively. KPS scores improved in both treatment groups (HAL: Friedman: Chi-square 7.60, df = 2, p < 0.05 and RIS: Friedman: Chi-square 14.86, df = 2, p < 0.01). Between groups there were differences in KPS scores at baseline (19.3 (HAL) and 24.4 (RIS), Mann-Whitney U: 58.50, Z = -2.89, p < 0.01) and T3 (23.6 (HAL) and 32.2 (RIS), Mann-Whitney U: 57.50, Z = -2.86, p < 0.05).
In subjects with hyperactive delirium MDAS scores improved in both treatment groups (HAL: Friedman: Chi-square 33.50, df = 2, p < 0.001 and RIS: Friedman: Chi-square 21.30, df = 2, p < 0.001). Between groups there were no significant differences at baseline, T2 or T3. There was also no significant difference in delirium resolution rates with HAL 55.6% and RIS 31.3% at T2 and 72.2% and 75% at T3 respectively. KPS scores improved in both groups (HAL: Friedman: Chi-square 22.0, df = 2, p < 0.001, and RIS: Friedman: Chi-square 16.55, df = 2, p < 0.01) and there were no significant differences between groups at any time.
Discussion
We were able to confirm previous findings regarding the safety and efficacy of haloperidol and risperidone in the treatment of delirium from a secondary analysis of our delirium database. Similar to previous studies we were not able to find differences in each cohort treated with haloperidol and risperidone. At 48-72 hours the delirium resolution rates were 43.8% in HAL treated patients and 37.5% in RIS treated patients, at T3 delirium resolution rates were 68.8% and 84.4% respectively.
The haloperidol treatment results were similar to Han's findings11 in respect to improvement in MDAS scores and delirium resolution rates: MDAS scores improved from 21.8 to less than 13 and the delirium resolution rate reached 58.3% on day 3 and 75%. The haloperidol dose at 1.71 mg haloperidol was lower than 4.6 mg found in our treatment group. Our risperidone treatment group received similar doses of risperidone (1.3 mg risperidone at the endpoint). The delirium resolution rates were higher than Han's finding with 33.3% at day three and 42% at the end of the study, but similar to the results of other risperidone studies10, 21-23. The MDAS score improved in his RIS group from 23.5 to less than 16, which may explain the lower delirium resolution rate with the delirium resolution cut off score set at 13. Our risperidone treated patients achieved delirium resolution rates of 37.5% at T2 and 84.4% at the endpoint, using a cut-off point of 10 for delirium resolution. In a later study the same authors found in 24 subjects receiving haloperidol and 18 subjects receiving risperidone a decrease in DRS scores from 22.04 to 8.0 (HAL) and 21.61 (RIS) to 9.72, which would be comparable to our results, although a different rating scale, the DRS, was used. The dosing was 1.67 mg and 1.19 mg respectively12.
Side effects in form of EPS occurred more often in the cohort of patients treated with haloperidol. In these patients we found 22.1% EPS treated with an average dose of 4.6 mg haloperidol in comparison to 3.1% occurrence of EPS in the risperidone cohort. The higher rate of EPS in the haloperidol treated patients may be attributable to higher haloperidol doses administered compared to Han's findings with 8% akathisia. EPS In patients who received haloperidol, parkinsonism occurred in 19.0% and dystonia in 9.4%. Patients with hyperactive delirium received significantly higher doses of halo-peridol and experienced EPS with greater frequency. The higher dose of haloperidol in this patient group was deemed to be necessary to maintain the safety of the patient and achieve symptom control. Considering the age of more than 60 years in this patient group24, the rate of EPS may be within expectable limits.
We also examined the motoric subtypes of delirium and found no significant difference in treatment efficacy between haloperidol and risperidone. Of note the haloperidol treated patients with hypoactive delirium had significantly lower KPS score at baseline and T3, which could represent a medically sicker population in the haloperidol cohort, but did not affect the outcome.
Overall our data compares well to the existing haloperidol25-29 and risperidone results10, 21-23. We were not able to show significant differences in treatment response in delirium and its subtypes between haloperidol and risperidone.
Although the data collection has strengths, such as the prospective nature, systematic evaluation of etiology, differentiation between hypoactive and hyperactive delirium, recording of side effects, indication of severity of medical illness through KPS scores, there are important limitations to be noted.
The design was open and investigators were not blinded to the medication. Although the setting was naturalistic and all patients able to comply with delirium assessment were included, the assignment in the trial was not random, resulting in the exclusion of severely agitated, delirious patients, posing immediate danger to themselves or others, very critically ill patients. In the subpopulation of patients with dementia we were not able to assess the baseline cognitive deficits. And finally the number of patients studied was limited to 64.
Further research, particularly double blind, randomly assigned, controlled designs of atypical antipsychotics and typical antipsychotics will be needed to confirm our findings.
In summary we were able to show no difference in efficacy between haloperidol and risperidone in the treatment of delirium and its subtypes. Treatment with haloperidol caused a higher rate of EPS.
Acknowledgments
This trial was not sponsored by a pharmaceutical company. William Breitbart is on the speaker's bureau of and consultant to Cephalon and received grants from the National Cancer Institute (NCI) that did not support this work. Steve Passik is on the speaker's bureau of and consultant to Lilly, Cephalon, King/Ligand, Alpharma, Endo, Purdue-Pharma and received grants from Lilly and Cephalon that did not support this work. Soenke Boettger does not have affiliations to pharmaceutical companies.
References
1. Trzepacz PT, Breitbart W, Franklin J, Levenson J, Martini R, Wang P. Practice Guideline for the treatment of patients with Delirium. American Psychiatric Association. Am J Psychiatry 1999; 156(5 Suppl): 1-20. [ Links ]
2. Bucht G, Gustafson Y, Sandberg O. Epidemiology of Delirium. Dement Geriatr Cogn Disord 1999; 10(5): 315-318. [ Links ]
3. Lipowski ZJ. Delirium in the elderly patient. N Engl J Med 1989; 320(9): 578-582. [ Links ]
4. Bond SM, Neelon VJ, Belyea MJ. Delirium in hospitalized older patients with cancer. Oncol Nurs Forum 2006; 33(6): 1075-1083. [ Links ]
5. Breitbart W, Strout D. Delirium in the terminally ill. Clin Geriatr Med 2000; 16(2): 357-372. [ Links ]
6. Massie MJ, Holland J, Glass E. Delirium in terminally ill cancer patients. Am J Psychiatry 1983; 140(8): 1048-1050. [ Links ]
7. Inouye SK. Delirium in hospitalized older patients. Clin Geriatr Med 1998; 14(4): 745-764. [ Links ]
8. Lonergan E, Britton AM, Luxenberg J, Wyller T. Antipsychotics for Delirium. Cochrane Database Syst Rev 2007; (2): CD005594. [ Links ]
9. Boettger S, Breitbart W. Atypical antipsychotics in the management of delirium: A review of the empirical literature. Palliat Support Care 2005; 3(3): 227-237. [ Links ]
10. Liu CY, Juang YY, Liang HY, Lin NC, Yeh EK. Efficacy of risperidone in treating the hyperactive symptoms of delirium. Int Clin Psychopharmacol 2004; 19(3): 165-168. [ Links ]
11. Han CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004; 45(4): 297-301. [ Links ]
12. Kim JY, Jung IK, Han C, Cho SH, Kim L, Kim SH, et al. Antipsychotics and dopamine transporter gene polymorphisms in delirium patients. Psychiatry Clin Neurosci 2005; 59(2): 183-188. [ Links ]
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000. [ Links ]
14. Breitbart W, Rosenfeld B, Roth A, Smith MJ, Cohen K, Passik S. The Memorial Delirium Assessment Scale. J Pain Symptom Manage 1997; 13(3): 128-137. [ Links ]
15. Lawlor PG, Nekolaichuk C, Gagnon B, Mancini IL, Pereira JL, Bruera ED. Clinical utility, factor analysis, and further validation of the Memorial Delirium Assessment Scale in patients with advanced cancer: Assessing delirium in advanced cancer. Cancer 2000; 88(12): 2859-2867. [ Links ]
16. Meagher DJ, O'Hanlon D, O'Mahony E, Casey PR, Trzepacz PT. Relationship between symptoms and motoric subtype of delirium. J Neuropsychiatry Clin Neurosci 2000; 12(1): 51-56. [ Links ]
17. Meagher D, Moran M, Raju B, Leonard M, Donnelly S, Saunders J, et al. A new data-based motor subtype schema for delirium. J Neuropsychiatry Clin Neurosci 2008; 20(2): 185-193. [ Links ]
18. Meagher DJ, Moran M, Raju B, Gibbons D, Donnelly S, Saunders J, et al. Motor symptoms in 100 patients with delirium versus control subjects: Comparison of subtyping methods. Psychosomatics 2008; 49(4): 300-308. [ Links ]
19. Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents in cancer. In: Mc Leod CM, ed. The evaluation of chemotherapeutic agents. New York: Columbia University Press; 1949. p. 191-205. [ Links ]
20. Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K. The UKU side effect rating scale. A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand Suppl 1987; 334: 1-100. [ Links ]
21. Horikawa N, Yamazaki T, Miyamoto K, Kurosawa A, Oiso H, Matsumoto F, et al. Treatment for delirium with risperidone: Results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003; 25(4): 289-292. [ Links ]
22. Mittal D, Jimerson NA, Neely EP, Johnson WD, Kennedy RE, Torres RA, et al. Risperidone in the treatment of delirium: Results from a prospective open-label trial. J Clin Psychiatry 2004; 65(5): 662-667. [ Links ]
23. Parellada E, Baeza I, de Pablo J, Martinez G. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004; 65(3): 348-353. [ Links ]
24. Uchida H, Kapur S, Mulsant BH, Graff-Guerrero A, Pollock BG, Mam DC. Sensitivity of older patients to antipsychotic motor side effects: A PET Study examining potential mechanisms. Am J Geriatr Psychiatry 2009; 17(3): 255-263. [ Links ]
25. Breitbart W, Marotta R, Platt MM, Weisman H, Derevenco M, Grau C, et al. A double-blind trial of halo-peridol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry 1996; 153(2): 231-237. [ Links ]
26. Platt MM, Breitbart W, Smith M, Marotta R, Weisman H, Jacobsen PB. Efficacy of neuroleptics for hypoactive delirium. J Neuropsychiatry Clin Neurosci 1994; 6(1): 66-67. [ Links ]
27. Schwartz TL, Masand PS. Treatment of delirium with quetiapine. Prim Care Companion. J Clin Psychiatry 2000; 2(1): 10-12. [ Links ]
28. Skrobik YK, Bergeron N, Dumont M, Gottfried SB. Olanzapine vs haloperidol: Treating delirium in a critical care setting. Intensive Care Med 2004; 30(3): 444-449. [ Links ]
29. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics 1998; 39(5): 422-430. [ Links ]
![]() Correspondence:
Correspondence:
Soenke Boettger
Department of Consultation Liaison
Psychiatry and Medical Psychiatry
Bellevue Hospital Center, New York
University Langone Medical Center
462 First Avenue
New York 10016
Tel: 212 562 3536
Fax: 212 562 8985
E-mail: soenkeboettger@yahoo.com
Received: 26 October 2009
Revised: 2 November 2010
Accepted: 18 December 2010

